
A more careful and comparative reading with the previous edition will however allow some to note more profound modifications among others on the I-Gel.
To download the document in pdf:
#TCCC #CoTCCC #Medic #Tactical
{kind=link}
TCCC Guidelines 01 AUGUST 2018 Tactical Combat Casualty Care by JTS / CoTCCC. FREE pdf http://emssolutionsint.blogspot.com/2018/08/tccc-guidelines-01-august-2018-tactical.html
{kind=link}
Les Esperamos en nuestro Grupo en TELEGRAM Soc. IberoAmericana de Emergencias https://t.me/joinchat/FpTSAEHYjNLkNbq9204IzA
Todos Nuestros VIDEOS en YouTube
{kind=link}
{kind=link}
{kind=link}
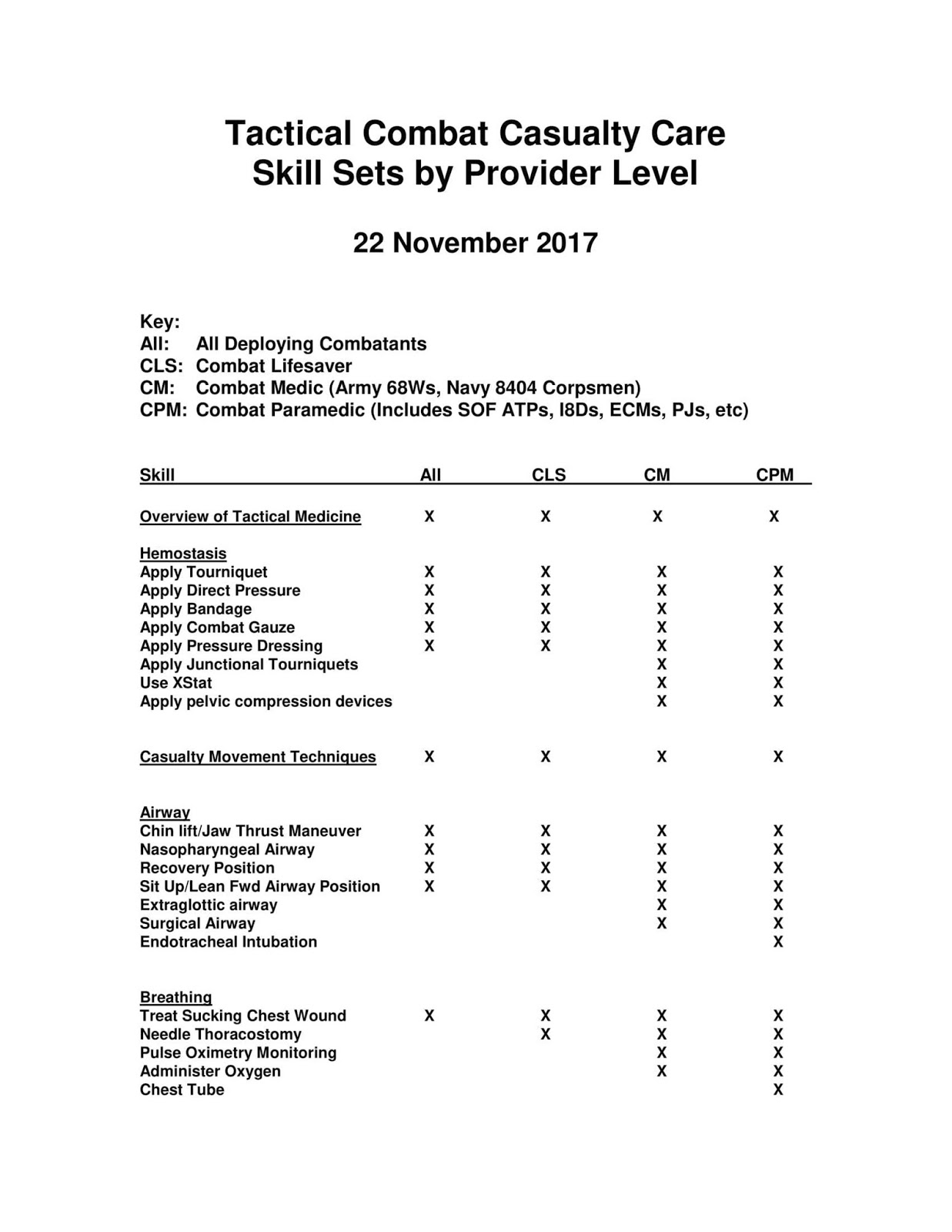
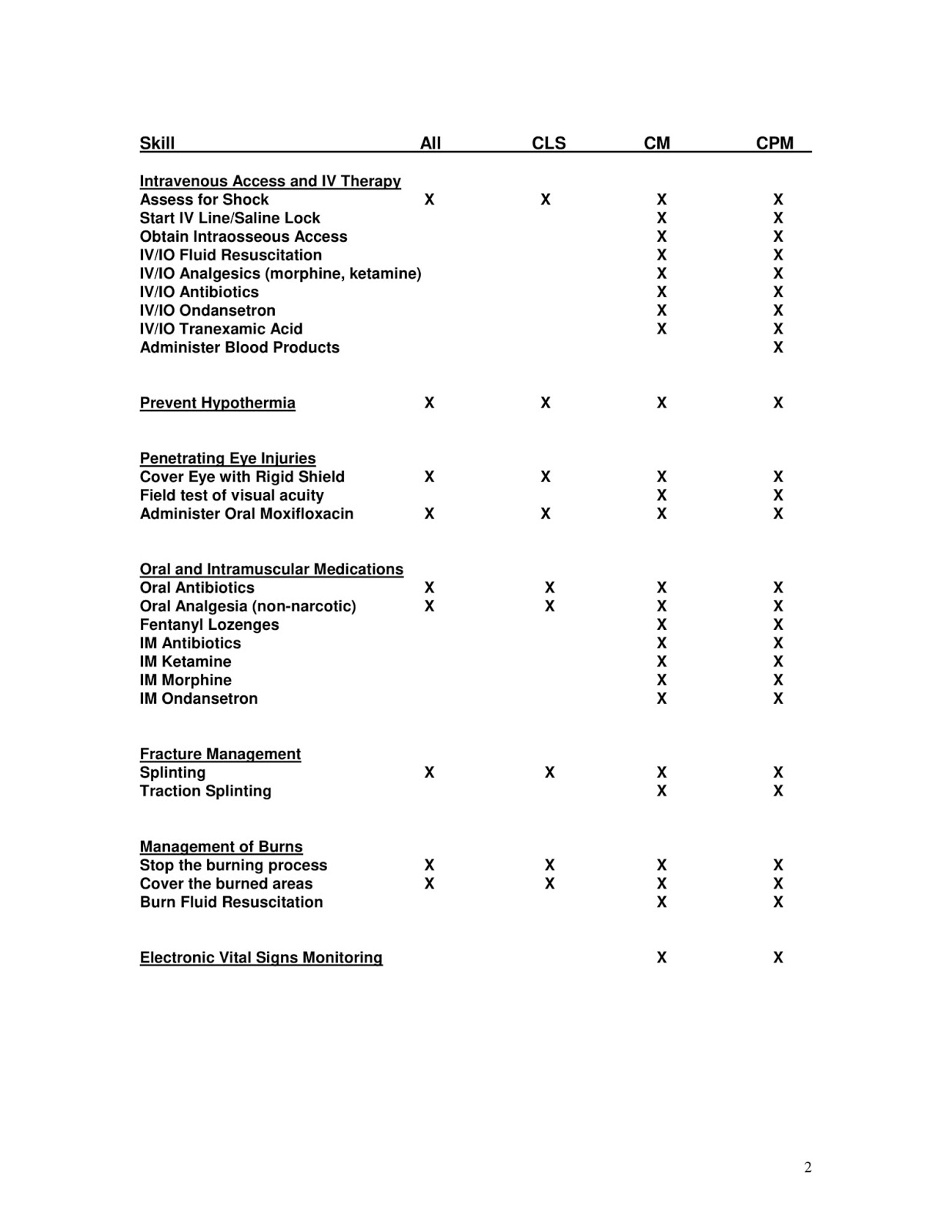
TCCC Tactical Combat Casualty Care Skills Sets by Provider Level
November 2017 by CoTCCC 2-2
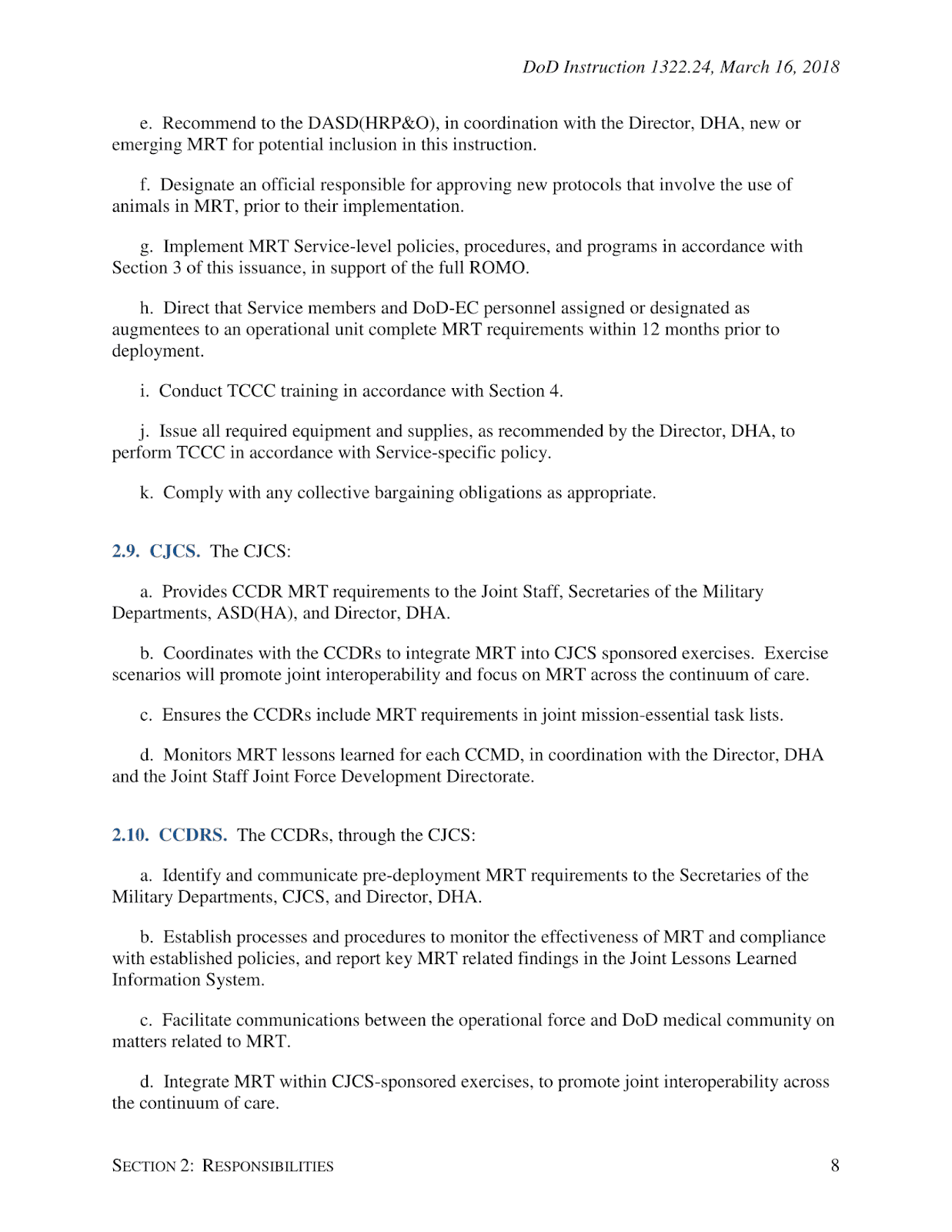
Effective 16 March 2018, Tactical Combat Casualty Care - TCCC - DoD Committee on TCCC is the DoD-wide standard for medical care.
Key Points:
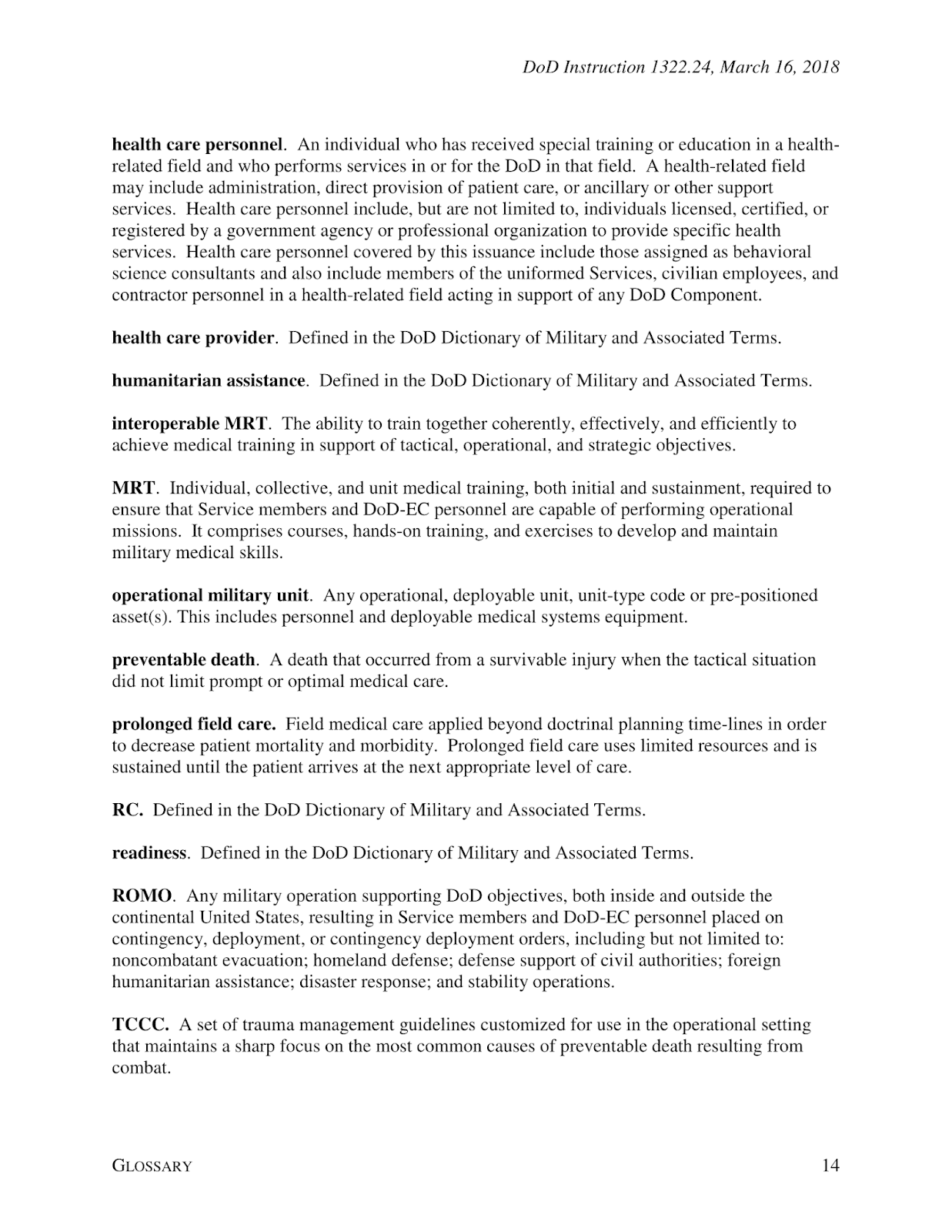
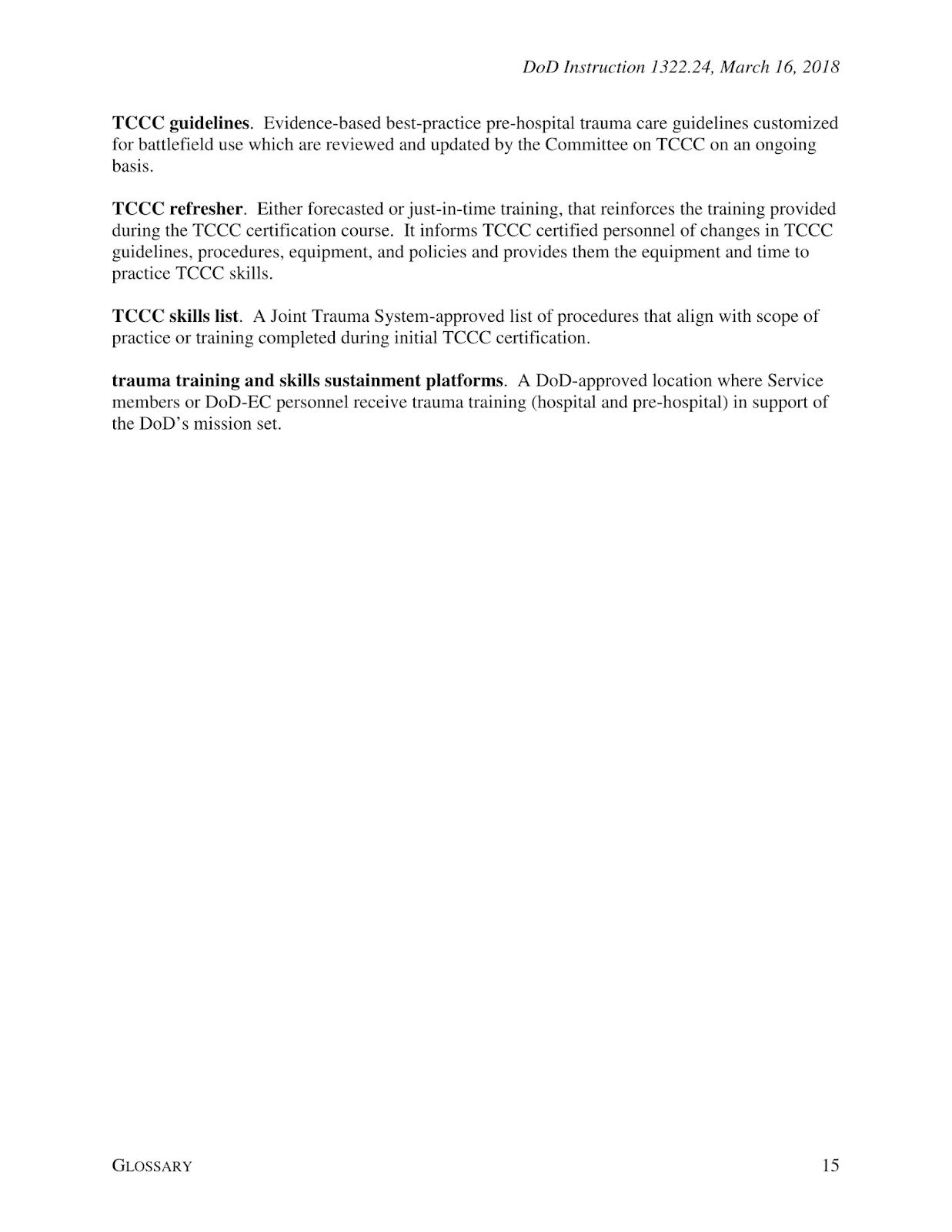
- TCCC is a set of evidence-based best-practice pre-hospital trauma care guidelines customized for battlefield use which are reviewed and updated by the Committee on TCCC on an ongoing basis.
- The "All Service Member" TCCC course replaces Service trauma skills currently taught in first aid and self-aid buddy care courses.
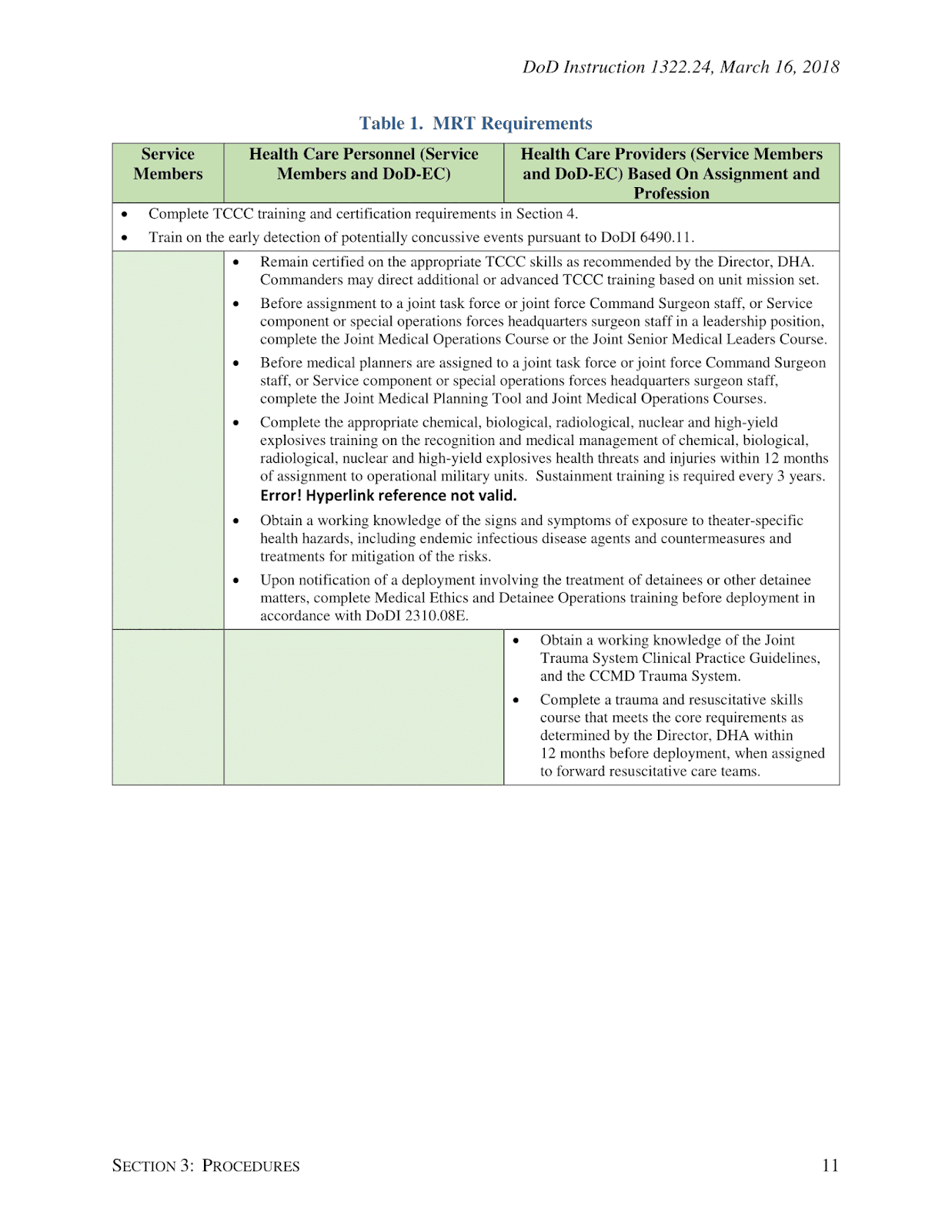
- Service members must complete MRT with their deploying unit within 12 months before departure.
- The Defense Health Agency is responsible for building, maintaining, and disseminating course materials. You can find the materials on DHA's Deployed Medicine website (deployedmedicine.com)
- The component services are responsible for ensuring their medical training programs are in keeping with the most current TCCC guidelines.
- All active duty Service members will complete TCCC recertification every 3 years. At a minimum, all reserve component Service members must complete TCCC certification, recertification, or refresher training within 12 months before deployment.
- TCCC is a set of evidence-based best-practice pre-hospital trauma care guidelines customized for battlefield use which are reviewed and updated by the Committee on TCCC on an ongoing basis.
- The "All Service Member" TCCC course replaces Service trauma skills currently taught in first aid and self-aid buddy care courses.
- Service members must complete MRT with their deploying unit within 12 months before departure.
- The Defense Health Agency is responsible for building, maintaining, and disseminating course materials. You can find the materials on DHA's Deployed Medicine website (deployedmedicine.com)
- The component services are responsible for ensuring their medical training programs are in keeping with the most current TCCC guidelines.
- All active duty Service members will complete TCCC recertification every 3 years. At a minimum, all reserve component Service members must complete TCCC certification, recertification, or refresher training within 12 months before deployment.
This is a huge leap forward in bringing the number of preventable battlefield deaths down to zero. Download a copy of the U.S. Department of Defense (DoD) Instruction below:
Download document in PDF Manual TCCC Español
TCCC vs CLS: which protocol is worth choosing in military training
Text: Hlib BITYUKOV
Photo: Matteї BATRUCH
Recently, there has been much debate over which system to use to train military to provide first aid. People more experienced in international standards choose systems used in NATO member states. Then the question arises which one is best for our military: ТССС or CLS.
The first acronym ТССС (Tactical Combat Causality Care) is a standardized, systematic approach aimed at treating potentially preventable causes of death on the battlefield. This is a guideline of actions arranged in the correct sequence.
Unlike civilian medicine it is not just a certain algorithm of actions, it also presupposes a tactical component. It provides a overall understanding of the battlefield and differentiation of different actions at various stages of a battle or its parts. ТССС protocol is available for public view onthe National Association of Emergency Medical Technicians in US (NAEMT) website.
The algorithm of actions for trauma care provided on the battlefield was adopted in the late 1990s in the USA. After the United States’ invasion of Afghanistan in 2001, there were many lifesaving advances in battlefield trauma care and this protocol was expanded and adopted as a basis for all medical personnel in US and later in NATO member states.
Now the ТССС protocol is reviewed annually and recommendations based on the most recent casualty information are issued in spring. You can see the latest changes and recommendations for battlefield trauma care on the NAEMT site.
All the internationally applicable guidelines and protocols of pre-hospital casualty care to some extent are based on a specific algorithm of actions, the emphasis of which is to support vital functions such as breathing and blood circulation. This is A-B-C protocol – Airways, Breathing, Circulation.The battlefield introduces certain changes to this protocol. Primarily, it presupposes critical bleeding control, which is a major cause of premature death and disability on the battlefield, considering the fact that the casualty and everybody else are at risk of getting injured.
Tactical medicine differs from civilian medicine in terms of trauma types or wound types, surroundings, the ability to provide casualty care and the time necessary for casualty evacuation (sometimes it is much longer under combat conditions).
Tactical medicine is built around three definitive phases of casualty care which are fully compliant with ТССС protocols.
- Care under fire. It is a situation where both the casualty and the care provider are in danger from enemy fire and aims at minimizing the number of casualties. Care in this phase depends on the scarce equipment carried by each military.
- Tactical field care. Tactical field care is rendered once the casualty and the care provider are no longer under hostile fire. Medical equipment is still limited to that carried into the field by the care provider or other mission personnel. Care in this phase depends on time prior to evacuation, which may range from a few minutes to many hours.
- Tactical evacuation care. Tactical evacuation care is rendered during evacuation. Often but not always this may include qualified professionals and minimum amount of necessary equipment.
These standards are used not only for training military units. They are also mandatory for police and emergency medical technicians.
ТССС protocols unlike civilian medicine use MARCH algorithm (Massive Hemorrhage-Airways-Respiration-Circulation-Hypothermia), however the essence of this approach is pretty much the same as in С-А-В-С algorithm.
This protocol is a guideline for medical personnel and military who have passed the necessary medical training. It includes intravenous or intraosseous fluid resuscitation, use of anti-hemorrhagic or hemostatic agents such as tranexamic acid, colloidal solutions, analgesia such as ketamine or morphine, antibiotics and medical equipment, which is not available for soldiers.
It is important to realize that a combat lifesaver is not a professional medic and his first priority is to fight. First of all, he is a soldier. Primarily, the military should be trained to return fire and save lives depending on the combat conditions.
Therefore, “Combat Lifesaver course” (CLS) was developed to train people how to provide first aid. This course was adapted for all military branches and is compliant with ТССС protocols and recommendations.
First, the course implies that a combat lifesaver has no medical knowledge or skills sufficient for complex medical procedures, he is limited in the number of medical equipment available on the battlefield, and time following traumatic injury being sustained by a casualty up to their transfer to professional medical personnel may range from a few minutes to many hours.
This course is internationally recognized and was first introduced by the US Army for those who need medical care under effective enemy fire.
The course is also divided into three definite phases of providing casualty care:
- Care under fire. The course takes into account that the first priority of a soldier while under fire is to continue firing at the enemy and try to prevent further casualties, to return fire and kill the enemy, to move to a safe location from enemy fire and stop life threatening bleeding.
- Tactical field care.The course is based on simple actions to ensure vital functions: critical bleeding control, rapid airway management, breathing and chest examination, stabilizing blood flow; and does not include medical actions that require special skills and knowledge. It includes tactical elements as well as proving first aid. However, this care is based on the available medical equipment carried into the field by individual soldiers in his or her individual first aid kits (IFAKs).
- Tactical evacuation care. This phase includes preventing hypothermia, continuous casualty monitoring, documenting the care and requesting further medical assistance.
Apart from medical skills, the course involves tactical component practice with the emphasis on military unit specifics, and focuses more on casualty care under fire.
Adapted “Combat Lifesaver course” (CLC), conducted by “Patriot Defence”, lasts for 16 hours, 2.5 of which are dedicated to care under fire.
In addition, the course was developed with the idea that each combat lifesaver could and should be able to provide first aid and be a link between the casualty and medical personnel, including military doctor assistance if a combat lifesaver has no priority military tasks.
Combat Lifesaver coursegives a possibility to save lives of casualties on prehospital stage. This course must become mandatory for all law enforcement agencies, such as the Security Service, the Armed Forces, the National Guard, the State Border Guard Service, Police Service, the Administration of State Guard of Ukraine, etc.
Comparing core skills requirements according to CLS and TCCC training course
CLS | TCCC | |
Casualty care on the battlefield is divided into definitive phases | V | V |
Algorithm С-А-В-С (MARCH) | V | V |
Combat Application Tourniquet | V | V |
Nasopharyngeal airway | V | V |
Occlusive dressings | V | V |
Needle decompression | V | V |
Hemostatic dressings | V | V |
Bandaging | V | V |
Check for additional wounds | V | V |
Prevention of hypothermia | V | V |
Documentation of care | V | V |
Monitoring the casualty | V | V |
Requesting further medical assistance. | V | V |
Intravenous/intraosseous fluid resuscitation | V | |
The use of drugs such as tranexamic acid, ketamine, morphine | V | |
Colloidal solutions | V | |
Burns or fractures care | V |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
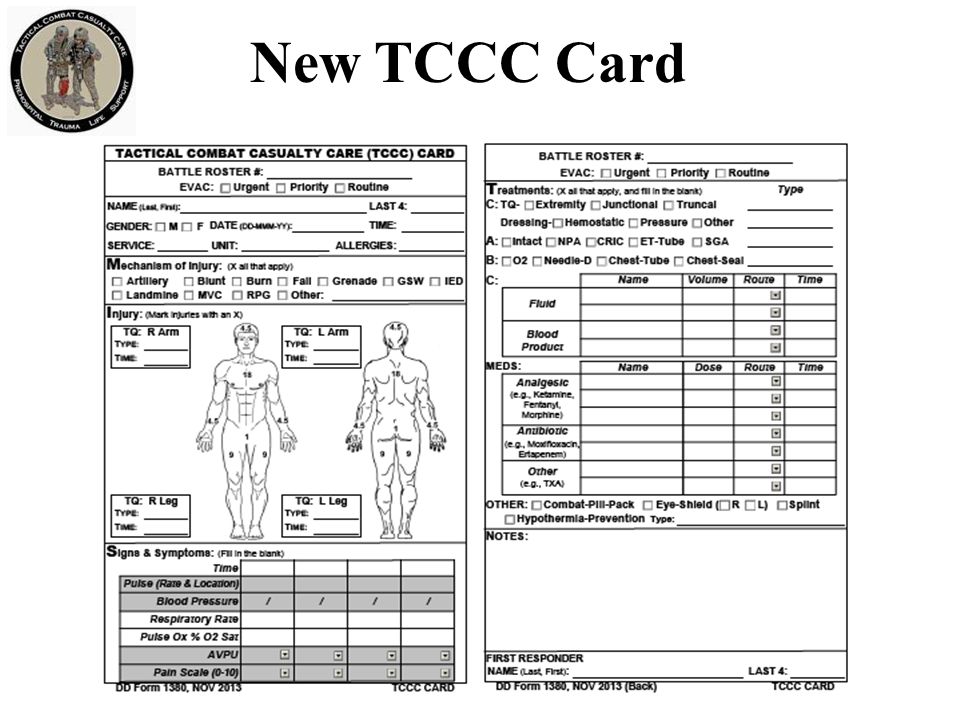
TCCC Card
Tactical Combat Casualty Care TCCC