
{kind=link}
Risk to the patient
SEA typically occurs from hematogenous spread, extension of nearby infection, or from iatrogenic inoculation. Staphylococcus aureus is responsible for the majority of infections [1]. 20% of SEAs occur anterior to the spinal cord. These lesions, which are typically associated with vertebral osteomyelitis, are thought to cause more systemic features which can make the diagnosis more obvious. Unfortunately most (80% of cases) occur in the posterior region, and these patients are less likely to experience systemic symptoms such as a fever [2]. Lesions occur most commonly in the lumbar region, however cervical and thoracic lesions often present atypically, are commonly missed, and account for a disproportionate number of cases that result in a lawsuit.
Overall mortality ranges from 5-34%, down from near 100% at the beginning of the 20th century. About 45% of patients will have a complete recovery, and the majority of patients will have some degree of neurologic compromise [3]. SEA is commonly missed during the patient’s initial visit, causing a delay that can significantly increase the patient’s morbidity. Davis et al. found that about 75% of SEA patients had a delay before imaging was performed, leading to a significant increase in motor weakness with 45% of these patients demonstrating residual weakness compared to 13% who did not have a diagnostic delay [4].
Risk to the provider
Missed SEA is a source of significant medicolegal risk in the United States with an average verdict against the physician of $398,000. Delay in treatment was associated with bad outcomes for both the patient and the provider. In cases where there was a delay of over 48 hours from presentation to surgery, the odds of a plantiff’s verdict increased significantly. In one series, patients with SEA who were initially misdiagnosed and not offered treatment within 48 hours of symptom onset won their cases against the physician 100% of the time [1].
Don’t count on the “classic” symptoms
The “classic triad” of fever, back pain, and neurologic deficits does not accurately identify patients with SEA. In a review of patients with SEA, Davis et al. found that only 13% of patients had this “classic triad” on presentation. The physical exam was also unreliable as 68% of SEA patients had a normal neurologic exam on initial presentation. Findings such as urinary incontinence and perineal parasthesias can significantly increase the likelihood of the patient having a SEA, however lack of these findings does not reliably rule out the disease.
Know who is truly at risk
A wide variety of at-risk conditions include:
- Diabetes mellitus
- IV drug use
- Chronic kidney/liver disease
- Recent spine procedure or indwelling spinal hardware
- Indwelling vascular catheter
- Recent spine fracture
- Immunocompromised status
- Other site of infection
In one study, 98% of patients in the SEA group had at least one of these risk factors compared to 21% of a matched control group with “spine pain” [4].
ESR can help risk stratify high risk patients
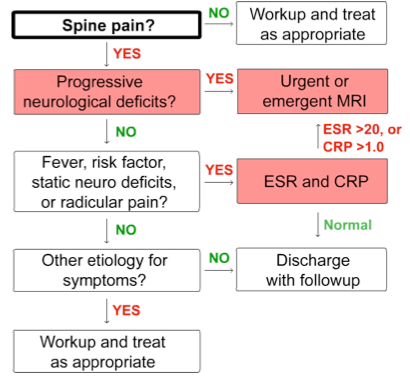
Based on these high risk criteria, Davis et al. developed a clinical decision guideline in an attempt to expedite the workup and diagnosis of SEAs using a combination of high risk features and laboratory tests. In this study, 100% of patients with a SEA had at least one risk factor, with IV drug use being the most common risk factor.
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were ordered for the majority of the patients. The CRP was elevated (>1.0 mg/L) in 87% of SEA patients, but was also elevated in 50% of non-SEA patients who had at least one risk factor. ESR had better test characteristics than CRP and was elevated (>20 mm/hr) in 100% of patients with an abscess compared to 33% of the abscess-free cohort. The combination of one or more clinical risk factors and an elevated ESR was 100% sensitive and 67% specific for SEA. Patients with these positive findings underwent further testing, which was usually MRI [5]. After implementing the guideline, Davis et al. noted a decreased of delays in diagnosis from 84% to 10% (OR 47.7). Similarly motor deficits at the time of diagnosis dropped from 82% to 20% (OR 18.8) [5].
{kind=link}
Is the algorithm ready for prime time?
If all patients with back pain and a clinical risk factor for SEA have an ESR performed, there are going to be a large number of patients who have an elevated level but who ultimately do not have a SEA. The authors did not mention the rate of MRI use after the implementation of the algorithm, but it would be reasonable to assume that if the guideline is followed closely then there would be an increase in the rate of imaging as more patients are identified as being potentially at risk. From a logistical standpoint, most departments would have difficulty obtaining emergent MRIs on all patients with one risk factor for SEA and a mildly elevated ESR.
From a diagnostic standpoint, it would be reasonable to use clinical criteria and ESR in conjunction with overall provider determined pre-test probability. A patient with a history of diabetes with lumbar pain that started after a recent motor vehicle accident has a very low pre-test probability of having a SEA, and contrary to the algorithm needs no further testing. Conversely a patient with fever, IVDA, and unexplained back pain likely needs an MRI, even with a normal ESR. The algorithm proposed by Davis et al. provides an effective means of risk stratification in patients who potentially have a SEA, but given its broad inclusion parameters and poor specificity it should not be used on all patients who present with back pain.
Protect yourself
From a risk management standpoint, the possibility of SEA should be considered and documented in all patients with back pain. A reasonable approach would be to chart:
“I have considered the possibility of SEA, the patient has no features that place them at increased risk of SEA, and they have a normal neurologic exam in the emergency department. I think the pre-test probability of SEA is sufficiently low that they do not need any further workup emergently.”
Patients with no specific risk factors for SEA and a normal exam do not need further testing emergently. In patients with a risk factor, an ESR can be used for further risk stratification. When the ESR is elevated, providers should have a low threshold to obtain imaging.
This post belongs to Dr. Matthew DeLaney’s series on Everyday Risk in Emergency Medicine (EREM).
References
- French KL, Daniels EW, Ahn UM, et al. Medicolegal cases for spinal epidural hematoma and spinal epidural abscess. Orthopedics. 2013;36 (1): 48-53. Pubmed
- Soehle M, Wallenfang T. Spinal epidural abscesses: clinical manifestations, prognostic factors, and outcomes. Neurosurgery. 2002;51 (1): 79-85. Pubmed
- Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev. 2000;23 (4): 175-204. Pubmed
- Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess. J Emerg Med. 2004;26 (3): 285-91. Pubmed
- Davis DP, Salazar A, Chan TC, et al. Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain. J Neurosurg Spine. 2011;14 (6): 765-70. Pubmed
Image (modified)
Author information
The post High risk back pain: Spinal Epidural Abscess appeared first on ALiEM.