
{kind=link}
Santo Domingo, Republica Dominicana
Octubre 2022
Precio US$190.00 (US$210 Torniquete LTQ 1.0) Al concluir y terminar el curso de forma satisfactoria: Recibirá Certificado de Pared y Carnet, emitidos por la NAEMT
Solo 14 Cupos
30 días de lectura previa
Ejercicios fisicos
1. Lentes seguridad
2. Guantes
3. Botas
4. Casco de Proteccion
5. Pantalon resistente con bolsillos laterales (Tipo militar)
6. Ropa Managas largas
Contacto: Alexander Pacheco
+1 809 849 9295 WhatsApp
eeiird@gmail.com
Director Medico y Coordinador General
{kind=link}
La segunda edición del curso de atención de víctimas de emergencia táctica (TECC) de NAEMT enseña a los profesionales de EMS y otros proveedores prehospitalarios cómo responder y cuidar a los pacientes en un entorno táctico civil.
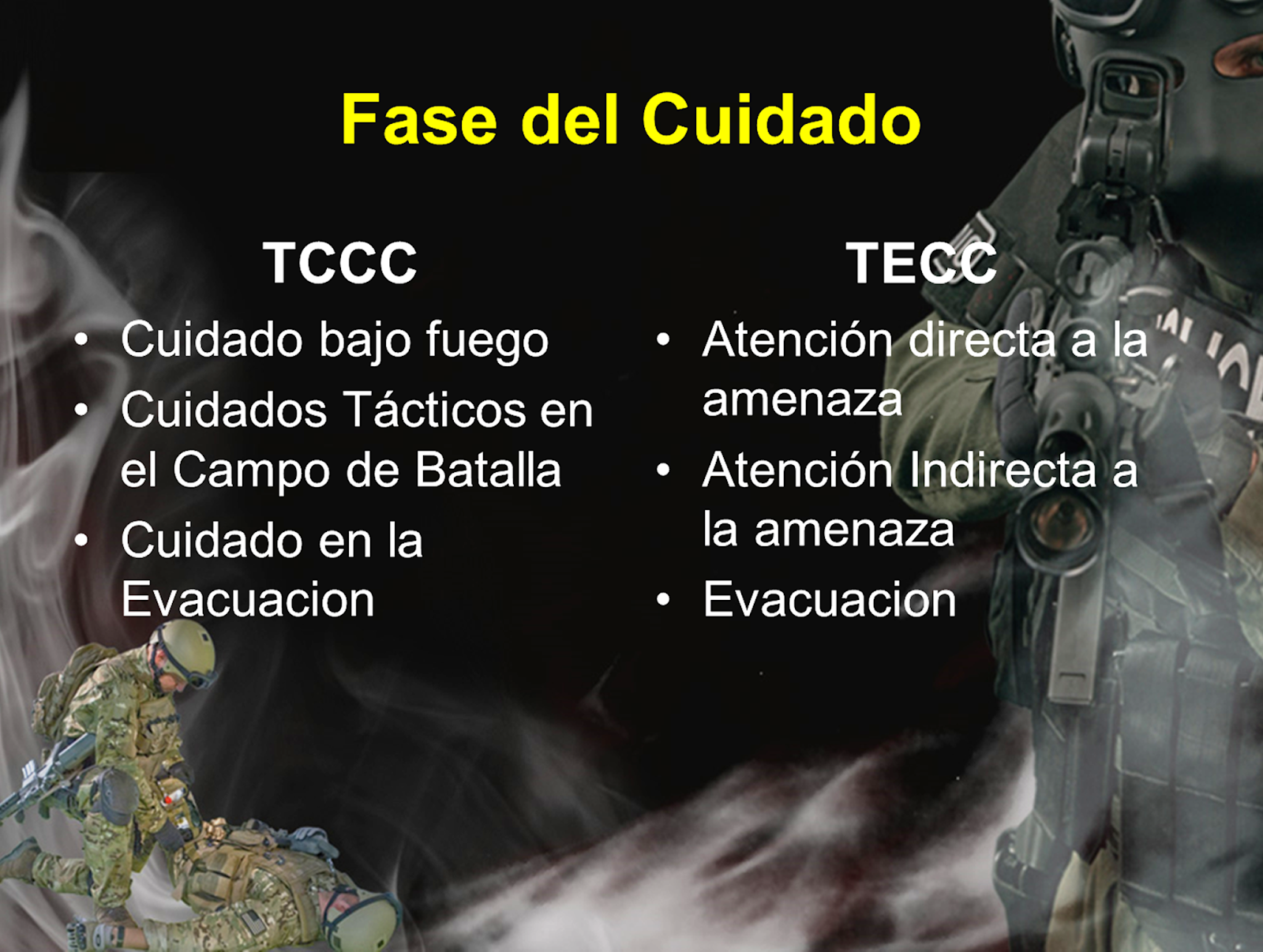
El curso presenta las tres fases del cuidado táctico e integra la nomenclatura paralela de EMS:
Hot Zone/Direct Threat Care que se presta mientras se está bajo ataque o en condiciones adversas.
Warm Zone/Indirect Threat Care que se brinda mientras la amenaza ha sido suprimida pero puede resurgir en cualquier momento.
Zona fría/evacuación Atención que se brinda mientras se evacua a la víctima del lugar del incidente.
El curso presencial de 16 horas incluye todas las simulaciones de pacientes nuevos y cubre los siguientes temas:
Control de hemorragias, incluidos ejercicios de acción inmediata para la aplicación de torniquetes durante todo el curso;
Cobertura completa de la evaluación MARCH;
Control quirúrgico de la vía aérea y descompresión con aguja;
Estrategias para tratar a los socorristas heridos en entornos amenazantes;
Atención de pacientes pediátricos;
Técnicas para arrastrar y llevar a las víctimas a un lugar seguro; y
Una simulación final de evento de tirador activo/víctimas masivas.
El curso TECC de NAEMT cuenta con el respaldo del Comité de Trauma del Colegio Estadounidense de Cirujanos, es consistente con las pautas actuales establecidas por el Comité de TECC (Co-TECC) y cumple con todos los Dominios de Competencia de Apoyo Médico de Emergencia Táctica Nacional actualizados. Este curso está acreditado por CAPCE por 16 horas de crédito de educación continua y reconocido por NREMT.
C-TECCNAEMT es un socio educativo reconocido de Co-TECC. El Co-TECC establece pautas para la prestación de atención prehospitalaria a pacientes lesionados durante un incidente táctico. El Co-TECC no crea currículo para el proveedor prehospitalario, ni respalda el currículo de otras organizaciones.
Este curso examina y aborda los requisitos únicos y desafiantes de administrar atención médica en el lugar del incidente por parte del proveedores Bomberos/Rescatistas/ SEM-EMS a Victimas "pacientes" entorno de alto riesgo (Amenaza).
Los proveedores Bomberos/Rescatistas/ SEM-EMS/Policias aprenderán a distinguir las diferencias entre las intervenciones vitales y las secundarias, y cuándo deben aplicarse en función de la amenaza predominante para los proveedores "socorristas" y los pacientes.
TECC vs TCCC
¿Existen diferencias?
Los equipos de respuesta médica de emergencia y lo de respuesta tácticas y civiles ahora se encuentran en la misma encrucijada en la que se encontraba la comunidad médica de operaciones especiales militares a principios de la década de 1990. La implementación de las pautas de TCCC tal como están escritas en los protocolos civiles tiene los mismos defectos fundamentales que la utilización de los principios civiles de ATLS para el tratamiento de los heridos en combate en el campo de batalla. Esta práctica esencialmente basa la atención médica en una doctrina diseñada para abordar el entorno específico y las restricciones del campo de batalla militar, no el entorno civil.
TCCC está escrito para el médico de combate que opera en un teatro de combate, no para el médico táctico civil que opera en una casa de crack en el centro de Washington, DC. No hay duda de que las armas y las heridas son similares entre los dos escenarios, y no hay duda de que los equipos tácticos federales y civiles están efectivamente en combate. Pero, así como ATLS no abordó muchos de los factores únicos específicos del entorno de combate militar, TCCC no aborda las diferencias en el entorno militar, el proveedor federal o civil y el entorno no militar.
{kind=link}
¿Filosofía?
Como Proveedores de Contenido Educativo Reconocidos por C-TECC, la capacitación brindada por nuestra institucion cumple con los lineamientos de TECC, enseñamos cómo debe ser impartida, de acuerdo con el nivel de habilidad del proveedor. No nos desviamos de los estándares de atención aceptables ni enseñamos nuestra propia versión de las pautas en función de nuestro nivel de comodidad.
Te enseñamos el cómo y el por qué, seguido de la investigación de medicina táctica basada en la evidencia que lo justifica. Le mostramos todos los diferentes tipos de equipos y cómo se aplican mejor. Tenemos numerosos tipos diferentes de torniquetes, vendajes, agentes hemostáticos, camillas, trineos y herramientas de entrenamiento para que los evalúe.
Cada curso incluye tiempo para una revisión completa del equipo, le mostraremos lo que tiene que vale la pena conservar, lo que es basura y lo que necesita comprar.
Este es un "curso médico táctico", no un curso de "correr y disparar" o "entretenimiento educativo", está diseñado para mejorar su conjunto de habilidades médicas. Los cursos que incluyen entrenamiento táctico significativo con fuego real en un formato de 1 o 2 días realmente quitan el componente didáctico médico.
Queremos que comprenda realmente el tema y dedicaremos todo el tiempo que sea necesario para que cada estudiante se vaya con la confianza necesaria para actuar durante un momento de crisis.
Las diferencias que distinguen a TECC de TCCC incluyen, entre otras, las siguientes:
1. El ámbito de la práctica y la responsabilidad:
Los socorristas médicos federales y civiles deben practicar bajo el alcance de la práctica y los protocolos estatales y locales, y están sujetos tanto a la negligencia como a la responsabilidad que el proveedor militar no tiene.
2. Población de pacientes para incluir geriatría y pediatría:
Los datos y la investigación de TCCC se basaron en gran medida en una población de 18 a 30 años, no en todos los grupos de edad representados en las operaciones civiles.
TCCC se escribió principalmente para abordar al combatiente herido y no aborda la atención de alto riesgo para no combatientes inocentes.
3. Distancia, tiempo requerido, recursos disponibles para la evacuación a la atención definitiva
La mayoría de las ciudades civiles tienen múltiples instalaciones médicas definitivas, muchas con centros de Trauma de Nivel 1, dentro de una distancia corta, y los recursos médicos tanto terrestres como aéreos están fácilmente disponibles en la mayoría de los entornos civiles y federales.
4. Diferencias en las barreras de evacuación y atención:
En entornos civiles, hay mucha menos necesidad de preocuparse por ataques secundarios o resistencia armada a la evacuación. En general, una vez fuera de la escena inmediata, se puede asumir la seguridad en el entorno civil.
5. Línea base de salud de la población:
La población de combatientes de TCCC es relativamente saludable y está en buena forma física sin la alta incidencia de enfermedades médicas crónicas que existe en la población civil.
6. Patrones de heridas:
Aunque las armas son similares entre escenarios militares y civiles, los patrones de heridas difieren dada la prevalencia y las diferencias en el equipo balístico de protección, así como el uso y la fuerza de los artefactos explosivos improvisados en el entorno militar.
7. Uso crónico de medicamentos en los lesionados:
TCCC no tiene en cuenta ni aborda los efectos del uso crónico de medicamentos, como los bloqueadores beta y especialmente los anticoagulantes.
Poblaciones especiales, incluidas pacientes embarazadas, discapacitados mentales y físicos.
Las poblaciones especiales prevalecen en el entorno civil y las diferencias requeridas en su atención no deberían ser un ajuste en el campo de batalla.
Adaptamos nuestros cursos a las necesidades específicas
Adaptamos nuestros cursos para satisfacer las necesidades didácticas y prácticas específicas de la unidad que se está capacitando; sin embargo, todos los cursos incluyen variaciones de los siguientes componentes:
.png){kind=link}
Introducción a TECC
Revisión básica de anatomía y fisiología
Las causas evitables de muerte
¿Quién puede usar TECC?
Diferentes aplicaciones TECC
Atención de amenazas directas
Uso de torniquetes y presión directa
Atención de amenazas indirectas
Vendajes de presión
Sellos torácicos y descompresión con aguja
Vías respiratorias nasales y orales
Embalaje de heridas y agentes hemostáticos
Atención de evacuación
Ascensores, Mueve, Lleva
Tratamientos Médicos Adicionales
Revisiones de incidentes y discusiones facilitadas
Tirador activo LAX
discoteca pulso
Incidente del Teatro Aurora
Numerosos ejercicios prácticos
Escenarios Basados en el Ambiente de Trabajo del Estudiante
Entonces, lógicamente, la conclusión de esta página es que la implementación ciega de la doctrina TCCC por parte de los socorristas federales y civiles sin tener en cuenta estas sutiles diferencias dará como resultado una práctica que no será tan efectiva y potencialmente puede ser perjudicial en algunas poblaciones.
De manera similar a lo que hizo TCCC para la atención médica en el entorno de combate militar, los socorristas civiles y federales necesitaban un nuevo paradigma, un marco que definiera el entorno y las limitaciones de recursos, y brindara orientación que permitiera lograr el mejor manejo de pacientes basado en evidencia. la misión de salvar vidas.
Para abordar esta necesidad, se formó un grupo diverso de expertos en primeros auxilios denominado Comité para la Atención Táctica de Emergencias a Víctimas (C-TECC) y, en mayo de 2011, celebró su reunión inaugural para crear las pautas de Atención Táctica de Emergencias a Víctimas (TECC).
Estas pautas TECC, como resultado, son un conjunto de recomendaciones de mejores prácticas para el manejo de víctimas durante operaciones tácticas y de rescate civiles de alta amenaza y el estándar para el apoyo médico de emergencia táctico prehospitalario moderno.
Contáctenos para programar entrenamientos específicos para su equipo, unidad o escuadrón.
+1 809 849 9295
eeiird@gmail.com
Active Bystander Guidelines
Borrador NO OFICAL en Castellano/Español
Ver documento al final en imagenes
¿Qué es C-TECC?
El Comité TECC se convocó originalmente para acelerar la transición de las lecciones médicas militares aprendidas en el campo de batalla a una guía médica operativa basada en evidencia y mejores prácticas para la respuesta médica y el tratamiento de los heridos durante escenarios operativos civiles atípicos y de alto riesgo.
Las pautas de atención de víctimas de emergencia táctica (TECC) son un conjunto de recomendaciones de mejores prácticas para el manejo de víctimas durante las operaciones tácticas y de rescate civiles. Con base en los principios de la atención de heridos en combate táctico (TCCC), TECC tiene en cuenta las diferencias en el entorno civil, los recursos, la población de pacientes y el alcance de la práctica del entorno de combate militar de TCCC. El (C-TECC) sigue el modelo del (CoTCCC) y está compuesto por una amplia gama de líderes académicos y operativos interinstitucionales en la práctica de la medicina de alto riesgo y de incendios/rescate de en todo el país, incluidos miembros de medicina de emergencia, servicios médicos de emergencia, policía, bomberos y la comunidad de operaciones especiales militares. C-TECC sigue siendo una entidad civil independiente pero mantiene una relación cercana con CoTCCC para orientación y apoyo.
Teniendo en cuenta que los patrones de heridas y los mecanismos de las lesiones pueden ser similares en los incidentes civiles que involucran heridas balísticas y explosivas, el TECC recomienda modalidades de tratamiento basadas en la situación y los recursos disponibles. Los objetivos principales de TCCC de adelantar la atención médica oportuna y hacer lo correcto en el momento correcto también son primordiales en las pautas de TECC. Al igual que con TCCC, TECC se divide en tres fases de atención según la relación del proveedor, la víctima y la amenaza.
Se ha invertido una experiencia y un esfuerzo considerables en el desarrollo de un estándar médico operativo civil en paralelo con las pautas exitosas de Atención de heridos en combate táctico. Conocido como Atención táctica de emergencia para heridos, este nuevo estándar utiliza datos y experiencias de las fuerzas armadas y da cuenta de las diferencias de operar en el sector civil. Las pautas de TECC continuarán actualizándose utilizando las mejores prácticas médicas basadas en evidencia y permanecerán bajo la custodia del Comité TECC.
Ver el folleto de descripción general de C-TECC
Objetivos
Los objetivos del TECC incluyen:
Para equilibrar la amenaza, el alcance civil de la práctica, las diferencias en la población civil, las limitaciones del equipo médico y los recursos variables para responder a emergencias atípicas
Establecer un marco que equilibre la relación riesgo/beneficio para toda la respuesta médica operativa civil
Brindar orientación sobre el manejo médico de muertes prevenibles en o cerca del punto de herida.
Para minimizar el riesgo del proveedor mientras se maximiza el beneficio del paciente
Aplicaciones
Las aplicaciones de las directrices TECC para Bomberos/EMS son de gran alcance, más allá de la aplicación tradicional en operaciones tácticas y de aplicación de la ley. La respuesta médica a casi cualquier escenario civil que implique un alto riesgo para los socorristas, entornos austeros o peligros atípicos se beneficiará de las pautas, incluida la respuesta activa de tiradores, eventos relacionados con QBRNE y terrorismo, víctimas masivas, escenarios salvajes/austeros, eventos de rescate técnico y incluso la respuesta traumática tradicional.
The Active Bystander Guidelines have been approved and published by the C-TECC Guidelines Committee and are available at the link below. Updated January of 2020.
The BLS/ALS and First Responders with a Duty to Act Guidelines have been approved and released by the Committee. They are available at the links below. Please update your records accordingly.
- Tactical Emergency Casualty Care Guidelines for First Responders with a Duty to Act (Law Enforcement, Fire fighters, not trained EMS providers)
- Tactical Emergency Casualty Care Guidelines for BLS/ALS Medical Providers
{kind=link}
Borrador Agenda Reunion Comite TECC C-TECC en Washington DC ahi estaremos JuanRa Juan Ramon Viera de España y Dr Ramon REYES, MD...
{kind=link}
Borrador Agenda Reunion Comite TECC C-TECC
en Washington DC ahi estaremos JuanRa Juan Ramon Viera de España y Dr Ramon REYES, MD...
{kind=link}
{kind=link}
1. Massive Hemorrhage / Mask Check (if in place)
A. Address life-threatening hemorrhage first
B. If respiratory protection is present, ensure proper fit/function
2. Airway / Antidote
A. Assess airway
i. Weigh risk / benefit of removing respiratory protection if in place
B. Antidote - If casualty will die before DECON
i. Nerve – ATNAA (1/3) /CANA (1)
ii. Opioid – Naloxone 2mg
iii. Cyanide – Amyl Nitrate
iv. Chlorine/Blister inhalation/TIC – Albuterol
3. Respirations / Rapid DECON
A. Determine if respiratory distress is due to injury or agent
i. Weigh risk / benefit of airway interventions that will compromise respiratory
protection if present
B. Rapid DECON if visible gross contamination or breach in PPE (RSDL)
i. Do not breach PPE / Do not expose any more than necessary
Warm Zone (DECON)
1. Reassess interventions / antidote effectiveness
A. Dirty intervention exchange
2. Countermeasures / Circulation
A. Countermeasures
i. Cyanide - Cyanokit
ii. Nerve – Atropine 2mg q. 3-5 Min
B. Circulation
i. Determine and address route cause
3. Hypothermia management
A. Prevent hypothermia especially during DECON operations
4.EVAC
{kind=link}
TECC vs TCCC ¿Cual es la diferencia?
•TCCC es un curso militar.
–Desarrollado por el CoTCCC
–Focalizado en los peligros en el campo de batalla y en condiciones remotas.
•TCCC el el cuidado estandarizado de trauma en ambientes militares tacticos.
•Usado por:
•Fuerzas Armadas de los EUA
•Mayoria de los naciones aliadas de EUA
•OTAN
•Otros paises alrededor del mundo
•TECC es un curso Civil.
–Basado en las Guias del CoTECC
–Enfocado en los peligros a nivel civil
•TECC provee las guias para el manejo de trauma en ambientes de peligro del tipo tactico civil.
•Enfoque de todos los peligros
•Adoptedo por:
•Agencias Federerales, estatales y fuerzas de seguridad a nivel local en EUA
•Servicio de Bomberos
•Agencias SEM
Los cursos de medicina táctica de la National Association of Emergency Medical Technicians (NAEMT) están diseñados para proveer a los participantes los conocimientos y destrezas para proveer la mejor medicina posible en algunos de los peores escenarios.
La medicina táctica es una de las ramas de lo que se denomina como “medicina operacional”. La medicina operacional consiste en la atención a pacientes bajo circunstancias poco ideales, tales como medicina de desastres, medicina táctica, medicina en lugares remotos, etc. Todas estas ramas tienen el mismo concepto principal: mejorar la sobrevivencia bajo la adversidad. Aunque hay áreas de solape, cada una de las disciplinas tiene una particularidad que la hace especial.
En otras palabras, las circunstancias bajo las cuales se lleva a cabo el cuidado médico es lo que hace especial la medicina operacional.
Cuando hablamos de medicina táctica, el curso Tactical Combat Casualty Care (TCCC) se diferencia al Tactical Emergency Casualty Care (TECC) principalmente en el motivo por el cual los proveedores se encuentran en la zona peligrosa.
El curso TCCC está diseñado para personas cuyo trabajo lo lleva a la zona caliente de combate, mientras que el curso TECC está diseñado para crear una oportunidad para los primeros respondedores para responder a la zona tibia, bajo protección de la policía, para poder llevar a cabo el triage y rescate de las víctimas que tengan posibilidad de sobrevivir.
Ambos cursos están basados en los mismos principios de cuidado bajo fuego (cuidado bajo amenaza directa), cuidado médico táctico (cuidado bajo amenaza indirecta), y evacuación táctica.
Aunque hay mucho en común entre ambos cursos, el curso TECC está más dirigido a los primeros respondedores que están esperando a que la policía entre a una escena peligrosa. Por otro lado, el curso TCCC está diseñado para proveer el cuidado médico dentro de circunstancias en donde los proveedores se ven en la necesidad operacional de entrar a la zona de combate.
{kind=link}
Tactical Emergency Casualty Care (TECC) Guidelines for First Responders with a Duty to Act
Guías para Primeros Respondedores con Deber de Actuar “En Acto de Servicio”
(Fuerzas de Seguridad, Bomberos no SEM)
{kind=link}
Muertes Prevenibles en Combate:
Hemorragia de Extremidades, Neumotorax a Tension y Obstruccion de Vias Aereas.
Cursos tácticos, enfocados en el cuidado básico de víctimas en situaciones de alto riesgo
By John Erich Jan 25, 2016
En la actualidad los disturbios entre la población civil, por causa de francotiradores y tiroteos indiscriminados, están a la orden del día; y las redes sociales pueden crear pánico fácilmente. Todos sabemos que pueden llamarnos para trabajar en situaciones altamente riesgosas. Eso explica la creciente popularidad de los Cursos Tácticos en Atención a Víctimas en Emergencias Médicas.
Pero analicemos el concepto de “situaciones de alto riesgo” un poco más. Las armas y bombas, no son los únicos riesgos para usted o sus pacientes.
“Yo diría,” dice el Dr. E. Reed Smith, Fellow del Colegio Americano de Médicos de Emergencias, Copresidente y Cofundador del Comité de Cuidados Tácticos de Victimas en Emergencias (C-TECC), “que las operaciones diarias de rescate, de un cuerpo de bomberos, también son actividades peligrosas.”
Consideren algo tan común como responder una Colisión de Vehículo Motorizado (CVM) en una autopista muy transitada. Aún con personal capacitado y control de tránsito, se corre el riesgo de que conductores imprudentes atropellen al personal de atención o a las víctimas; enfrenten derrames de gasolina; o incendios, especialmente si son los prime-ros en llegar a la escena del accidente.
“Eso”, dice Smith, quién también es el Director Médico del Departamento de Bomberos del Condado de Arlington en Virginia, “es una escena de alto riesgo. Un riesgo no siempre significa una explosión o una bala, un riesgo puede ser un auto, un derrumbe, un incendio o cualquier situación desconocida. Estos rescates son altamente peligrosos”
Es ahí cuando entra en juego la Atención Táctica de Emergencia de Víctimas. Creado para situaciones de alto riesgo, provee un sistema para balancear el riesgo y el beneficio, limitando el cuidado médico —separando las cosas que se podrían hacer de las que hay que hacer— hasta que la escena se asegure o el paciente esté en un lugar más seguro.
Piense en la medicina militar o en un desastre en una escala menor: En circunstancias atenuantes, el protocolo general puede ser recortado a puntos im-prescindibles simples y rápidos, sólo para preservar la vida en los momentos iniciales.
“Mucho de lo que hacemos es bueno”, dice Smith.” “En un 99% de las veces es bueno comenzar conectando una vía intravenosa”. Pero ¿por qué comenzaría conectando una vía intravenosa en una zona peligrosa de derrumbe, tratando de salvarle la vida a alguien atrapado en el lodo? Eso es muy peligroso. Sin embargo, la medicina tradicional no usa esa estrategia. La medicina tradicional asume que todo está bien. Así que cuando tenemos que trabajar en situaciones poco seguras, como lo hacemos todos los días, es necesario replantear la medicina. Si no salva vidas, entonces debería esperar hasta más tarde.
Componentes Básicos
Una serie de acontecimientos recientes han contribuído a dar más énfasis a este mensaje, se pueden encontrar muchos cursos de tipo TECC en el mercado. Óptimamen-te los departamentos podrían desarrollar su propio curso, basado en sus amenazas, poblaciones y circunstancias. Si eso no resulta práctico, los cursos están disponibles para diferentes industrias y organizaciones privadas, que generalmente se basan en las directrices del Comité TECC, pero no son cursos aprobados oficialmente.
Los procedimientos utilizados para la atención de víctimas en escenarios de alto riesgo son bastante comunes: control de hemorragias, abrir una vía respiratoria, a veces sellar un neumotórax. El impartir conocimientos básicos de trauma no es en realidad lo que los cursos TECC ofrecen. El Comité TECC proporciona los componentes básicos para la estructuración; le toca a los departamentos adoptar y poner en práctica lo que consideren apropiado.
“No necesito mostrar cómo usar un torniquete, usted debe saber por ser un Técnico en Emergencias Médicas Básico”, dice Smith. “La puesta en práctica de las directrices TECC sucede cuando se hacen las cosas. Hacen esto en base a este riesgo.
El cuándo, generalmente se basa en tres fases de la asistencia identificados en la experiencia militar:
Asistencia en amenazas directas:
La asistencia dada bajo ataque o en condiciones adversas;
Asistencia en amenazas indirectas:
Asistencia dada cuando la amenaza ha sido contenida pero que puede volver a resurgir en cualquier momento;
Asistencia en la evacuación
Asistencia dada cuando la víctima está siendo evacuada de la zona del accidente.
Esto coincide con nuestros conceptos de: zonas calientes, tibias y frías.
En la zona caliente: Se corre un alto riesgo de lesión o muerte, así que la asistencia es mínima; deben mantener vivo al paciente y sacarlo de allí.
En la zona tibia: Puede existir una amenaza potencial o indirecta. Una bomba secundaria, que se caiga una estructura inestable, o que ceda una zanja; pero en medio de los riesgos, se pueden llevar a cabo intervenciones adicionales.
En la zona fría: El riesgo es mínimo y se puede prestar una asistencia completa.
“Lo que estamos haciendo es permitir que el proveedor cambie el protocolo basado en el riesgo”, dice Smith: “Si mi percepción del riesgo es del nivel más alto, o no es tan alto, o por el contrario; mi percepción del riego es bajo, entonces puedo usar este conjunto de reglas para determinar el grado de atención.
En general, el TECC es muy simple. Tiene que ver con el momento en que se está haciendo la intervención, con base en lo que está sucediendo a su alrededor; y en como unir la situación operacional con la prioridad de la medicina. Se trata de cómo determinar cuál es la prioridad para cada situación”.
Para conocer más de este tema, visite: http://c-tecc.org.
Nota: Este artículo apareció originalmente en la edición en ingles de la Revista EMS World y fue traducido por un voluntario. Si usted ve errores o quiere sugerir un cambio, favor de avisarnos por correo a editor@emsworld.com.
Traducido por Luis Roberto Yépez Alvarado es Oficial de Bomberos con grado de Capitán, Técnico en Emergencias Médicas Paramédico con un Diplomado en Medicina de Montaña, es Criminalista en Incendios y Explosiones, Coordinador Nacional de PHTLS en Ecuador y Facultado Latinoamericano de TCCC.
{kind=link}
Cadena de Supervivencia TECC by Committee Tactical Emergency Casualty Care
1. Primeros Respondientes: Profesores, Trabajadores, cuidadanos
2. Primeros Respondintes Profesionales en Acto de Servicio ej Bomberos, Policias
3. Cuidado Medico PreHospitalario
4. Departamentos de Emergencias
5. Centros de Trauma
Traducido y adaptado
Miembro Comite TECC
TacMed: We are very privileged to have the secretary of ATMA, Tim Makrides, write us a guest post on the recent winter meeting of the Committee for Tactical Emergency Casualty Care. At the bottom of the post are the replays of the live videos from the meeting. Thanks Tim & ATMA (and of course C-TECC!).
C-TECC MEETING DEBRIEF BY ATMA SECRETARY TIM MAKRIDES
I was recently privileged enough to attend the Committee on Tactical Emergency Casualty Care (C-TECC) winter meeting in California as a representative of the Australian Tactical Medical Association (ATMA) along with ATMA’s President, Matt Pepper.
For those of you who don't know much about ATMA, we are an association formed in mid-2017 with the aim of representing the interests of everyone involved in the provision of first aid or medical care in high threat environments. We carry out our work on behalf of paramedics, doctors, law enforcement officers and even the general public.
While some of the members of the Board of Directors have worked for or currently work for Tacmed Australia, they are two distinct entities, and ATMA is strictly a not for profit organisation.
We are very grateful for the support TacMed has given us, and openly acknowledge that they are one of a few organisations in Australia that have been relentlessly advocating for improved access to tactical medical education and equipment.
Back to the meeting…
We flew over for a very short three-day trip and hit the ground running for the amazing one and half day meeting.
Before I fill you in on the ins and outs of the meeting, it's important to give you a quick run down on who C-TECC are and what they’re trying to achieve (click HERE for the run down).
After arriving very jet lagged but excited we headed in for day one of the meeting.
We started with a presentation from the local Police Chief and Fire Chief who both provided an interesting context into the work being achieved by the committee. It was very evident that this particular County in Southern California was heavily invested in TECC from the ground up. The local police department has trained every officer in bleeding control, and the fire/ EMS Department has one of the strongest tactical medicine programs in the state.
The county was also one the first in the state to co-locate ‘Stop the Bleed’ kits with every defibrillator in a public place. The conference centre alone had three kits.
By mid-morning we heard from the director of the newly formed High Threat Institute, a joint venture involving George Washington University. The institute has recently set up “Go Teams” a highly effective and intriguing concept.
In a nutshell, this newly formed team was created out of a distinct need to learn from major incidents in real or near real time. Go Teams are deployed in the immediate aftermath of a major incident with 2-3 members hitting the ground in the first 24-48 hours. Their job is to link into the local emergency network and talk “offline” with operators involved in the incident. These operators range from paramedics and doctors through to security staff and local law enforcement assets.
While the conversations with responders are informal, the teams are taught to gather and collate specific de-identified data sets. Once the team returns back to their headquarters, the data is translated into an after action report (AAR) and published within a couple of weeks of the incident.
The beauty of this program is that lessons are learned from these incidents much quicker than conventional post incident AAR’s which can often take 2 or so years to publish.
Just before lunch, we heard from Pete Carlo, Assistant Medical Director of Las Vegas Police Department, who briefed us into the Mandalay Bay Shooting in September this year.
The incident was the worst civilian mass shooting in U.S. history and while it was a dark day for everyone involved, the overwhelming body of evidence showed that both EMS and police training before the event ensured a rapid and coordinated response to neutralize the threat and evacuate patients to the local trauma centres.
This presentation raised some interesting questions regarding hospital preparedness for major incidents. C-TECC has recently released ‘First Receiver’ Guidelines which are designed to help hospitals cope with a large number of trauma patients following a major intentional violence incident. There’s a great deal of interesting information available to hospital staff, so if you're an influencer in this space, or just purely interested I urge you to read more about it HERE.
After lunch, ATMA President, Matt Pepper, provided the committee with an introduction to the association, as well as an update on tactical medicine in Australia. The short presentation was very well received with a long list of questions waiting for Matt at the end.
The remainder of the day was spent on working group updates, including:
- First Care Providers
- K9
- First Receivers
- Triage
- Breaching
- Hazmat
- International engagement
Whilst there was a lot of great content covered in the working group updates, it’s far too in-depth to cover on this blog.
The one thing I will quickly mention is that the HAZMAT working group highlighted that there is a very real and likely possibility that fire could be used as part of complex coordinated attacks, as shown by recent ISIS propaganda. The intention is that this will be worked into the guidelines in the future.
The first day wrapped up with a social event at a local bar where many new international friendships were forged over a beer or two.
Day two kicked off bright and early with an animated discussion on the data surrounding head injuries. The C-TECC working group presented a draft of their soon to be released Traumatic Brain Injury (TBI) guideline.
There was a great deal of discussion surrounding the finer detail of the guideline, and a decision was made to re-present the final product at the next meeting in May 2018.
The final topic for the morning was the TECC guidelines for penetrating thoracic trauma and the use of chest seals. The scarce evidence was presented which consists mainly of experimental swine studies. The possibility that covering a wound with a non vented occlusive dressing can consistently cause the development of tension pneumothorax was apparent. The main change to the guidelines will, therefore, be that sucking chest wounds/open pneumothoraces should be covered with a vented seal, and if one is not available, then it should be left uncovered.
This is a significant change for many providers and trainers, and ATMA will be putting out more information on this change over the next few weeks.
The meeting was adjourned around lunchtime, with the Committee sitting again in May 2018 at the Special Operations Medicine Scientific Assembly in Charlotte, NC next year.
Overall the trip was an invaluable experience, and it gives ATMA members and those we inform in Australia a voice and a direct link into the C-TECC. It is the responsibility of ATMA to disseminate this information and to continue to advocate for our member's interests in high threat medical care. We have paved the way for ATMA members to sit on several working groups so if there is something that interests you; please get in touch with me.
Finally, if you’re keen to stay up to date with ATMA then check out our website or social media pages.
Stay safe.
Tim Makrides
Secretary
Australian Tactical Medical Association
email: tim@atma.net.au
website: www.atma.net.au
facebook: www.facebook.com/australiantacticalmedicalassociation
Below are the videos that were live broadcast by the Committee for Tactical Emergency Casualty Care. Thanks to the committee for broadcasting!
{kind=link}
Guidelines Tactical Emergency Casualty Care TECC by CTECC every day getting more space in Europe...
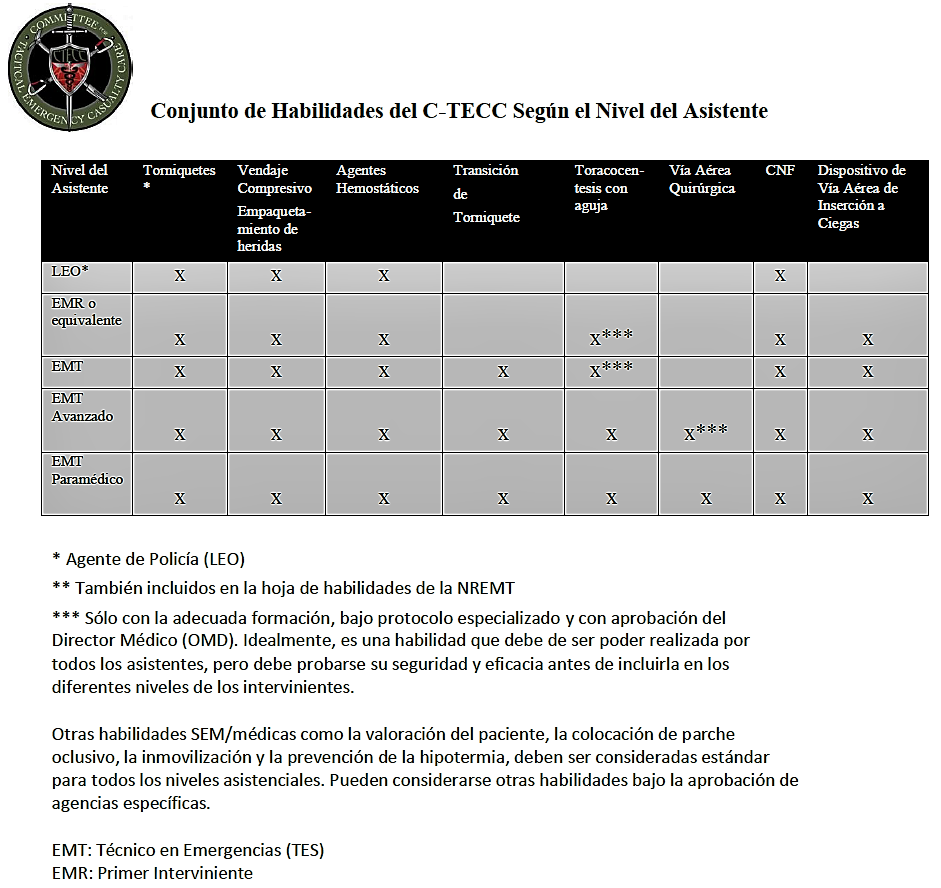
| TECC-NAEMT TACTICAL EMERGENCY CASUALTY CARE. DIRECT THREAT CARE (DTC) / HOT ZONE Guidelines: 1. Mitigate any threat and move to a safer position (e.g. Return fire, utilize less lethal technology, assume an overwhelming force posture, etc.). a. Recognize that threats are dynamic and may be ongoing, requiring continuous threat assessments. 2. Direct the law enforcement/first responder casualty to stay engaged in tactical operation if able and appropriate. 3. Extract casualty to a safer position: a. Instruct the casualty to move to a safer position and apply self-‐aid if capable. b. If the casualty is responsive but cannot move, a rescue plan should be devised and implemented. c. If a casualty is unresponsive, weigh the risks and benefits of an immediate rescue attempt in terms of manpower and likelihood of success. Remote medical assessment techniques for survivability should be considered. 4. Stop life threatening external hemorrhage if present and reasonable depending on the immediate threat, severity of the bleeding and the extraction distance to safety. Consider moving to safety prior to application of the tourniquet if the situation warrants. a. Direct casualty to apply direct pressure to wound and/or own effective tourniquet if able. b. Tourniquet application: i. Apply the tourniquet as high on the limb as possible, including over the clothing if present. ii. Tighten until cessation of bleeding and move to safety. 5. Consider quickly placing unresponsive casualty in recovery position to protect airway. INDIRECT THREAT CARE (ITC) / WARM ZONE Guidelines: 1. Any casualty with a weapon should have that weapon made safe and secured once the threat is neutralized and/or if mental status is altered. 2. Bleeding: a. Assess for and control any unrecognized major bleeding: i. Use a tourniquet or an appropriate pressure dressing with deep wound packing (either plain gauze or, if available, hemostatic dressing to control life-‐ threatening bleeding in an extremity or a junctional area: - Apply the tourniquet over the clothing as proximal-‐-‐ high on the limb-‐-‐ as possible, or if able to fully expose and evaluate the wound, apply directly to the skin at least 2-‐3 inches above wound (DO NOT APPLY OVER THE JOINT). - For any traumatic total or partial amputation, a tourniquet should be applied as high on the extremity as possible regardless of bleeding. b. If available, immediately apply a junctional tourniquet device for anatomic junctional areas where bleeding cannot be easily controlled by direct pressure and hemostatics/dressings. c. Reassess all tourniquets that were hastily applied during Direct Threat/Hot Zone Care. i. Evaluate the wound for continued bleeding or a distal pulse in the extremity. - If there is continued bleeding or a distal pulse is still present, either tighten the existing tourniquet further or apply a second tourniquet, side-‐ by-‐side and, if possible, proximal to the first, to eliminate the distal pulse. d. If possible, mark all tourniquet sites with the time of tourniquet application. 3. Airway Management: a. If the casualty is unconscious or is conscious but unable to follow commands: i. Clear mouth of any foreign bodies (vomit, food, teeth, gum, etc). ii. Apply basic chin lift or jaw thrust maneuver to open airway. iii. Consider placing a nasopharyngeal airway. iv. Place casualty in the recovery position to maintain the open airway. b. If the casualty is conscious and able to follow commands: i. Allow casualty to assume position of comfort, including sitting up. Do not force to lie down. a. All open and/or sucking torso wounds should be treated by immediately applying a vented or non-‐vented occlusive seal to cover the defect. b. Monitor any casualty with penetrating torso trauma for the potential development of a tension pneumothorax. Most common presentation will be penetrating chest injury with subsequent increasing shortness of breath and difficulty breathing and/or increasing anxiety/agitation. i. If tension pneumothorax appears to be developing, removing the occlusive dressing and/or “burp” the chest seal. ii. Casualties with concern for developing tension pneumothorax should be prioritized for evacuation to higher level of care. 5. Shock Management/Resuscitation: a. Assess for hemorrhagic shock i. Altered mental status (in the absence of head injury) and weak or absent peripheral pulses are the best field indicators of shock. b. If not in shock: i. Casualty may drink if conscious, can swallow, and there is a confirmed delay in evacuation to care. c. If in shock: i. Prioritize for rapid evacuation any patient, especially those with penetrating torso injury, displaying signs of shock. 6. Prevention of hypothermia: a. Minimize casualty’s exposure and subsequent heat loss. i. Keep protective gear on or with law enforcement casualty if feasible. ii. Keep casualty warm and dry: - Place the casualty onto an insulated surface to reduce conductive heat loss as soon as possible. - Minimize exposure to the elements. - Replace wet clothing with dry if possible. - Cover casualty with commercial warming device, blankets, poncho liners, sleeping bags, or anything that will retain heat and keep the casualty dry. 7. Reassess casualty: a. Perform a rapid blood sweep, front and back, checking for additional injuries. Tearing, cutting, or otherwise exposing the wound may be necessary. 8. Burns: a. Stop the burning process. b. Cover burns with loose dry dressings if available. c. Large area burns and signs of significant airway burns or smoke inhalation (e.g. singed facial hair, soot/burns/swelling around the nose or mouth) should be prioritized for rapid evacuation. d. Burn patients are more susceptible to hypothermia – minimize heat loss as above. 9. Prepare casualty for movement: a. Consider operational and environmental factors for safe and expeditious evacuation. b. Secure casualty to a movement assist device when available. c. If vertical extraction required, ensure casualty secured appropriately. 10. Communicate with the casualty if possible. a. Encourage, reassure and explain care. a. CPR within this phase of care for victims of blast or penetrating trauma who have no pulse, no ventilations, and no other signs of life will likely not be successful and should not be attempted. b. In other circumstances, performing CPR may be of benefit and may be considered in the context of the operational situation. 12. Documentation of Care: a. Communication of assessments and treatments rendered should be passed along with the casualty to the next level of care. This should be documented on a simple standardized casualty care card with the casualty to the next level of care. EVACUATION CARE (EVAC) / COLD ZONE Guidelines: 1. Reassess all interventions applied in previous phases of care. 2. If multiple wounded, perform primary triage for priority and destination of evacuation to a higher level of care. 3. Airway Management: a. The principles of airway management in Evacuation Care / Cold Zone are similar to that in ITC / Warm Zone. b. If the casualty is unconscious or is conscious but unable to follow commands: i. Clear mouth of any foreign bodies (vomit, food, teeth, gum, etc). ii. Apply basic chin lift or jaw thrust maneuver to open airway. iii. Consider placing a nasopharyngeal airway. iv. Place casualty in the recovery position to maintain the open airway. c. If the casualty is conscious and able to follow commands: i. Allow casualty to assume position of comfort, including sitting up. Do not force to lie down. 4. Breathing: a. All open and/or sucking chest wounds should be treated immediately by applying a vented or non-‐vented occlusive seal to cover the defect. Monitor the casualty for the potential development of a subsequent tension pneumothorax. b. Reassess casualties who have had chest seals applied. Any developing tension pneumothorax should be treated as described in ITC / Warm Zone. c. If available, administration of oxygen may be of benefit for all traumatically injured patients, especially for the following types of casualties: - Chest injuries - Torso injuries associated with shortness of breath - Unconscious or altered mental status - Post-‐blast injuries - Casualty in shock - Casualty at altitude 5. Bleeding: a. Fully expose wounds to reassess for and control any unrecognized major bleeding: i. Use a tourniquet or an appropriate pressure dressing with deep wound packing (either plain gauze or, if available, hemostatic gauze) to control life-‐ - Apply the tourniquet over the clothing as proximal-‐-‐ high on the limb-‐-‐ as possible, or if able to fully expose and evaluate the wound, apply directly to the skin 2-‐3 inches above wound (DO NOT APPLY OVER THE JOINT). - For any traumatic total or partial amputation, a tourniquet should be applied regardless of bleeding. b. If available, immediately apply a junctional tourniquet device for anatomic junctional areas where bleeding cannot be easily controlled by direct pressure and hemostatics/dressings. c. Reassess all tourniquets that were hastily applied during prior phases of care. i. Evaluate the wound for continued bleeding or a distal pulse in the extremity. - If there is continued bleeding or a distal pulse is still present, either tighten the existing tourniquet further or apply a second tourniquet, side-‐ by-‐side and, if possible, proximal to the first, to eliminate the distal pulse. d. Clearly mark all tourniquet sites with the time of tourniquet application. 6. Shock Management/Resuscitation: a. Re-‐assess for developing hemorrhagic shock i. Altered mental status (in the absence of head injury) and weak or absent peripheral pulses are the best field indicators of shock. ii. Utilize additional medical assessment and monitoring equipment that may be available in this phase. b. If not in shock: i. Casualty may drink if conscious, can swallow, and there is a confirmed delay in evacuation to care. ii. Allow casualty to assume position of comfort. c. If in shock: i. Prioritize for rapid evacuation any penetrating torso injury patient displaying signs of shock. ii. Consider alternative methods of transportation to definitive medical care if traditional methods delayed or unavailable. Ensure coordination of patient distribution to avoid overwhelming any one medical receiving facility. d. If altered mental status due to suspected TBI and casualty not in shock, position the casualty supine and raise the casualty’s head to 30 degrees. 7. Prevention of hypothermia: a. Minimize casualty’s exposure and subsequent heat loss. i. Keep protective gear on or with law enforcement casualty if feasible. ii. Keep casualty warm and dry: -‐ Place the casualty onto an insulated surface to reduce conductive heat loss as soon as possible. -‐ Minimize exposure to the elements. -‐ Replace wet clothing with dry if possible. -‐ Cover casualty with commercial warming device, blankets, poncho liners, sleeping bags, or anything that will retain heat and keep the casualty dry. iii. Move into a vehicle or warmed structure if possible. 8. Reassess casualty: a. Complete full front and back re-‐assessment checking for additional injuries. Inspect and dress known wounds that were previously deferred. b. Frequently re-‐check the casualty for any changes in condition. Worsening status at any point should prompt priority evacuation. Consider alternative methods of transportation to definitive medical care if traditional methods delayed or unavailable. Ensure coordination of patient distribution to avoid overwhelming any one medical receiving facility. 9. Burns: a. Stop the burning process. b. Cover burns with loose dry dressings if available. Clean, dry sheets are effective for casualties with large area burns. c. Large area burns and signs of significant airway burns or smoke inhalation (e.g. singed facial hair, soot/burns/swelling around the nose or mouth) should be prioritized for rapid evacuation. Consider alternative methods of transportation to definitive medical care if traditional methods delayed or unavailable. Ensure coordination of patient distribution to avoid overwhelming any one medical receiving facility. d. Burn patients are more susceptible to hypothermia – minimize heat loss as above. 10. Prepare casualty for movement: a. Consider environmental factors for safe and expeditious evacuation. b. Secure casualty to a movement assist device when available. c. If vertical extraction required, ensure casualty secured appropriately. 11. Communicate with the casualty if possible, and with the operational medical provider or medical facility assuming care of the casualty. a. Encourage, reassure and explain care and expectations to patient, family and/or caregivers. b. Notify receiving provider or facility of wounds, patient condition, and treatments applied. 12. Cardiopulmonary resuscitation a. CPR may have a larger role during the evacuation phase especially for patients with electrocution, hypothermia, non-‐traumatic arrest or near drowning. 13. Documentation of Care: a. Continue or initiate documentation of clinical assessments, treatments rendered, and changes in the casualty’s status in accordance with local protocol. b. Forward this information with the casualty to the next level of care. GOALS, PRINCIPLES, SKILL SETS Care provided within the TECC guidelines is inherent upon individual first responder training, available equipment, local medical protocols, and medical director approval. I. Direct Threat Care (DTC)/Hot Zone Primary Goals: 1. Accomplish the mission with minimal additional casualties. 2. Prevent any casualty from sustaining additional injuries. 3. Keep response team maximally engaged in neutralizing the existing threat (e.g. active shooter, barricade, high threat warrant etc.). 4. Minimize public harm. Operational Principles: 1. Establish tactical supremacy and defer in-‐depth medical interventions if engaged in ongoing direct threat mitigation (e.g. active fire fight, dynamic explosive scenario, etc.). 2. Threat mitigation techniques will minimize risk to casualties and the providers. These should include techniques and tools for rapid casualty access and egress. 3. Triage should be deferred to a later phase of care. Prioritization for extraction is based on resources available and the tactical situation. 4. Minimal trauma interventions are warranted during this phase. 5. Consider bleeding control. a. Tourniquet application is the primary “medical” intervention to be considered. b. For response personnel, tourniquet should be readily available and accessible with either hand. DTC/Hot Zone Required Skill Set (applied per approved SOP/protocol only): 1. Direct pressure and hasty tourniquet application a. Consider PACE Methodology-‐ Primary, Alternative, Contingency, Emergency b. Commercially available tourniquets c. Field expedient tourniquets 2. Tactical casualty extraction 3. Rapid placement in recovery position Primary Goals: 1. Goals 1-‐4 as above with DTC / Hot Zone care 2. Stabilize the casualty as required to permit safe extraction to dedicated treatment sector or medical evacuation assets. Operational Principles: 1. Maintain tactical supremacy and complete the overall mission. 2. As applicable, ensure safety of both first responders and casualties by rendering weapons safe and/or rendering any adjunct tactical gear safe for handling (flash bangs, gas canisters, etc). 3. Conduct dedicated patient assessment and initiate appropriate life-‐saving interventions as outlined in the ITC / Warm Zone guidelines. DO NOT DELAY casualty extraction/evacuation for non life-‐saving interventions. 4. Consider establishing a casualty collection point if multiple casualties are encountered. 5. Unless in a fixed casualty collection point, triage in this phase of care should be limited to the following categories: a. Uninjured and/or capable of ambulation or self-‐extraction b. Deceased / expectant c. All others 6. Establish communication with the tactical and/or unified command and request or verify initiation of casualty extraction/evacuation. 7. Prepare casualties for extraction and document care rendered for continuity of care purposes. ITC/Warm Zone Required Skill Set (applied per approved SOP/protocol only): 1. Hemorrhage Control: a. Application of direct pressure b. Application of tourniquet i. Consider PACE Methodology-‐ Primary, Alternative, Contingency, Emergency ii. Commercially available tourniquets iii. Field expedient tourniquets c. Perform wound packing with gauze or hemostatic agent d. Application of pressure dressing 2. Airway: a. Perform Manual Maneuvers (chin lift, jaw thrust, recovery position) b. Insert nasal pharyngeal airway 3. Breathing: a. Application of effective occlusive chest seal b. Apply oxygen c. Recognize the symptoms of tension pneumothorax d. “Burp” occlusive dressing 4. Circulation: a. Recognize the symptoms of hemorrhagic shock a. Apply available materials to prevent heat loss 6. Wound management: a. Initiate basic burn treatment 7. Casualty evacuation: a. Move casualty (drags, carries, lifts) b. Secure casualty to litter 8. Other Skills: a. Monitor casualty b. Recognize need and requirements for, and establish Casualty Collection Point. Primary Goals: 1. Maintain any lifesaving interventions applied during DTC and ITC phases. 2. Provide rapid and secure evacuation to an appropriate medical receiving facility. 3. Provide good communication and patient care data between field medical providers and fixed receiving facility. 4. Avoid additional preventable causes of death. Operational Principles: 1. Reassess the casualty or casualties for efficacy of all applied medical interventions. 2. Utilize a triage system/criteria per local policy that considers priority AND destination to ensure proper distribution of patients. 3. Utilize additional available resources to maximize advanced care. 4. Avoid hypothermia. 5. Communication is critical, especially between tactical elements and non-‐tactical EMS teams. 6. Maintain situational awareness: in dynamic events, there are NO threat free areas. Evac/Cold Zone Required Skill Set (applied per approved SOP/protocol only): 1. Same as ITC/Warm Zone 2. Apply triage prioritization of casualties 3. Communicate effectively between non-‐medical, pre-‐hospital and hospital medical assets There is no official or national certification in TECC. There is no official designation as a TECC instructor. The Committee maintains the belief that the guidelines are the evidenced based 'what to do' and 'why to do it.' The 'how' is up to you, and that planning and training should occur on an local/agency level. So, take the guidelines and create your own training. However, if you can't, be sure to chose a training entity that displays the CTECC recognized educational content logo. This means the training adheres to the Committee's educational principles. No existe una certificación oficial o nacional en tecc. No hay designación oficial como instructor de tecc. El Comité mantiene la creencia de que las directrices son las que se basan en " qué hacer " y " por qué hacerlo " el " Cómo " depende de ti, y que la planificación y la formación deben tener lugar a nivel local o de la agencia. Así que, toma las directrices y crea tu propio entrenamiento. Sin embargo, si no puedes, asegúrate de elegir una entidad de entrenamiento que muestre el logotipo de contenido educativo reconocido por ctecc. Esto significa que la formación se atiene a los principios educativos del comité. Introduction to Tactical Emergency Casualty Care (TECC) FEMA Introduction TECC Tactical Emergency Casualty Care Course with Certificate First you must get the FEMA SID Number in this link https://cdp.dhs.gov/femasid/register This course represents the foundational curriculum in a series of courses sponsored by the Federal Emergency Management Agency’s, National Training and Education Division, developed by The George Washington University and its partners. It is designed for all levels of providers: citizens who become a first care provider, police officers, fire and EMS professionals, hospital based first receivers and all those comprised in the TECC Chain of Survival. This course provides an overview of civilian high threat medical principles that can be applied by all first care and medical providers during active acts of violence and intentional mass casualty events, such as an active shooter, detonation of explosives, or use of fire as a weapon. The goal is to better prepare our nation’s communities to respond to atypical incidents that involve mass-casualties and preserve life. The training challenges some long-standing principles of emergency response, and establishes a platform from which to build additional knowledge and skills. Completion of this introductory course is required prior to participating in any of the other courses specifically designed for your role as a first responder. All other courses in this series are delivered in person, are based on your experience and professional scope of practice, and include practical hands on skills practice. For information about additional FEMA training, visit www.training.fema.gov. Christian Goring, Dr. Luis Perez-Bolde, MD, Dr. Ramon REYES, MD Presentacion realidad Iberoamericana de la MEDICINA TACTICA Reunion Comite TECC Dr. Reed Smith, MD Chair CTECC y Dr. Ramon REYES, MD Reunion Comite TECC Australia, Mexico, Chile, Dominicana, España Reunion Comite TECC Comite Iberoamericano de Medicina Tactica Reunion Comite TECC |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Curso TECC Tactical Emergency Casualty Care by CoTECC
Parte de las acciones formativas del Grupo de Trabajo en Medicina Tactica de SEMES Andalucia.
Enseña a los Servicios Medicos Civiles SEMs, a trabajar en conjunto a las Fuerzas de Seguridad del Estado. Dirigido a todos los actores en situaciones TACTICAS (Tiradores Activos, Bombas, Ataques Terroristas). No es un curso en donde se enseña a ser un SWAT, o Personal Tactico (Equipos de Contacto encargados de neutralizar las Amenazas) Se enseña Como Trabajar en la Fase posterior a la entrada en escena de los equipos de contacto, digase en la Fase de Rescate, practicando Maniobras en la medida de lo posible que permitan salvar la vida de las victimas y proceder a la Extricacion y Evacuacion de Heridos en las mejores de las condiciones posibles. Dirigido a TES, DUEs, Medicos, Bomberos, Personal de Proteccion Civil, etc.
El Director Medico con Experiencia Militar, Policial SWAT en EUA, ha trabajado en conflictos en Irak, Mali, Mauritania, etc. es Facultado Internacional TCCC-PHTLS-TECC y Autorizado por escrito para Impartir TCC-LEFR por el propietario del curso Dr. Peter Pons (Unico en España) y se dedica a la medicina de alto riesgo a nivel internacional. Es miembro del SOMA Special Operations Medical Association ID 17479 y Miembro Sociedad Europea de Medicina de Emergencias EUSEM.
Curso TECC TACTICAL EMERGENCY CASUALTY CARE
{kind=link}
Reunion de Trabajo "GRUPO MEDICINA TACTICA SEMES ANDALUCIA"
{kind=link}
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Localizacion de nuestro centro de entrenamiento
{kind=link}
More information in the link http://emssolutionsint.blogspot.com.es/2016/07/phtls-founder-and-medical-director.html
Faculty TCCC /TECC /
Especialista de Medicina de Alto Riesgo a Nivel Internacional
El Comité del Tactical Emergency Casualty Care (C-TECC), un grupo de voluntarios expertos en materias médicas operacionales civiles, publicó en el año 2011 sus primeras directrices reflejando el concepto IPA/FCP. El proceso de creación y las directrices del C-TECC se basaron en las exitosas directrices militares del Tactical Combat Casualty Care (TCCC) y fueron modificadas para ajustarse a los aspectos únicos de la respuesta en escenarios civiles con amenaza elevada. En el ámbito militar, el TCCC tuvo más éxito en la reducción de la tasa de mortalidad cuando se establecía como parte de un sistema de tratamiento de heridos de manera integral, como el Sistema de Primer Interviniente de los Rangers (Ranger First Responder). Sin embargo, existen grandes diferencias entre las respuestas a nivel operativo civiles y las militares: las peculiaridades de los pacientes de la población civil, las restricciones legales y las diferencias en cuanto a logística y recursos, impiden la aplicación directa del TCCC en las operaciones civiles. Las directrices del TECC tienen en cuenta esos aspectos únicos para la actuación en estos escenarios con nivel de amenaza elevada y, permiten a las autoridades locales, implementar de manera adecuada los programas de respuesta en este tipo de incidentes con heridos que involucren “a toda la comunidad”.
| About Tactical Emergency Casualty Care (TECC) What is Tactical Emergency Casualty Care? Tactical Emergency Casualty Care (TECC) is a set of best practice treatment guidelines for trauma care in the high-threat prehospital environment. These guidelines are built upon critical medical lessons learned by US and allied military forces over the past 15 years of conflict. They are appropriately modified to address the specific needs of civilian populations and civilian EMS practice. The guidelines are freely available to all interested stakeholders via the Committee for TECC website - www.c-tecc.org How did the TECC guidelines come about? The Committee for Tactical Emergency Casualty Care (C-TECC) was formed in 2010 to formally translate military trauma lessons learned into the civilian high threat prehospital community. The C-TECC is modeled after the highly successful Committee on Tactical Combat Casualty Care (CoTCCC) - frequently credited as one of the major initiatives that has resulted in the lowest combat mortality rates in recorded history. C-TECC brings together SME's from EMS, fire, law reinforcement and federal emergency bodies, as well as physicians from emergency departments, trauma centers and the military to develop evidence-based principles of high threat prehospital medicine. What does TECC address that other guidelines do not? The TECC guidelines take into account the requirement of a civilian population. This includes paediatric, geriatric and special needs patients, as well as considerations for underlying medical conditions common in a civilian population (i.e. regular anti-platelet use), the characteristics and limitations of civilian EMS, and the varied types of threats that responders face. Military treatment guidelines were developed for a very specific purpose and population - fit healthy 18-40 year olds in a combat environment. They have been extremely successful, but these guidelines cannot be directly carried over into the civilian population without taking these differences into account. How can I find out more? To find out more, visit the website of the Committee for Tactical Emergency Casualty Care - www.c-tecc.org |
{kind=link}
{kind=link}
Comite Ejecutivo TECC
Co-Operating Chair
Reed Smith, MD
Arlington County Fire Department
Co-Operating Chair
David Callaway, MD
Carolinas Medical Center
Secretary
Brendan Hartford, EMT
Chicago SWAT
Treasurer
Geoff Shapiro, EMT-P
George Washington University
At-Large
Sean McKay, EMT-P
Clearwater Fire and Rescue
Reed Smith, MD
Arlington County Fire Department
Co-Operating Chair
David Callaway, MD
Carolinas Medical Center
Secretary
Brendan Hartford, EMT
Chicago SWAT
Treasurer
Geoff Shapiro, EMT-P
George Washington University
At-Large
Sean McKay, EMT-P
Clearwater Fire and Rescue
Junta Directiva TECC
Chief Skip Kirkwood
Wake County EMS Division
Chief James Schwartz
Arlington County Fire Department
Babak Sarani, MD
George Washington University Medical Faculty Associates
Rick Mathews
National Center for Security and Prepredness
David Davis, EMT-P
DHS
Nelson Tang, MD
Johns Hopkins University
Wake County EMS Division
Chief James Schwartz
Arlington County Fire Department
Babak Sarani, MD
George Washington University Medical Faculty Associates
Rick Mathews
National Center for Security and Prepredness
David Davis, EMT-P
DHS
Nelson Tang, MD
Johns Hopkins University
Comite de Directrices
Mark Gibbons, EMT-P
Maryland State Police
John Gandy, MD
US Air Force
Matthew Sztajnkrycer, MD
Mayo Clinic
Jeff Cain, MD
Emergency Medicine
Michael Marino, EMT-P
Prince George Fire Department
David Tan, MD
Washington University
Mark Anderson, EMT-P
Seattle/King County Medic One
Capt. John Delaney, EMT
Arlington County Fire Department
Scott Weir, MD
Fairfax County Fire Department
Keith Monosky, PhD
Central Washington University
Jeff Lindsey, PhD
24-7 EMS Training
William Bozeman, MD
Wake Forest University
Joshua Bobko, MD
Loma Linda University
Barry Frasier, EMT-P
US Air Force
Tom Burnett, MD
Virginia Polytechnical Institute
Mike Shertz, MD
Oregon Emergency Physicians
Rich Kamin, MD
State of Connecticut Department of Public Health
Jason Pickett, MD
Wright State University Dept. of Emergency Medicine
Russ Kotwall, MD
US Army, Joint Trauma System Division Director for Trauma Care Delivery
Chief Robert Wylie, EMT
Cottleville Community Fire Protection District
Scott Kimball, EMT-P
Special Operations Group, US Marshall's Service
Vincent Johnson, EMT-P
Fire Department of NY
Eileen Bulgar, MD
Harborview Medical Center
Ofer Lichtman, EMT-P
Rancho Cucamonga Fire District
Gina Piazza, DO
SUNY at Buffalo
Liaison Positions:
Maryland State Police
John Gandy, MD
US Air Force
Matthew Sztajnkrycer, MD
Mayo Clinic
Jeff Cain, MD
Emergency Medicine
Michael Marino, EMT-P
Prince George Fire Department
David Tan, MD
Washington University
Mark Anderson, EMT-P
Seattle/King County Medic One
Capt. John Delaney, EMT
Arlington County Fire Department
Scott Weir, MD
Fairfax County Fire Department
Keith Monosky, PhD
Central Washington University
Jeff Lindsey, PhD
24-7 EMS Training
William Bozeman, MD
Wake Forest University
Joshua Bobko, MD
Loma Linda University
Barry Frasier, EMT-P
US Air Force
Tom Burnett, MD
Virginia Polytechnical Institute
Mike Shertz, MD
Oregon Emergency Physicians
Rich Kamin, MD
State of Connecticut Department of Public Health
Jason Pickett, MD
Wright State University Dept. of Emergency Medicine
Russ Kotwall, MD
US Army, Joint Trauma System Division Director for Trauma Care Delivery
Chief Robert Wylie, EMT
Cottleville Community Fire Protection District
Scott Kimball, EMT-P
Special Operations Group, US Marshall's Service
Vincent Johnson, EMT-P
Fire Department of NY
Eileen Bulgar, MD
Harborview Medical Center
Ofer Lichtman, EMT-P
Rancho Cucamonga Fire District
Gina Piazza, DO
SUNY at Buffalo
Junta de Asesores
- CAPT (R) Frank Butler, MD, Chair Committee for Tactical Combat Casualty Care
- Thomas Scalea, MD, R. Cawley Shock Trauma
- Roger Band, MD, University of Penn
- Daniel Fagbuyi, MD, Children's National Medical Center
- William Gephart, PA-C, US Army Special Operations
- Paul Pepe, MD, University of Texas Southwestern
- John Freese, MD, Fire Department of New York City
- Brent Myers, MD, Wake County EMS
- Gary Kibbee, EMT-P, South San Francisco Fire Dept
- Jose Henao, MD, US Navy
- Alex Eastman, MD, Dallas Police Department
- Mel Otten, MD, Cincinnati SWAT
- Crawford Mechem, MD, University of Pennsylvania
- Rick Hammesfahr, MD, Marietta GA SWAT
- Lawrence Heiskel, MD, International School of Tactical Medicine
- James McGinnis, PA-C, Health Intervention and Disaster Response, George Washington University
- David Slattery, MD, Las Vegas Fire and Rescue
- Chief Michael Touchstone, Philadelphia Fire Department
- SGT James Gordon, Los Angeles Police Department
- Scott Sasser, MD, Emory University
- Alex Isakov, MD, Emory University
- John Armstrong, MD, Florida State Surgeon General and Secretary of Department of Health
- Duane Caneva, MD, Customs and Border Protection
- Peter Carlo, PA-C, Las Vegas SWAT
- COL Isaac Ashkenazi, MD Retired, Israeli Defense Forces
- Allen Yee, MD, Chesterfield Fire Department
- Darryl Stroud, Special Operations Group, London Fire Brigade
- LT Tracy Frazzano, Township of Montclair Police Department
- Cory Slovis, MD, Vanderbilt University Medical Center
- Don Jenkins, MD, Trauma Center, Mayo Clinic
- Kevin Gerold, MD, TEMS Section, NTOA
- Carol Cunningham, MD, Ohio Department of Public Safety, Division on EMS
- August Vernon Forsyth, County Emergency Management
- Glenn Bollard, MD, Gallatin County SRT
- Steve Giebner, MD, Committee for Tactical Combat Casualty Care
- Howard Champion, MD, University of Maryland
- Stuart Thomas – Director, Line9Medic Ltd UK
- Matthew Wentzel , Psy.D, M.Ed - Blue Pearl Consulting
- Kristina Anderson, KOSHKA Foundation for Safe Schools
- Detective Eric Soderlund, Pinellas County Sheriff's Department
- Terry Nichols, ALERRT, Texas State University
- Captain Christopher Baldini, Philadelphia Fire Department
- Lee Palmer, DVM, K9 Medic, Oregon State University
- Nate Hiner, EMT-P, Arlington County Fire Department
- Denis Fitzgerald, MD, CONTOMS
- Greg Smith, EMT-P, CONTOMS
- Andre Pennardt, MD, National TEMS Initiative and Council
- Todd Baldridge, EMT-P, Orange County Fire Authority
- Carol Cunningham, MD, Ohio Department of Public Safety, Division of EMS
Liaison Positions:
- DHS/FBI/NCTC Joint Counter Terrorism Awareness Workshop Series Liaison
- Coalition for Tactical Medicine Liaison
- National TEMS Initiative and Council Liaison
- International Trauma Life Support Liaison
- PreHospital Trauma Life Support Liaisonls Liason
- Koshka Foundation for Safe Schoo
Videos Ejemplos de habilidades practicadas en el Curso
{kind=link}
¿Como actuar ante tiradores Activos? Corra- Escondase-Pelee
RUN HIDE FIGHT
Bleeding Control Basic by American College of Surgeons and The Hartford Consensus IV StopTheBleed "Stop the Bleed" http://emssolutionsint.blogspot.com.es/2016/07/the-hartford-consensus-iv-compendium.html
#trauma #phtls #terrorismo #explosion #tecc #tccc #ems #sem #emergencias #urgencias #tiradoractivo #semes #eate #ctecc #cotccc #ambulancias #BCon #hartford #StopTheBleed #BleedingControl #hemorragia #sangrado #torniquete #SAMXT #CAT #EmpaquetamientoHeridas #hemostasia #viasaereas
Hola y saludos desde Nueva Orleans, Soy el Dr. Lance Stuke Director Medico PHTLS y miembro del Comite de Trauma del Colegio Americano de Cirujanos. Quiero extender mis felicitaciones al Grupo de Trabajo Tactico de la Sociedad Española de Medicina de Urgencias y Emergencias. SEMES, quienes estaran entrenando en Control de Sangrados y Manejo de Multiples Victimas en Situaciones Tacticas, adicionalmente quiero dar las gracias al Dr. Ramon Reyes por su liderazgo para brndar este curso a cada uno de ustedes, en el mundo en que vivimos multiples victimas, vienen haciendose mas y mas comun, y estos entrenamientos son valiosos al proveer estandares de calidad para la comunidad y y finalmente a nuestros pacientes. Gracias por su dedicacion, espero a conocerlos a todos en el futuro"
Dr. Lance Stuke
PHTLS Medical Director
{kind=link}
Curso T.E.C.C. TACTICAL EMERGENCY CASUALTY CARE . ESPAÑA
El Curso es endosado por el Comite TECC de los Esatados Unidos y tenemos autorizacion escrita para utilizar material y logos del C-TECC.
{kind=link}
Curso Cardioprotegido por
Emergency Educational Training Institute https://www.eeti.training/ |
{kind=link}
International EMS Registry
{kind=link}
http://www.iemsr.org/the-board.html
Emergency Educational Training Institute
Florida USA
Cómo actuar ante un incidente terrorista
Si te ves involucrado en un incidente terrorista, sigue los consejos que te ofrecemos desde #DivulgaSEMES y el Grupo de Enfermería Militar de SEMES:
ANTES DEL INCIDENTE
- Conoce el lugar en el que estás y busca al menos 2 salidas para caso de emergencia.
- Reconoce los lugares en los que podrías quedar atrapado en caso de salida.
- Identifica posibles lugares en los que refugiarte si fuera necesario.
- Notifica lo antes posible a la policía si observas alguna actitud extraña (alguien con un cuchillo/arma)
DURANTE EL INCIDENTE
HUYE:
- No siembres el pánico e intenta mantener la calma.
- Dirígete con decisión al lugar de salida/ huida que habías identificado.
- No te dirijas hacia la persona que está produciendo el tumulto.
- Intenta tranquilizar a los que están alrededor tuyo y abandonar la escena.
- No corras si no tienes espacio para ello, puedes crear avalanchas.
- Deja en el lugar tus pertenencias si suponen un lastre para huir.
- No te pares a grabar fotos ni vídeos.
- No te pares a atender heridos.
- No te enfrentes.
- Ponte en lugar cubierto lo antes posible.
Si no puedes huir, trata de ocultarte.
ESCÓNDETE:
- Mantente oculto.
- Manténgase en silencio.
- Esté en disposición de pelear.
- Intenta esconderte en lugar cerrado y bloquea la puerta.
- Silencia tu teléfono móvil y quita todas las fuentes de ruido.
SI no puedes huir ni esconderte,
PELEA (esta es la última opción):
- Actúa con agresividad.
- Utiliza cualquier objeto de fortuna para golpear.
- Pide ayuda y ataca en grupo.
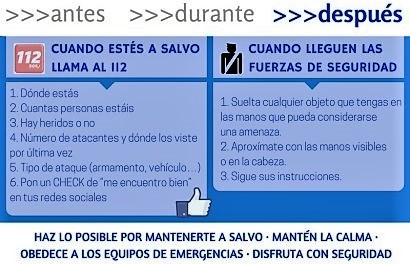
DESPUÉS DEL INCIDENTE
CUANDO ESTÉS A SALVO, LLAME AL 112 Y DE INFORMACIÓN AL OPERADOR.
- Dónde estás
- Cuantas personas estáis.
- Hay heridos o no
- Número de atacantes y dónde los viste por última vez.
- Tipo de ataque, (armamento, vehículo…).
- Cualquier dato que consideres relevante.
- Pon un CHECK de “me encuentro bien” en tus redes sociales
CUANDO LLEGUEN LAS FUERZAS DE SEGURIDAD:
- Suelte cualquier objeto que tenga en sus manos que pueda considerarse una amenaza.
- Aproxímese con las manos visibles o en la cabeza.
- Siga sus instrucciones.
Y recuerda:
- HAZ LO POSIBLE POR MANTENERTE A SALVO
- MANTEN LA CALMA
- OBEDECE A LOS EQUIPOS DE EMERGENCIAS
- DISFRUTA CON SEGURIDAD
{kind=link}
GUIA PARA LE MANEJO DE HERIDOS EN INCIDENTES
INTENCIONADOS CON MULTIPLES VICTIMAS Y TIRADORES ACTIVOS
GUIA M.A.C.T.A.C. Actualizacion 2017
Tamaño del archivo en PDF Gratis
2.34 MB
21 Paginas
Este obra cuyo autor es JUAN JOSE PAJUELO CASTRO Y JOSE CARLOS MENESES PARDO está bajo una licencia de Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional de Creative Commons.
{kind=link}
GUIA DE SOPORTE VITAL EN INCIDENTES CON AMENAZA ELEVADA PARA PRIMER INTERVINIENTE POLICIAL by Juan Jose Pajuelo. España 2017
Descargate la guia: Guía para Primer Interviniente Policial
El objetivo de estas Guías no es otro que resumir de manera breve y concisa los pasos ideales (en ocasiones lo ideal no es lo real) para una valoración y manejo iniciales de las principales causa de muerte evitable, hasta la llegada de los Servicios de Emergencia, en los compañeros o ciudadanos heridos.
Se pretende que estas Guías aborden la asistencia inicial, en el contexto de una intervención o incidente donde exista un alto nivel de amenaza, en el que se vean involucrados los “policías de a pie”, puesto que ha quedado demostrado que son los primeros (y en ocasiones los únicos) en abordar inicialmente tanto al incidente en sí mismo, como a las víctimas si se han producido.
Un incidente con alto nivel de amenaza no se limita a sucesos como atentados terroristas con múltiples víctimas, si no que contempla también otro tipo de circunstancias como incidentes con individuos armados y/o, aglomeraciones populares con individuos violentos.
Toman como referencia las Directrices para Primeros Intervinientes con la Obligación de Asistir (First Responders with a Duty to Act) del Comité del Tactical Emergency Casualty Care que, al igual que estas Guías, son meras recomendaciones y no protocolos rígidos que deben adaptarse a la legislación vigente y, a las especificidades de cada Institución/Servicio/Organismo.
Con independencia de lo mencionado anteriormente, tienen como objetivo final estandarizar un lenguaje y unas actuaciones a nivel nacional dado que, están basadas en la evidencia científica “in vivo” y, en las lecciones aprendidas de muchos profesionales nacionales e internacionales. Estas recomendaciones/guías, no sustituirán el buen juicio clínico.
Por lo tanto, se espera que las recomendaciones que se presentan a continuación sirvan de ayuda para todo aquél personal policial que se pueda ver involucrado en un incidente con un nivel de amenaza elevado, a la hora de enfrentarse al manejo de las principales causas de muerte evitable que se producen en actuaciones con un alto nivel de amenaza.
MANUAL DE SOPORTE VITAL AVANZADO EN COMBATE Ministerio de Defensa España 2014 http://emssolutionsint.blogspot.com.es/2016/02/manual-de-soporte-vital-avanzado-en.html |
{kind=link}
{kind=link}
DOWNLOAD PDF FREE
{kind=link}
{kind=link}
ANTES
{kind=link}
DURANTE
{kind=link}
DESPUES
{kind=link}
¿Como actuar ante Incidente TERRORISTA? by SEMES
| TACTICAL MEDICINE TACMED “Medicina Bona Locis Malis” tm. Good Medicine In Bad Places España by EMS Solutions International Tactical Medicine TACMED España Marca Registrada Nº. 377.032 El curso Tactical Emergency Casualty Care (TECC) de NAEMT está basado en los principios del Tactical Combat Casualty Care (TCCC) y cumple con las guías establecidas por el Comité de Cuidado Táctico en Emergencias (C-TECC). Este curso enseña a los técnicos de emergencias médicas a cómo responder a un evento de tiroteo activo (“active shooter”) o de múltiples víctimas de trauma. El curso de TECC está diseñado para primeros respondedores a un incidente de múltiples víctimas. Medicina Bona Locis Malis = medicina buena en lugares peligrosos. Se describen las fases de manejo en situaciones tacticas por parte de los Rescue Task Force TFR. TACTICAL EMERGENCY CASUALTY CARE TECC Course # TE-18-04082-03 - Site ID# 5388 Santo Domingo, Distrito Nacional Republica Dominicana http:// emssolutionsint.blogspot.co m.es/2017/09/ curso-tecc-espana-28-septie Contactos: Dr. Ramon Reyes, MD eeiispain@gmail.com Alex Pacheco 809 849 9295 eeiird@gmail.com 19-20 de Mayo 2018 ****CUPOS LIMITADOS**** Nos reservamos el derecho de admision Inicio inscripcion: 01 Mayo 2018 Fin Inscripcion: 10 Mayo 2018 Cupos Limitados Precio US$190 (156 Euros) Equivalentes Pesos Dominicanos Deposito Cuenta Banco Popular Dominicano RD$ Nº 759765241 (Enviar Recibo para asegurar el cupo) Rescue Task Force RTF? / FUERZAS de TAREA de RESCATE Guatemala military/medic special ops team. Art byDansun Photos @DansunPhotos Todos Nuestros VIDEOS en YouTubehttps://www.youtube.com/c/ Grupo en TELEGRAM Sociedad Iberoamericana de Emergencias https://t.me/joinchat/ http:// emssolutionsint.blogspot.co m.es/2018/03/ tactical-medics-vs-rescue-t What is Tactical Emergency Casualty Care? by CTECC Tactical Emergency Casualty Care (TECC) is a set of evidenced-based and best practice trauma care guidelines for civilian high-threat pre-hospital environments. The TECC guidelines are built upon the critical medical lessons learned by US and allied military forces over the past 15 years of conflict and codified in the doctrine of Tactical Combat Casualty Care (TCCC). Using the military TCCC guidelines as a starting point, the Committee creates the civilian high threat medical guidelines through a process of literature research, evidence evaluation, expert discussion, and civilian best practices review. The TECC guidelines are built upon the foundations of TCCC but are different to meet the unique needs of the civilian medical and operational environments. The differences address civilian specific language, provider scope of practice, population, civilian liability, civilian mission and operational constraints, logistics, and resource acquisition. How are TECC and TCCC similar? Tactical Emergency Casualty Care is a set of civilian medical guidelines for high threat operations. Tactical Combat Casualty Care is a set of military medical guidelines for care of the wounded during military combat operations. The two sets of guidelines are naturally related, but each with a necessary difference in language, scope, applicability and flexibility. There are two key unifying principles of TCCC and TECC. First is the process of guideline development. Both Committees are comprised of medics, physicians, academics and operational leaders. Both Committees began with prior operational and medical lessons learned- for CoTCCC this was Vietnam and Somalia, for C-TECC this was TCCC and OIF/OEF- and rapidly evolved their recommendations based on immediate lessons learned. Second is an understanding that success requires developing and deploying a SYSTEM of care. In the military, TCCC’s success fundamentally lies in the fact that all personnel deploying to a combat theater were trained in the principles of TCCC. The operational and trauma care systems were built around this training. This second fact is also the main limiting factor for the deployment of TCCC in the civilian setting. As a system, TCCC cannot be deployed in the civilian setting because many recommendations run counter to civilian scope of practice and medical standards (e.g. use of hextend for resuscitation, pre-hospital antibiotics, needle decompression practiced by non medical personnel, etc.). How are TECC and TCCC different? Tactical Emergency Casualty Care is the civilian evolution and application of the military Tactical Combat Casualty Care guidelines. When discussing the differences between the two, it is important to emphasize that TECC and TCCC are not in competition with each other; although, as the pictures from the recent Boston Marathon bombing demonstrate, the bullets and explosives may be similar in civilian settings as in military combat, this does not make the military guidelines directly applicable for civilian applications. The two sets of guidelines are naturally related, but each with a necessary difference in language, scope, applicability and flexibility. There are three primary differences between TECC and TCCC: guideline terminology, trauma care recommendations and operational focus. Terminology/ Language: TCCC was written by the military special operations community to specifically address the specificities and conditions surrounding combat operations. These guidelines are researched, developed, and written with the assumption that the patient is an otherwise healthy 18-45yo soldier and that the provider is working under the military defined scope of practice. The TCCC guidelines assume a military medical support system, military rules of engagement, and military legal precedent. While individual recommendations such as tourniquet use are valid, TCCC as a system has limited application in the civilian setting. The TCCC courses currently being taught were not intended for civilian application. The Pre-Hospital Trauma Life Support TCCC course comes from the military PHTLS textbook, a version that was specifically written for the military medical community because the civilian PHTLS textbook had a different focus and application. All leaders with operational experience understand that the language changes in TECC are critical. As with the Incident Command System (ICS), common operating language is important for interagency response to complex threats. For example, “Care Under Fire”, has variable meanings across the Fire (e.g. actual fire), EMS (e.g. fire or gunshots- but a non operational zone) and Law Enforcement (e.g. active gunfire in the area) communities. Tactical Emergency Casualty Care was created to address these system limitations and specific scope of practice challenges related to TCCC. The C-TECC members, many of whom are active and past CoTCCC members, worked with civilian leaders to codify threat based guidelines (the core of TCCC) in a way that was easily applicable to civilian operations, legal and liability limitations and scope of practice, and in a way that is broadly applicable to the entirety of the civilian patient population. Trauma care guidelines: TECC and TCCC trauma recommendations are closely related. TECC places less emphasis on pre-hospital antibiotics, hextend as a resuscitation fluid, and specific product solutions. The TECC guidelines place more emphasis on interagency communication, integrated operations between EMS, Fire and Law Enforcement, casualty extraction and evacuation, and care of non-combatant civilians. Additionally, as the civilian high threat focus continues with the results of on-going study and medical data, the recommendations of TECC will necessarily diverge in small ways from TCCC. One recent example is the 2013 pediatric TECC guidelines. Children are not accounted for in the TCCC guidelines as they are not in the military deployable population. As such, the C-TECC specifically examined the research and data specific to the pediatric population and created a specific set of recommendations for children. Operational: The fundamental mission difference between the military and civilian high threat operations is important. In general, military operations focus on clearing, holding, and/or gaining territory with an emphasis on domination of enemy forces. By definition, civilian operations are rescue operations with the key missions of limiting civilian morbidity and mortality. Civilian first responders are sworn to “serve and protect”. Any guidelines must acknowledge this important difference and account for rescue operations, limitations in use of force, and other regional operational requirements. How can I get certified in TECC? The TECC guidelines are open source and non-proprietary with the exception of the TECC logo. There are currently no “official TECC courses” or a certified TECC provider/instructor. The C-TECC believes that, though there are universal “principles” of high threat response, the application must be tailored for individual agencies based upon local resources, political climate, budget and operational experience. “Cookie cutter” or standardized courses and applications for high threat operations fail to account for the differences among first responders that vary widely jurisdiction to jurisdiction, region to region, state to state, etc. As such, the concepts and skills in these classes have to be ‘un-learned’ or ‘ignored’ because they do not fit into the specific agency SOP or scope. TECC is not dogma, and the principles are meant to be applied uniquely by each agency that uses it, depending on that agency's provider levels, scope of practice, culture, patient population, risk assessment, etc. We consider the TECC guidelines to be a pile of bricks; take only the bricks that fit into your operational culture and build a response program that is unique to you. Just don’t change the individual bricks! Overall, the principles of TECC are not difficult to teach – the actual medical interventions such as pressure dressings and tourniquets are now commonplace for everyday trauma. What is unique about high threat medical principles is less about what is done medically and more about when it is done, what injuries on focused on, and what can be excluded. There are training entities that offer TECC courses. The Committee does not require any of these as your application of TECC is unique to your agency. If you cannot develop your own training, several of these companies offer a solid foundation of training. In the future, those companies and institutions that meet the principles of TECC guidelines instruction as set forth by the Committee may display a special C-TECC logo and be listed on the C-TECC.org website; until then, if you take a TECC class, make sure you check into the background and experience of the instructors first, and make sure that they are not teaching you TCCC and calling it TECC! How can I become a TECC instructor? There is currently no C-TECC sanctioned certification or classification as a ‘TECC instructor.” If you have the operational and educational experience to teach in your agency, if you have experience as an educator, or you are recognized by your agency as an instructor, you can take the open source TECC guidelines and create a course of instruction specific to your agency’s SOPs. I am a certified TCCC instructor. Can I teach TECC? Sure, although it is certainly not required. Knowledge of TCCC is helpful as TCCC is the starting point for TECC. You must understand however that the two are not the same, and must be clear on the differences between the two. Please also refer to the TECC skill set; at no point should skills outside of scope of practice be taught to students as a part of TECC. For example, although TECC includes needle decompression of a chest, this skill set should NOT be taught to providers if it is not specifically included in their scope of practice. Other than that, if you are familiar with instruction of the military combat medical guidelines, then your understanding of how to instruct the civilian high threat medical guidelines should be solid! How can my department or agency start a TECC program? Implementing the TECC guidelines into your agency’s standard operations for high threat response is not as ‘heavy a lift’ or difficult as one would think. If you have an operational plan for deployment of assets and operations during situations of high threat, the medical guidelines will fit in easily. The individual TECC guidelines, such as applying a tourniquet or using hemostatic gauze, are becoming common place in everyday pre-hospital management of trauma. Remember that TECC is less about what you do and more about when you do it. Teaching the TECC guidelines to your agency should be done in a way that is specific to your agency’s culture, scope, and approach to operational training. The Committee for Tactical Emergency Casualty Care is committed to assisting all response agencies and first responders who wish to utilize the guidelines. We have, and are working on, a variety of resources to assist you. Currently, we can provide a variety of educational articles and plenty of advice on how to get started. In the near future, we will be distributing a standard slide deck to get you started in teaching the guidelines. Feel free to contact the Committee with any questions or request for assistance. Is TECC only for law enforcement and SWAT operations? Absolutely not!!! Yes, it does have the word ‘tactical’ in its name but do not think that implies that the guidelines are for use only in law enforcement or tactical medical operations. Although the word ‘tactical’ in common use implies law enforcement associated operations, every first responder utilizes ‘tactics’ on every call every day. The Committee uses the word tactical to refer to the operational decisions that are made during response. Every one of these operational decisions has an effect on medical care and the competing priorities of operations and medical care need to be considered in real time. TECC allows you to do just this. TECC has applications for ALL high risk operations, where there is a real and on-going risk to both the patient and provider. Examples of high risk operations include, but are not limited to:
How can I become involved with the Committee? The development of the TECC guidelines was a grassroots effort by a group of operational medical personnel who identified the gap when applying military medical guidelines to a non-military population and operation. We remain a grassroots effort and thus all of our meetings are open to the public and everything we produce is available to all at no charge. Anyone can participate in the discussion regarding the TECC guidelines. We want your opinions and involvement as the guidelines are intended for all to use, not for just a few with special “certifications.’ We have two meetings a year: every December in conjunction with the Special Operations Medical Association conference in Tampa, FL, and a spring meeting at a different location every year. As a whole, about two months prior, we publish the information and logistics for our next meeting on the C-TECC website. As a 501c3, we have bylaws that outline the different committees, the number of members on each committee, the requirements for members and the process by which one becomes an official member. Part of that process is attending at least one meeting in person. If you are interested in becoming an official member, feel free to attend a meeting, and then contact us directly and submit a CV. In the meantime, be a part of the grassroots that is our foundation. Submit comments and questions on line – all will be heard and considered! Are the Committee’s meetings open to the public? As discussed in the question regarding how to become a member, all Committee meetings are open to the public. TECC is founded on a grassroots effort to address the operational gap that exists in high threat medical operations; as such, we want and encourage your opinions and involvement. We have two meetings a year: every December in conjunction with the Special Operations Medical Association conference in Tampa, FL, and a spring meeting at a different location every year. As a whole, about two months prior, we publish the information and logistics for our next meeting on the C-TECC website. How can I get more information on the Committee? Just ask! We will do all we can to answer your questions and support your operational use of the TECC guidelines. Currently on our website, under the resources tab, there are several articles on TECC and C-TECC that you can access. Are there approved TECC courses? Currently, there is no course approval or certification for TECC. As a whole, you do not need a course in TECC. We recommend that you use the in-house training staff and operational experts in your agency to create an operational paradigm and training program that is specific to your agency. That being said, there are many companies and training programs that state they teach TECC courses. Many of these are very good, but several teach military TCCC and just call it TECC. The two sets of guidelines are similar and related, but definitely different! So, if you cannot do it in-house for whatever reason and instead are seeking a TECC course, buyer beware! Do your due diligence to ensure that the content is consistent with TECC guidelines, that the instruction is matched to the students scope of practice, and that the instructional cadre has the expertise and TECC experience that they claim. In the near future, companies that agree to meet and adhere to the principles of TECC guidelines instruction being created by the Committee will be able to display a special C-TECC logo and be listed on our website to denote that the course of instruction is consistent with the TECC guidelines. How can I get my TECC course approved? Currently there is no ‘course approval’ process for TECC instruction. Feel free to create your TECC course utilizing the TECC guidelines as they are written. However, you must adhere to the principles of TECC – do not teach procedures outside of your student’s scope of practice, do not refer to equipment or supplies as ‘approved’ or ‘preferred’ or ‘recommended’, and do not change the language or intent of the guidelines. In the near future, the Committee will have a simple ‘principles of guidelines instruction’ that is an agreement between the Committee and the educational entity that will allow the course to display a special C-TECC logo to denote proper use and instruction of the guidelines. What equipment is TECC approved? None! The civilian patient population, the supply and equipment acquisition process, the budget and logistics of civilian response agencies and providers is completely different than the military. Just because a product is used or recommended by the military does NOT mean it is the best for civilian use. The military ‘recommended’ products are just that, recommended for the military population. These products do not take into account the aspects of civilian use including body and limb size, anticoagulation profiles, resources available, and the need for open bid acquisition. The Committee also will not endorse products as such endorsements may be misconstrued as unethical or done with impropriety. The C-TECC will discuss and offer existing evidence for products that have been tested and demonstrated effective, but does not specifically endorse any product. We recommend that every agency should explore the different product solutions available and make an agency specific decision based on available unbiased scientific data as well as agency and provider preference. Why are so many TCCC courses being taught to civilians? Tactical Combat Casualty Care is a great military medical innovation. These concepts have saved countless lives on the battlefield, and have provided a wealth of medical data for us to build upon. Until 2011, TCCC was the only existing set of high threat medical guidelines that existed. Multiple courses were developed to teach military personnel; these courses were made available to civilians as well. What is interesting, however, is that even prior to the development of TECC from the TCCC guidelines, civilian personnel who were trained in TCCC through these standard courses would bring the concepts back and have to alter or change what they were taught to fit the constraints of the civilian application. Essentially, what was being done was these civilian providers were taking TCCC and making into something appropriate for civilians. This is exactly how the efforts of the Committee for Tactical Emergency Casualty Care began, and is exactly what we have codified in the TECC guidelines. Courses in TCCC are still being offered and taught to civilians mainly because the infrastructure exists to do so; and these students are likely going back and changing what they learned to civilian appropriate for their agencies and application. As TECC continues to grow, the Committee will continue to distribute and emphasize the need for civilian specific and appropriate training through partnerships with federal agencies, civilian training entities such as PHTLS and ITLS, and future collaboration with professional pre-hospital, operational, and medical organizations. How are the guidelines updated? The Committee meets twice a year to discuss the guidelines and make changes based on current research and data. At these meetings, we review current research, data, and case reports that are relevant to the guidelines and raise questions as to where and what changes need to be made. As a whole, the December full committee meeting opens the discussion on any aspect of the guidelines and sets agenda for discussion and voting for the spring full committee meeting. If overwhelming data becomes available in-between meetings that show that the application of any individual guideline could cause harm, the Board of Directors will consider and make the necessary changes in real-time with the input of the Guidelines Committee and our Board of Advisor experts. An example of this process was the changes made to the TECC guidelines regarding limiting the use of Hextend after the FDA’s warning on Hextend use in critically injured patients. How can I submit a comment or an article for consideration? Please by all means submit the reference through the website! We rely on all of the first response community to assist us in identifying relevant data and research that may affect the Guidelines. How did TECC come to be included in the HSGP National Priorities, and how is it related to MCI preparedness? Recent events such as the mass shootings in Aurora (CO), Newtown (CT) and the bombing at the Boston Marathon have solidified the recognition that a national capability gap exists in terms of pre-hospital trauma care. The life safety of our citizens is recognized as government’s highest duty, and FEMA has named MCI preparedness as a national priority in order to address this gap. Improved out-of-hospital trauma care is integral to the successful management of mass casualty events. How did the TECC guidelines come about? The Committee for Tactical Emergency Casualty Care (C-TECC) was formed in 2010 to formally translate military trauma lessons learned into the civilian high-threat pre-hospital community. The C-TECC is modeled after the highly successful Committee on Tactical Combat Casualty Care (CoTCCC) – frequently credited as one of the major initiatives that has resulted in the lowest combat mortality rates in modern history. C-TECC brings together SME’s from EMS, fire, law enforcement and DHS/FEMA, as well as physicians from emergency departments, trauma centers and the military to develop evidence-based, best-practice principles of high-threat pre-hospital medicine. What does TECC address that other guidelines do not? The TECC guidelines take into account the requirements of a civilian population. This includes pediatric, geriatric, and special needs patients, as well as considerations for underlying medical conditions common in a civilian population, the characteristics and limitations of civilian EMS, and the varied types of threats that responders face. Military treatment guidelines were developed for a very specific purpose and population – fit and healthy 18-45 year olds in a combat environment. They have been extremely successful, but these guidelines cannot be directly carried over into the civilian population without taking these differences into account. Is this a training curriculum or an equipment product line that is being marketed? No – the TECC initiative was undertaken in order to advance the practice of trauma care in the pre-hospital civilian environment. To accomplish this, the guidelines are freely available to all. Training and equipment vendors are encouraged to incorporate the principles of TECC into their curricula and products. C-TECC is a not-for-profit (501c3) organization composed of subject matter experts who volunteer their time in order to benefit the public. C-TECC doesn’t offer training courses or product lines, nor does it endorse specific vendors or products. Does FEMA or any other federal agencies support or endorse TECC? Several federal agencies (including FEMA, DHS–Office of Health Affairs and multiple federal law enforcement agencies) have a role in the work of C-TECC, and representation on the Committee. TECC is prominently featured in the Joint Counter Terrorism Workshop Series (JCTAWS) initiative, which helps prepare urban areas for major mass casualty events. In order to support the efforts of implementing TECC into response paradigms, the FEMA Office of Counter Terrorism and Security Preparedness is sponsoring one-day seminars conducted by Technical Assistance teams composed of members from the C-TECC. The seminar is focused on providing an executive briefing on the development and uses of the guidelines, application design into existing and new response protocols, curriculum design and implementation strategies, and instructor train-the-trainer information. How can my jurisdiction or agency get more information or an orientation to the TECC initiative? The Committee is working on development of an orientation program that explains the foundations of the TECC principles, describes the medical evidence behind the guidelines and offers tips for implementation and training. http://www.c-tecc.org/about/faq The 2nd edition of NAEMT's Tactical Emergency Casualty Care (TECC) course teaches EMS practitioners and other prehospital providers how to respond to and care for patients in a civilian tactical environment. The course presents the three phases of tactical care and integrates parallel EMS nomenclature: Hot Zone/Direct Threat Care that is rendered while under attack or in adverse conditions. Warm Zone/Indirect Threat Care that is rendered while the threat has been suppressed but may resurface at any point. Cold Zone/Evacuation Care that is rendered while the casualty is being evacuated from the incident site. The 16-hour classroom course includes all new patient simulations and covers the following topics: Hemorrhage control including immediate action drills for tourniquet application throughout the course; Complete coverage of the MARCH assessment; Surgical airway control and needle decompression; Strategies for treating wounded responders in threatening environments; Caring for pediatric patients; Techniques for dragging and carrying victims to safety; and A final, mass-casualty/active shooter event simulation. NAEMT's TECC course is endorsed by the American College of Surgeons Committee on Trauma, is consistent with the current guidelines established by the Committee on TECC (Co-TECC), and meets all of the updated National Tactical Emergency Medical Support Competency Domains. This course is accredited by CAPCE for 16 hours of continuing education credit, and recognized by NREMT. NAEMT is a recognized education partner of the Co-TECC. The Co-TECC establishes guidelines for the provision of prehospital care to injured patients during a tactical incident. The Co-TECC neither creates curriculum for the prehospital provider, nor does it endorse the curriculum of other organizations. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
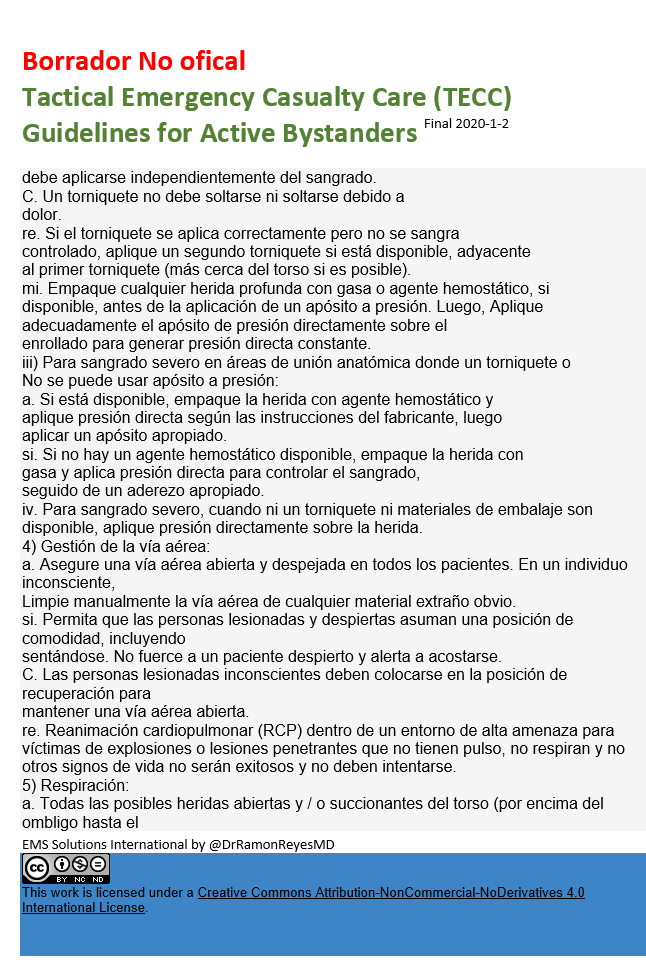{kind=link}
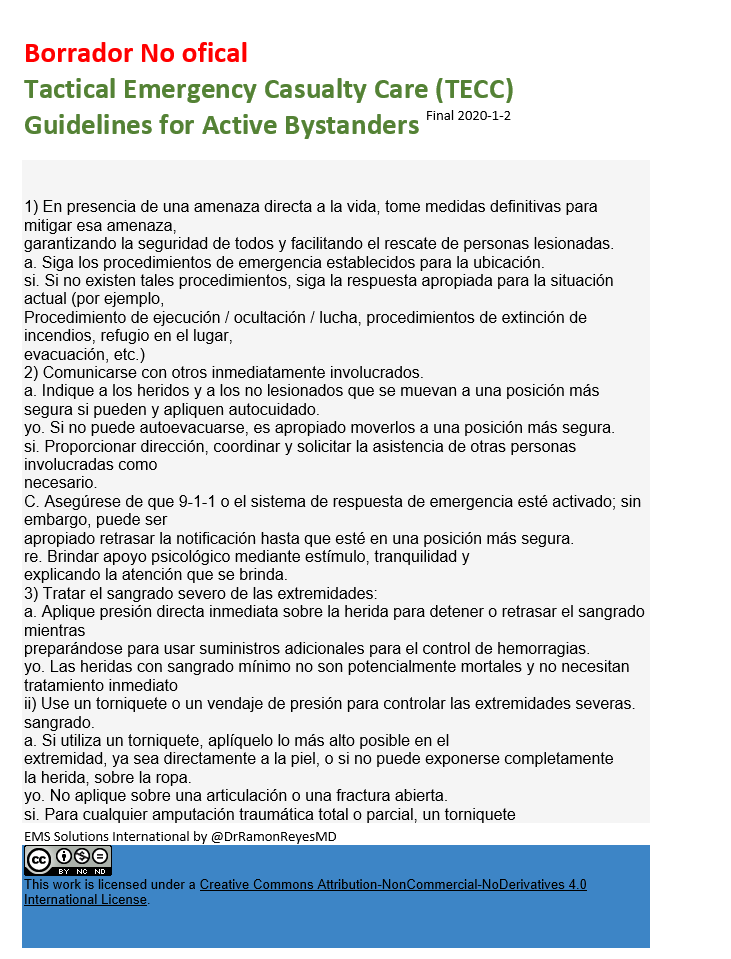{kind=link}
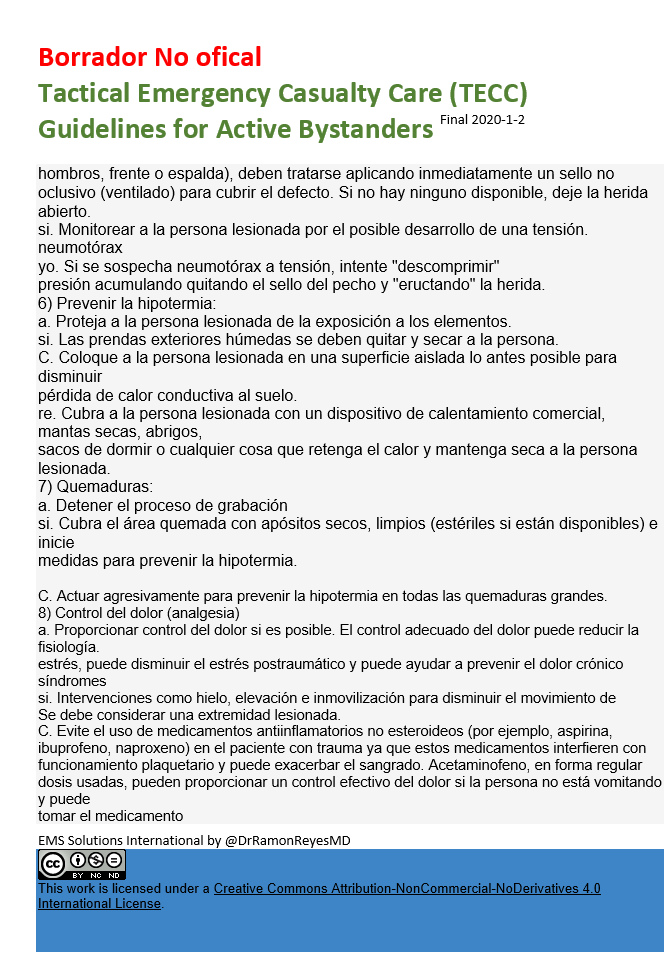{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ampliar informacion en el enlace
http://emssolutionsint.blogspot.com/2017/09/curso-tcc-lefr-tactical-casualty-care_4.html
http://emssolutionsint.blogspot.com/2017/09/curso-tcc-lefr-tactical-casualty-care_4.html
{kind=link}
{kind=link}
AED Automatic External Defibrillator . UN compacto, economico y seguro https://emssolutionsint.blogspot.com/2019/08/aed-automatic-external-defibrillator-un.html
DESCARGA MANUAL PDF en Español
{kind=link}
CORONAVIRUS covid-19
Dr Ramon REYES, MD,
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/groups/PDFgratisMedicina #DrRamonReyesMD
Facebook
https://www.facebook.com/DrRamonReyesMD
Instagram
https://www.instagram.com/drramonreyesmd/
Pinterest
https://www.pinterest.es/DrRamonReyesMD/
Twitter
https://twitter.com/eeiispain
Blog
http://emssolutionsint.blogspot.com/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html
TELEGRAM
Group https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/groups/PDFgratisMedicina #DrRamonReyesMD
https://www.facebook.com/DrRamonReyesMD
https://www.instagram.com/drramonreyesmd/
https://www.pinterest.es/DrRamonReyesMD/
https://twitter.com/eeiispain
Blog
http://emssolutionsint.blogspot.com/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html
TELEGRAM
Group https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q
AVISO IMPORTANTE A NUESTROS USUARIOS
Este Blog va dirigido a profesionales de la salud y publico en general EMS Solutions International garantiza, en la medida en que puede hacerlo, que los contenidos recomendados y comentados en el portal, lo son por profesionales de la salud. Del mismo modo, los comentarios y valoraciones que cada elemento de información recibe por el resto de usuarios registrados –profesionales y no profesionales-, garantiza la idoneidad y pertinencia de cada contenido.
Es pues, la propia comunidad de usuarios quien certifica la fiabilidad de cada uno de los elementos de información, a través de una tarea continua de refinamiento y valoración por parte de los usuarios.
Si usted encuentra información que considera erronea, le invitamos a hacer efectivo su registro para poder avisar al resto de usuarios y contribuir a la mejora de dicha información.
El objetivo del proyecto es proporcionar información sanitaria de calidad a los individuos, de forma que dicha educación repercuta positivamente en su estado de salud y el de su entorno. De ningún modo los contenidos recomendados en EMS Solutions International están destinados a reemplazar una consulta reglada con un profesional de la salud.