
Take Home Points:
- Prioritize ABCs and systematic evaluation of the trauma patient with an open fracture as one third of these patients have multiple injuries
- Assess neurovascular status and immediately reduce and immobilize if compromised
- Give appropriate antibiotics as soon as possible
- Consult orthopedics for operative management as soon as possible
REBEL Core Cast 70.0 – Open Fractures
Click here for Direct Download of the Podcast
DEFINITION:
- Osseous disruption in which a break in the skin and underlying soft tissue communicates directly with the fracture and its hematoma (Egol 2015)
- “Compound fracture” refers to the same entity but is an outdated term
MECHANISM:
- Almost always high-velocity trauma (GSW, MVAs, falls from height)
EPIDEMIOLOGY:
- Of the 3.5-6 million fractures every year in the US, 3% are open (Jedlicka 2012 )
- One third of patients with open fractures have multiple injuries
PHYSICAL EXAM:
- Control hemorrhage
- Direct pressure
- Use tourniquet if patient in extremis and bleeding cannot be controlled with direct pressure.
- Assess neurovascular status- including absent distal pulses, dusky appearance, and impaired motor or sensory function distal to the level of the injury.
-
- Use Doppler if pulses are not palpable
- In 10-20% of significant arterial injuries, distal pulses may be normal
- Perform ABIs for lower extremity injuries if there are signs of vascular compromise
-
- Reduce and splint immediately if neurovascular compromise is present
- Assess for compartment syndrome (present in 9% of open fractures) by looking for severe pain, decreased sensation, pain with passive stretch of fingers or toes
{kind=link}
CLASSIFICATION:
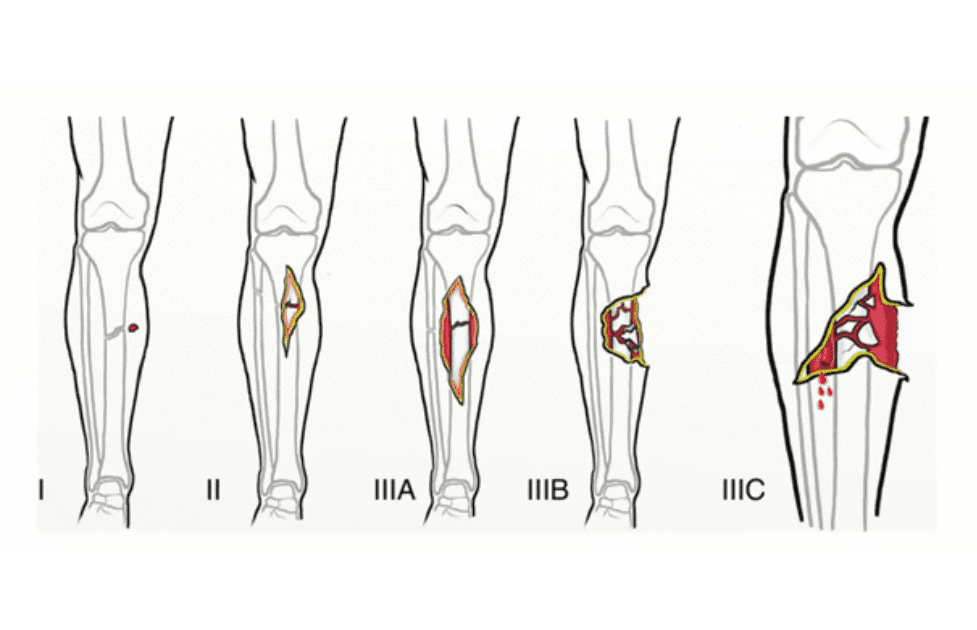
- Gustilo-Anderson Classification: describes open fractures and their risk of infection according to degree of soft tissue injury and contamination
-
- Type I: clean skin opening of <1cm, usually “poke hole” from inside to outside, minimal muscle contusion, often associated with low energy simple spiral or short oblique fractures (0-2% infection risk)
- Type II: laceration >1cm, more extensive soft tissue damage; minimal to moderate crushing component; associated with simple transverse or short oblique fractures with minimal comminution (2-5% infection risk)
- Type III: extensive soft tissue damage including muscles, skin, and neurovascular structures, any high energy injury with severe crushing component
-
- IIIA: extensive soft tissue laceration, adequate bone coverage; segmental fractures, minimal periosteal stripping, high energy traumas regardless of size of wound (crush component, GSW, farm injuries, amputations) (5-10% infection risk)
- IIIB: extensive soft tissue injury with periosteal stripping and bone exposure requiring soft tissue flap closure; usually associated with massive contamination (10-50% infection risk)
- IIIC: same as IIIB but with a vascular injury requiring repair (infection risk 25-50%)
-
- Limitation: Poor interobserver agreement on classification
-
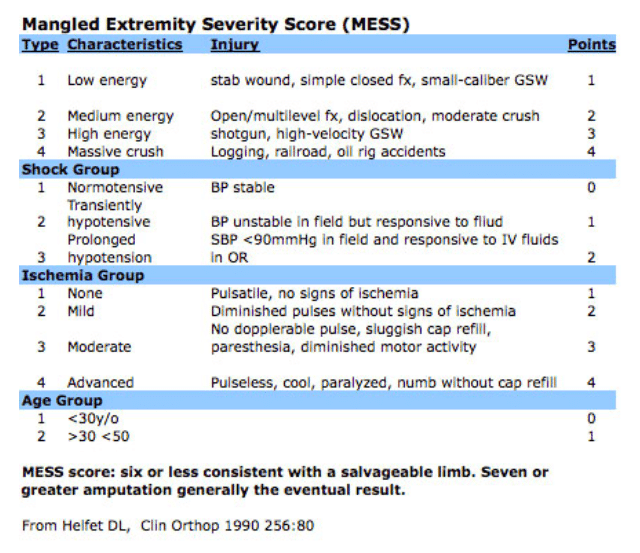
- Mangled Extremity Severity Score (MESS)
-
- Extent of skeletal and soft tissue damage
- Extent and severity of limb ischemia
- Associated shock
- Age
- Note: “mangled” refers to a limb in which three of the four functional components (bone, vessels, nerves, and soft tissue) are injured
-
{kind=link}
IMAGING:
- Obtain X-rays with at least 2 views at 90 degrees to one another
- X-ray the joints above and below the injury
- Visible tracking of air from the wound to the fracture may be visible on X-ray in cases where open fractures are not obvious
- CT of the extremity if intra-articular involvement is suspected to evaluate for air in the intra-articular space
- CTA in cases of suspected vascular injury on exam
ED MANAGEMENT:
- As in all trauma patients, ABCs are the first priority in patient evaluation and must be done prior to assessing fracture
- Immediate administration of antibiotics
-
- IV antibiotics given within 3 hours of injury reduces rate of infection
- Type I and II injuries: 1st generation cephalosporin (i.e. Cefazolin 1g in adults, 25 mg/kg up to 1g in children every 8 hours) (Staph Aureus most common)
- Type III injuries: add an aminoglycoside (i.e. Gentamicin 240mg in adults, 2.5 mg/kg in children one time dose) (added gram negative coverage)
- Farm injuries: add penicillin G or metronidazole to cover Clostridium and other anaerobes
- Seawater contamination: consider adding doxycycline to cover Vibrio species
-
- Pre-debridement wound cultures not found to be helpful in guiding management.
- Tetanus Immunization
-
- If no booster in last 5 years
- Add human tetanus immune globulin for immunocompromised patients, patients that have not had a booster in the last 10 years, and for any wounds suspected to be colonized with C.tetani,
- Provide analgesia
- Consult orthopedics for possible surgical management
- Do not irrigate, debride or probe wound in the ED if immediate operative intervention is planned. This may further contaminate the tissue or force debris deeper into the wound. If there is a delay to operative management, irrigate with saline and cover with a sterile dressing
PROGNOSIS:
- Infection of open fracture may lead to delayed union, non-union, multiple additional surgeries and amputation
- 50% of IIIC injuries result in amputation (Jedlicka 2012 )
TAKE HOME POINTS:
- Prioritize ABCs and systematic evaluation of the trauma patient with an open fracture as one third of these patients have multiple injuries
- Assess neurovascular status and immediately reduce and immobilize if compromised
- Give appropriate antibiotics as soon as possible
- Consult orthopedics for operative management as soon as possible
REFERENCES:
- Adams, J et. al. Rosen’s Emergency Medicine: Concepts and Clinical Practice. Philadelphia: Saunders/Elsevier; 2014: 511-533.
- Egol, KA, et. al. Handbook of Fractures. Philadelphia: Wolter Kluwer; 2015.
- Gustilo, RB, Anderson, JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective. J Bone Joint Surg Am. 1976; 58A: 453-458. PMID: 773941
- Jedlicka, N, et. al. Overview of concepts and treatments in open fractures. Clin. Podiatr Med Surg. 2012: 29(2). PMID: 22424488
- Kanakaris, NK, Giannoudis, PV. “Open Fractures.” Trauma and Orthopaedic Classifications: A Comprehensive Overview, 2014: 487-493.
- Konda SR, Davidovitch RI, Egol, KA. Open knee joint injuries: an evidence-based approach to management. Bull Hosp Jt Dis. 2014;72(1):61-9. PMID: 25150328
- Mauffrey, C, et.al. Acute Management of open fractures: proposal of a new multidisciplinary algorithm. Orthopedics. 2012; 35:10. PMID: 23027477
Shownotes By: Xandra Ortego, MD
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Core Cast 70.0 – Open Fractures appeared first on REBEL EM - Emergency Medicine Blog.