
| Inflight medical emergency Compilation made by Dr. Ramon Reyes, MD |
{kind=link}
Grupo en TELEGRAM Sociedad Iberoamericana de Emergencias https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q
Emergencias médicas durante un vuelo comercial
{kind=link}
It might seem like an odd thing to pack in a travel bag, but Rachel Zang, MD, never boards a flight without a supply of ondansetron. On a flight from the United Kingdom back to the United States, Zang stepped up to help a 2-year-old who was vomiting. To her surprise, the medical kit on board had no antiemetics.
“The standard [kits] do not require them,” says Zang, a fourth-year emergency medicine resident at the Hospital of the University of Pennsylvania in Philadelphia. “You have no ability to give a medication to stop vomiting.”
As a frequent traveler—she has been to 30 countries, including medical missions to Tanzania and Rwanda—Zang wanted to be better prepared when the next in-flight medical emergency crops up. She researched domestic and international laws and learned what those airline medical kits are supposed to contain and what they lack.
In fact, Zang amassed so much material that she shared it with her colleagues during a grand rounds on in-flight medicine. “Lots of people were interested,” she says. “[I]t’s something everyone’s a little uncomfortable with … so they want to know as much information as they can about it.”
With summer travel in full swing, Zang spent some on-the-ground time talking with JAMA about the ins and outs of responding to in-flight medical emergencies. The following is an edited version of that conversation.
JAMA:How often have you encountered medical emergencies on flights?
Dr Zang:In the last 4 years, I've had 2 medical emergencies that I responded to, and then my husband has had 2 as well. He’s also a physician.
JAMA:The common conditions that usually occur in flight are lightheadedness, loss of consciousness, nausea, vomiting, and cardiac or respiratory symptoms. Have these been the conditions that you, your husband, or other physicians you know have encountered during flights?
Dr Zang:Yes, definitely. My husband has responded to 2 syncopal episodes and many of my colleagues have responded to lightheadedness or vomiting. In the literature, the most common condition is syncope or near syncope. That accounts for about 37% of in-flight medical emergencies. The next most common is respiratory distress. That's about 12%, followed by vomiting and then chest pain.
JAMA:Are those conditions related to circumstances inside the plane, either cabin pressure or other factors?
Dr Zang:The airplane causes a lot of unique changes in the body that we're not really aware of. Being on a flight is the equivalent to being at 6000 to 8000 feet of altitude. At sea level, oxygen saturation in all of us healthy people is 99% to 100%, but when we go up into the air, most of us would be about 92% to 95%. So you can see how anyone who had underlying respiratory or cardiac issues, if their oxygen saturation drops lower, it's going to exacerbate angina or make their COPD [chronic obstructive pulmonary disease] or asthma worse. In turn, the very low humidity in the airplane has been shown to exacerbate asthma and COPD because of the increased dehydration and the increased mucosal dryness.
JAMA:Were the medical supplies on the plane adequate for the emergencies you dealt with?
Dr Zang:The emergencies that I handled were minor. One person had a headache and wanted Tylenol, which is in the medical kit. For the young child who was vomiting and very dehydrated, I had to mix my own oral rehydration solution, which is very easy. It's 6 teaspoons of sugar and half a teaspoon of salt in a liter of water. And you have syringes. So for very little kids, you can mix that up, and mom can give it to the child. Or you could use an IV [intravenous route] in a dehydrated child, which I think would be very challenging in the air.
JAMA:Are there standard supplies that airlines are required to keep on board, either by federal law or their company policies?
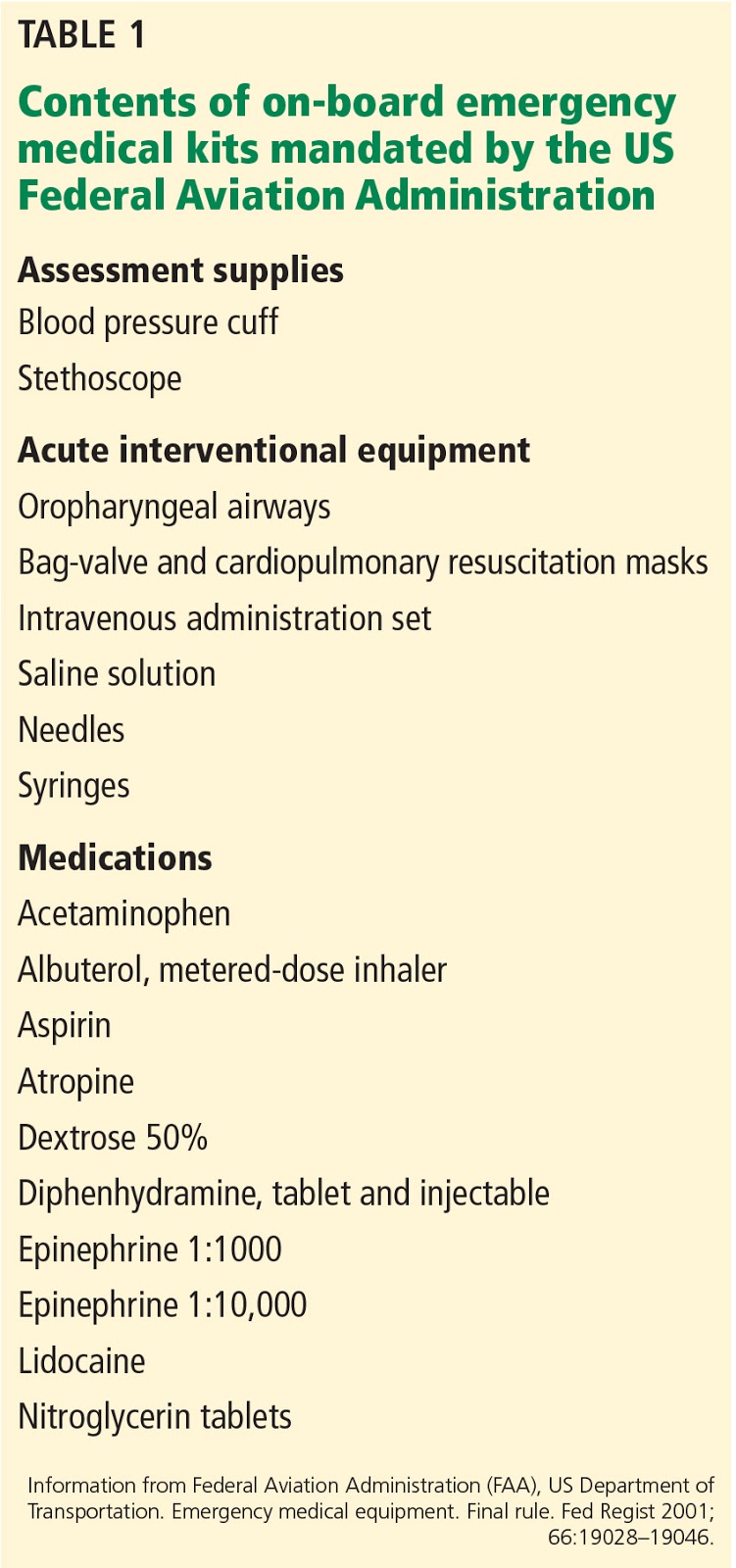
Dr Zang:In the United States, federal law mandates that all airlines have a first aid kit, an oxygen tank with enough oxygen for 2% of the passengers for the duration of the flight, and an AED [automated external defibrillator]. In the standard medical kit you get a stethoscope, blood pressure cuff, and gloves. You get an array of oral airways and bag valve masks and CPR [cardiopulmonary resuscitation] masks. You get a few needles, a few syringes, and a 500-cc bag of saline solution, and then you get a short list of medications: Tylenol and Benadryl in oral and IV form, aspirin, atropine, albuterol, and 1 A of D50 [50% dextrose]. You also have epinephrine in both IO [intraosseus] dose and anaphylactic dose, lidocaine, and nitroglycerin tablets.
JAMA:Despite the US minimum requirements, do any airlines go beyond the minimum?
Dr Zang:The only airlines I found that went beyond the minimum were international airlines. That's not to say US airlines don't; I just couldn't find any documentation. Some that go above and beyond are ANA [All Nippon Airways], a Japanese airline, and Lufthansa. Both of them have very extensive medical kits, and they have a program called Doctor on Board that allows you to designate yourself as a physician when you book your ticket so they don't have to page overhead. They provide some access to their medical supply kits and information when you sign up so you know what's on their plane. Turkish Airlines has a similar program.
JAMA:Would it be helpful to have a universal program like that for all airlines worldwide?
Dr Zang:Yes. We don't even have a national reporting database to figure out how often these in-flight medical emergencies happen. We think the numbers we have are grossly underestimated and it is well known in the airline industry that in-flight medical emergencies are expected to increase. People are flying more often and more elderly and people with preexisting medical conditions are flying. It's expected that by 2023, half of airline passengers will be over the age of 50. Doctors could be better equipped if there was a standard medical kit on every flight so you knew the medication and equipment you had access to.
JAMA:If you had a wish list of onboard improvements, what would they be?
Dr Zang:I would start small. Since 2001, when regulations for the emergency medical kit and the AED onboard went into effect, the FAA [Federal Aviation Administration] has not reexamined the medications in the kit. For example, lidocaine is still in the kit because it used to be recommended for cardiac arrest. It no longer is, but it's still in the kit, as opposed other medications. At the very least, it would be nice if the FAA would reevaluate what's in the mandated medical kit and add some basic things like Zofran for an antiemetic. On a broader scale, airlines are governed by so many different bodies, not just in the United States, but internationally.
So my wish would be that one person could create an international governing body of airlines and have it mandate medical equipment. The AED is necessary; a few more in the kit would be helpful. Now, if you want to put in an IV, you have 2 tries, and that's it. If you miss, you're done. Some more fluid in the kit would be helpful; 500 cc is not very much if you're dealing with a significantly dehydrated person on a long flight. Definitely, the medications need to be updated. If I had all of my dreams, pediatric and obstetric equipment would be included. There is no obstetric medication in any of the kits and there is no pediatric dosing or, aside from a CPR mask, anything pediatric related. There's not even a glucometer.
So my wish would be that one person could create an international governing body of airlines and have it mandate medical equipment. The AED is necessary; a few more in the kit would be helpful. Now, if you want to put in an IV, you have 2 tries, and that's it. If you miss, you're done. Some more fluid in the kit would be helpful; 500 cc is not very much if you're dealing with a significantly dehydrated person on a long flight. Definitely, the medications need to be updated. If I had all of my dreams, pediatric and obstetric equipment would be included. There is no obstetric medication in any of the kits and there is no pediatric dosing or, aside from a CPR mask, anything pediatric related. There's not even a glucometer.
JAMA:Do you think physicians sometimes are hesitant to come forward when there's a medical emergency on their flight?
Dr Zang:Yes, for a variety of reasons. You don't know why they're asking for a physician or if you're equipped to handle what they're asking for. Maybe you're really exhausted from a long trip. Maybe you had a beer with your dinner and you're not sure if you should step in. I think a lot of physicians aren't sure what their liability is if something goes wrong. So there's a whole host of reasons why physicians would feel uncomfortable.
JAMA:What are the potential legal liabilities?
Dr Zang:It depends on where you are. The US has the Aviation Medical Assistance Act of 1998 that says individuals shall not be liable for damages in federal or state court for any reason when they provide in-flight medical care unless they were grossly negligent or had willful misconduct. This covers physicians, nurses, nursing assistants, paramedics, and EMTs (emergency medical technicians). What that says is you will not be penalized if you attempt to help in good faith. The only reason that you could be liable is if you were grossly negligent because you were so fatigued you couldn't think straight, or you had taken medication because you were planning to sleep, or you were intoxicated because you drank a lot on the plane. The Act goes even further and says you can't be held liable if your recommendation is to divert the plane and they don't and something goes wrong. You can't be held liable if the equipment fails or if the patient collapses in front of you and you jump in to help even though nobody asked.
What’s less clear is when you're on international flights. For example, the United Kingdom does not have national law on this, and their airlines decide individually how they will cover physicians’ legal protections. British Airways, Virgin Atlantic, and other carriers provide indemnity for medical professionals, but unless you're looking up every flight, you might not know how you're covered. Then it becomes unclear what airspace you're in. If you’re on a French flight to the US in US airspace, are you covered under US law or French law? It can get complicated.
What’s less clear is when you're on international flights. For example, the United Kingdom does not have national law on this, and their airlines decide individually how they will cover physicians’ legal protections. British Airways, Virgin Atlantic, and other carriers provide indemnity for medical professionals, but unless you're looking up every flight, you might not know how you're covered. Then it becomes unclear what airspace you're in. If you’re on a French flight to the US in US airspace, are you covered under US law or French law? It can get complicated.
JAMA:Have you ever had to ask the pilot to divert the flight?
Dr Zang:I have never been in that situation. But diverting a flight is not as simple as it may seem because it involves a lot of other things besides the issue of that 1 patient. How far are you from the next possible airport and what is the emergency they're having? If somebody's going into labor, the next closest airport might not have medical capabilities to deal with obstetric issues. Ultimately, it's the pilot's decision.
JAMA:This issue was in the news recently after a lawsuit was filed in a case from 2016. A young woman died after a physician on the plane said she needed immediate care on the ground. An airline physician on the ground advised to continue on for 90 minutes and the pilot didn’t divert the flight. The woman died 3 days later; the cause reportedly was a pulmonary embolism. Is there anything else a physician could do in a circumstance like that?
Dr Zang:No. All you can do is speak with the ground doctor and the pilot and offer your recommendations. If the patient worsens or something changes, it's important to relay that to the ground doctor because it might change his or her decision. Statistically, the pilot will side with the doctor on the ground simply because they tend to have more experience in in-flight medical emergencies.
JAMA:During your grand grounds on in-flight medical emergencies, what were the most important things you felt your colleagues should know, especially those who had never encountered an in-flight emergency?
Dr Zang:The most important things for them to know were what equipment they can expect to have on board, the most common chief complaints, and what other resources they have. Flight attendants are all certified in CPR and AED use. Having access to a medical command doctor who deals with in-flight medical emergencies every day was something I didn’t know, and I think it's helpful to realize that you're not entirely alone up in the air.
I've received a lot of questions about credentials. The Aviation Medical Assistance Act of 1998 says that in good faith, the flight attendants believe the passenger offering assistance is a medical-qualified individual. So technically, you do not have to show credentials. But the FAA has come out with other regulatory letters, most recently in 2006, that said it’s preferable for flight attendants to check credentials of people holding themselves out as medical specialists. So I wouldn't be surprised or offended if somebody asks for credentials. I always fly with my medical credentials now.
I've received a lot of questions about credentials. The Aviation Medical Assistance Act of 1998 says that in good faith, the flight attendants believe the passenger offering assistance is a medical-qualified individual. So technically, you do not have to show credentials. But the FAA has come out with other regulatory letters, most recently in 2006, that said it’s preferable for flight attendants to check credentials of people holding themselves out as medical specialists. So I wouldn't be surprised or offended if somebody asks for credentials. I always fly with my medical credentials now.
| HOW LUFTHANSA CARES FOR PASSENGERS’ MEDICAL NEEDS BY BEN GRANUCCI Lets face it, nobody wants to need medical care while on board a plane. And yet, with a huge number of people traveling by air everyday, it’s inevitable that it will happen with some regularity. In fact if you travel by air regularly, you have probably heard the flight attendants ask over the PA if there is a “medical professional onboard.” Any malady that can occur on the ground can happen in the air, and the altitude while on a commercial aircraft can even exacerbate certain medical conditions. That means that some people may be more likely to need medical assistance in the air than they do on the ground. For German airline Lufthansa, there are about 3,000 passenger medical emergencies that occur on board each year. Of those, an average of 54 emergencies are serious enough that they require the flight to be diverted so that a patient can obtain urgent medical care. I recently had a chance to sit down with the airline and learn how they cope with these situations. Not only is the airline well prepared for any emergency that may arise in flight, they are also ready to treat those who need care before they board the aircraft. Emergencies On Board A rendering of the inside of Lufthansa’s Patient Transport Compartment, the “flying ICU” – Image: Lufthansa As mentioned above, Lufthansa averages 3,000 on-board medical emergencies of varying levels of severity each year. Just like any other airline, their flight attendants receive regular training on inflight first aid and emergency procedures. Crews are also trained to assist medical professionals when that need arises. However, this is where the similarities between Lufthansa and most other airlines ends. |
{kind=link}
In-Flight Medical Emergency Support.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1 in every 604 flights involves medical situation, study says
You may have heard this announcement before: "Ladies and gentlemen, a passenger requires medical attention. If there is a physician or medical personnel on board, please identify yourself to a flight attendant." One in every 604 flights involves a reported medical emergency, according to a 2013 study published in the New England Journal of Medicine. Researchers at the University of Pittsburgh Medical Center calculated that translates into 44,000 in-flight medical emergencies worldwide every year. The actual number may be much higher, because no mandatory reporting system exists and minor issues are very likely underreported. The most common problems, according to the data collected, were fainting or feeling dizzy and lightheaded (37%), respiratory symptoms (12%) and nausea or vomiting (10%). But how are these emergencies handled, especially when they're more complicated or life-threatening Ground support In-flight medical emergencies unfold in the skies above us every day, so many large airline companies spend a lot of time and money training their flight crews on what to do when presented with these types of extraordinary situations. "The flight attendants are trained as new hires very extensively, and then every year they have recurrent training that includes emergency response," said Barbara Martin, general manager for Air, Crew and Passenger Health Services at Delta Air Lines. "They are using a medical assistance form to get the key, most important data on signs, symptoms and vital signs," said Martin, who is an occupational nurse by training. "The pilots and dispatchers on the ground ... are also trained in what the key elements of information are that need to be transmitted to STAT-MD if there's a consult," Martin said. "It's really a team effort." You've probably never heard of STAT-MD, but the medical professionals at this low-profile University of Pittsburgh Medical Center medical communications center provide ground-based support services for a number of large commercial airlines based in North America. "We basically provide in-flight consultations for in-flight emergencies, and we also provide fitness-to-fly screening for the airlines for (passengers) on the ground in case there's a question on their ability to go up into the air," said Dr. TJ Doyle, STAT-MD's medical director. Doyle said they did about 10,000 consults last year, so they're fielding about one or two calls an hour. "The captain is always in charge," said Doyle. "We make a recommendation based on our expertise, and our experience. We've been doing this for a while and we do it quite often. So we'll make a recommendation to the captain on what we think can occur." In the most extreme cases, that might mean recommending diverting the flight. This occurred in 7.3% of the cases reported in the 2013 study. Far more often, the issue is something much simpler: a diabetic whose sugar has plummeted, so he or she needs a sip of orange juice. Or perhaps someone is feeling lightheaded and may just need to be administered oxygen.
You may have heard this announcement before:
"Ladies and gentlemen, a passenger requires medical attention. If there is a physician or medical personnel on board, please identify yourself to a flight attendant."
One in every 604 flights involves a reported medical emergency, according to a 2013 study published in the New England Journal of Medicine. Researchers at the University of Pittsburgh Medical Center calculated that translates into 44,000 in-flight medical emergencies worldwide every year.
The actual number may be much higher, because no mandatory reporting system exists and minor issues are very likely underreported.
The most common problems, according to the data collected, were fainting or feeling dizzy and lightheaded (37%), respiratory symptoms (12%) and nausea or vomiting (10%).
But how are these emergencies handled, especially when they're more complicated or life-threatening
Ground support
In-flight medical emergencies unfold in the skies above us every day, so many large airline companies spend a lot of time and money training their flight crews on what to do when presented with these types of extraordinary situations.
"The flight attendants are trained as new hires very extensively, and then every year they have recurrent training that includes emergency response," said Barbara Martin, general manager for Air, Crew and Passenger Health Services at Delta Air Lines.
"They are using a medical assistance form to get the key, most important data on signs, symptoms and vital signs," said Martin, who is an occupational nurse by training.
"The pilots and dispatchers on the ground ... are also trained in what the key elements of information are that need to be transmitted to STAT-MD if there's a consult," Martin said. "It's really a team effort."
You've probably never heard of STAT-MD, but the medical professionals at this low-profile University of Pittsburgh Medical Center medical communications center provide ground-based support services for a number of large commercial airlines based in North America.
"We basically provide in-flight consultations for in-flight emergencies, and we also provide fitness-to-fly screening for the airlines for (passengers) on the ground in case there's a question on their ability to go up into the air," said Dr. TJ Doyle, STAT-MD's medical director.
Doyle said they did about 10,000 consults last year, so they're fielding about one or two calls an hour.
"The captain is always in charge," said Doyle. "We make a recommendation based on our expertise, and our experience. We've been doing this for a while and we do it quite often. So we'll make a recommendation to the captain on what we think can occur."
In the most extreme cases, that might mean recommending diverting the flight. This occurred in 7.3% of the cases reported in the 2013 study.
Far more often, the issue is something much simpler: a diabetic whose sugar has plummeted, so he or she needs a sip of orange juice. Or perhaps someone is feeling lightheaded and may just need to be administered oxygen.
Managing medical emergencies at 30,000 feet
When the problem is more serious "If it can happen on the ground, it's going to happen in the air, as well, so we need to be able to respond to that appropriately," said Delta flight attendant trainer Justin Eberle. "Passenger safety is always our number one priority." All flight attendants working routes in the United States must be trained in CPR and how to use a defibrillator. "The flight attendants have access to what we call a medical accessory kit," said Martin. "That's got basic equipment in it for taking blood pressure, thermometers, personal protective equipment. If there's a medical volunteer on board, then they're given access to our emergency medical kit, and that kit has resuscitation equipment, IV equipment, medications." Many airlines require consultation with a ground-based physician, such as STAT-MD, before the emergency medical kit is used. There is one other prominent medical communications center in the United States called MedAire, based in Phoenix, Arizona, but those calls may not always be answered by a medical doctor. Kits vary widely in quality. The FAA requires contents such as saline solution, aspirin, antihistamines, epinephrine and nitroglycerine tablets. Some airlines choose to supplement the basic provisions, but supplies and medications are expensive, they take up weight and they have to be replaced when they expire. It goes without saying, too, that some protocols and procedures are more challenging in the air. A simple stethoscope, for example, is rendered relatively useless in flight because of all the ambient noise. 'Is there a doctor on the plane?' More useful, often, than the equipment is the expertise of a fellow passenger. Physician passengers provided medical assistance in 48.1% of reported in-flight medical emergencies, according to the 2013 study. Nurses assisted in 20.1% of the cases. Martin says the number is even higher. "Over the years, we've seen at least an 80% presence of a physician or RN volunteer," said Martin. "In fact, the most recent year we compiled data on, 2014, we have 90% volunteer by physician or nurse during a medical event." But what about liability? "Although U.S. health care providers traveling on registered U.S. airlines have no legal obligation to assist in the event of a medical emergency, ethical obligations may prevail," according to a 2015 study, also published in the New England Journal of Medicine. "In addition, many other countries, such as Australia and in Europe do impose a legal obligation to assist," according to researchers at the Georgetown University School of Medicine. To encourage medical professionals to assist, Congress passed the Aviation Medical Assistance Act in 1998, which protects providers who respond to in-flight medical emergencies from liability and thus encourages medical professionals to assist. "This law applies to claims arising from domestic flights and most claims arising from international flights involving U.S. carriers or residents," the authors of the 2015 study wrote. "The AMAA does allow for liability of providers if the patient can establish that the provider was 'grossly negligent' or intentionally caused the alleged harm ... An example of such disregard would be an intoxicated physician treating a patient." Worst-case scenario Among in-flight medical emergencies, cardiac arrest is very rare, accounting for only 0.3% of such emergencies, yet it is responsible for 86% of in-flight deaths, according to the 2013 study. When possible, protocol recommends the deceased passenger should be left in place or placed out of the direct view of other passengers (possibly in the lavatory). Flight attendants are also advised to relocate nearby customers to alternate seats when possible. A blanket can be used to cover the customer as needed. The flight deck crew is also instructed to inform the airline's operations center to make appropriate arrangements once the aircraft is on the ground. As with any in-flight emergency, the situation is evaluated on a case-by-case basis and flight attendants are advised to use their best judgment. Air rage is a real thing, but the biggest problem is much simpler Psychiatric issues constitute 3.5% of in-flight medical emergencies, according to the 2015 study. "Potential stressors include a lengthy check-in process, enhanced security measures, delayed flights, cramped cabins and alcohol consumption," the researchers wrote. "Acutely agitated passengers pose considerable safety concerns." The most common problem in flight, though, is actually dehydration. And there's a reason you feel dehydrated when you travel. "Passenger aircraft cabins are pressurized by air pumped through the engines, which results in a relatively arid environment," according to Georgetown University researchers. "As such, many passengers are somewhat dehydrated." The simplest, but most significant piece of advice: Stay hydrated. That means drinking of plenty of water and avoiding alcohol when you fly.
And if you take any medications, pack them in your carry-on. They won't do you any good in the cargo hold. In-Flight Medical Emergencies Posted by Carla Rothaus • September 4th, 2015
When a medical emergency occurs during a commercial flight, health care providers should be prepared to respond. A new review article offers guidance on how to respond to the more common emergencies and on roles and liabilities in offering medical assistance aboard an airplane. Estimating the frequency of in-flight medical events is challenging because no mandatory reporting system exists. A study of a ground-based communications center that provides medical consultative service to airlines estimated that medical emergencies occur in 1 of every 604 flights. This is likely to be an underestimate, however, because uncomplicated issues are probably underreported.
When the problem is more serious
"If it can happen on the ground, it's going to happen in the air, as well, so we need to be able to respond to that appropriately," said Delta flight attendant trainer Justin Eberle. "Passenger safety is always our number one priority."
All flight attendants working routes in the United States must be trained in CPR and how to use a defibrillator.
"The flight attendants have access to what we call a medical accessory kit," said Martin. "That's got basic equipment in it for taking blood pressure, thermometers, personal protective equipment. If there's a medical volunteer on board, then they're given access to our emergency medical kit, and that kit has resuscitation equipment, IV equipment, medications."
Many airlines require consultation with a ground-based physician, such as STAT-MD, before the emergency medical kit is used. There is one other prominent medical communications center in the United States called MedAire, based in Phoenix, Arizona, but those calls may not always be answered by a medical doctor.
Kits vary widely in quality. The FAA requires contents such as saline solution, aspirin, antihistamines, epinephrine and nitroglycerine tablets. Some airlines choose to supplement the basic provisions, but supplies and medications are expensive, they take up weight and they have to be replaced when they expire.
It goes without saying, too, that some protocols and procedures are more challenging in the air. A simple stethoscope, for example, is rendered relatively useless in flight because of all the ambient noise.
'Is there a doctor on the plane?'
More useful, often, than the equipment is the expertise of a fellow passenger. Physician passengers provided medical assistance in 48.1% of reported in-flight medical emergencies, according to the 2013 study. Nurses assisted in 20.1% of the cases.
Martin says the number is even higher.
"Over the years, we've seen at least an 80% presence of a physician or RN volunteer," said Martin. "In fact, the most recent year we compiled data on, 2014, we have 90% volunteer by physician or nurse during a medical event."
But what about liability?
"Although U.S. health care providers traveling on registered U.S. airlines have no legal obligation to assist in the event of a medical emergency, ethical obligations may prevail," according to a 2015 study, also published in the New England Journal of Medicine.
"In addition, many other countries, such as Australia and in Europe do impose a legal obligation to assist," according to researchers at the Georgetown University School of Medicine.
To encourage medical professionals to assist, Congress passed the Aviation Medical Assistance Act in 1998, which protects providers who respond to in-flight medical emergencies from liability and thus encourages medical professionals to assist.
"This law applies to claims arising from domestic flights and most claims arising from international flights involving U.S. carriers or residents," the authors of the 2015 study wrote. "The AMAA does allow for liability of providers if the patient can establish that the provider was 'grossly negligent' or intentionally caused the alleged harm ... An example of such disregard would be an intoxicated physician treating a patient."
Worst-case scenario
Among in-flight medical emergencies, cardiac arrest is very rare, accounting for only 0.3% of such emergencies, yet it is responsible for 86% of in-flight deaths, according to the 2013 study.
When possible, protocol recommends the deceased passenger should be left in place or placed out of the direct view of other passengers (possibly in the lavatory).
Flight attendants are also advised to relocate nearby customers to alternate seats when possible. A blanket can be used to cover the customer as needed. The flight deck crew is also instructed to inform the airline's operations center to make appropriate arrangements once the aircraft is on the ground.
As with any in-flight emergency, the situation is evaluated on a case-by-case basis and flight attendants are advised to use their best judgment.
Air rage is a real thing, but the biggest problem is much simpler
Psychiatric issues constitute 3.5% of in-flight medical emergencies, according to the 2015 study.
"Potential stressors include a lengthy check-in process, enhanced security measures, delayed flights, cramped cabins and alcohol consumption," the researchers wrote. "Acutely agitated passengers pose considerable safety concerns."
The most common problem in flight, though, is actually dehydration. And there's a reason you feel dehydrated when you travel.
"Passenger aircraft cabins are pressurized by air pumped through the engines, which results in a relatively arid environment," according to Georgetown University researchers. "As such, many passengers are somewhat dehydrated."
The simplest, but most significant piece of advice: Stay hydrated. That means drinking of plenty of water and avoiding alcohol when you fly.
And if you take any medications, pack them in your carry-on. They won't do you any good in the cargo hold.
In-Flight Medical Emergencies Posted by Carla Rothaus • September 4th, 2015 When a medical emergency occurs during a commercial flight, health care providers should be prepared to respond. A new review article offers guidance on how to respond to the more common emergencies and on roles and liabilities in offering medical assistance aboard an airplane.
Clinical Pearls
• Is cardiac arrest one of the more common in-flight emergencies? Among in-flight medical emergencies, cardiac arrest is quite rare, accounting for only 0.3% of such emergencies, yet it is responsible for 86% of in-flight events resulting in death. Syncope and presyncope are relatively common medical events; in one study, these conditions accounted for 37.4% of all aircraft medical emergencies. Seizures and postictal states account for 5.8% of aircraft emergencies, and complications from diabetes account for 1.6%. Psychiatric issues constitute 3.5% of in-flight medical emergencies. Suspected strokes account for approximately 2% of in-flight medical emergencies. • What resources are available for managing an in-flight medical emergency? The Federal Aviation Administration (FAA) mandates that United States-based airlines carry first-aid kits that are stocked with basic supplies such as bandages and splints. At least one kit must contain the additional items listed in Table 1 (see below). At least one automated external defibrillator (AED) must be available. These supplies are not comprehensive (e.g., there are no pediatric or obstetrical supplies). Because health professionals are not aboard every flight, most airlines contract with ground-based medical consultation services. The clinicians at these centers can provide treatment recommendations. On-board volunteer providers can also consult these services during an emergency. The FAA also mandates that flight attendants receive training every other year in cardiopulmonary resuscitation and the use of AEDs.
Morning Report Questions
Q: What option may be considered, in addition to supplemental oxygen, to improve oxygenation in patients who develop respiratory compromise during a commercial flight? A: Supplemental oxygen should be provided if the clinician suspects respiratory compromise, and the clinician might request a descent to a lower altitude to improve oxygenation. Because of Dalton’s law and because commercial airliners are usually pressurized to the equivalent altitude of 6000 to 8000 ft, passengers typically have a partial pressure of arterial oxygen of 60 mm Hg (at sea level, it is normally 75 to 100 mm Hg). A descent in altitude may permit higher pressures of oxygen, though at a risk of the use of more fuel, because fuel consumption is greater at lower altitudes. Q: Do physicians have a legal obligation to provide assistance for an in-flight medical emergency, and what legal protections are in place for doing so? A: Liability is generally determined under the law of the country in which the aircraft is registered, but the law of the country in which the incident occurs or in which the parties are citizens could arguably apply. Although U.S. health care providers traveling on registered U.S. airlines have no legal obligation to assist in the event of a medical emergency, ethical obligations may prevail. In addition, many other countries, such as Australia and many in Europe, do impose a legal obligation to assist. In 1998, Congress passed the Aviation Medical Assistance Act (AMAA), which protects providers who respond to in-flight medical emergencies from liability and thus encourages medical professionals to assist in emergencies. This law applies to claims arising from domestic flights and most claims arising from international flights involving U.S. carriers or residents. The AMAA does allow for liability of providers if the patient can establish that the provider was “grossly negligent” or intentionally caused the alleged harm. With respect to “gross negligence,” providers are liable only if they exhibit flagrant disregard for the patient’s health and safety.
{kind=link}
Be Prepared for In-Flight Medical Emergencies
ACEP News
August 2010
August 2010
By Amit Chandra, M.D., and Shauna Conry, M.D.
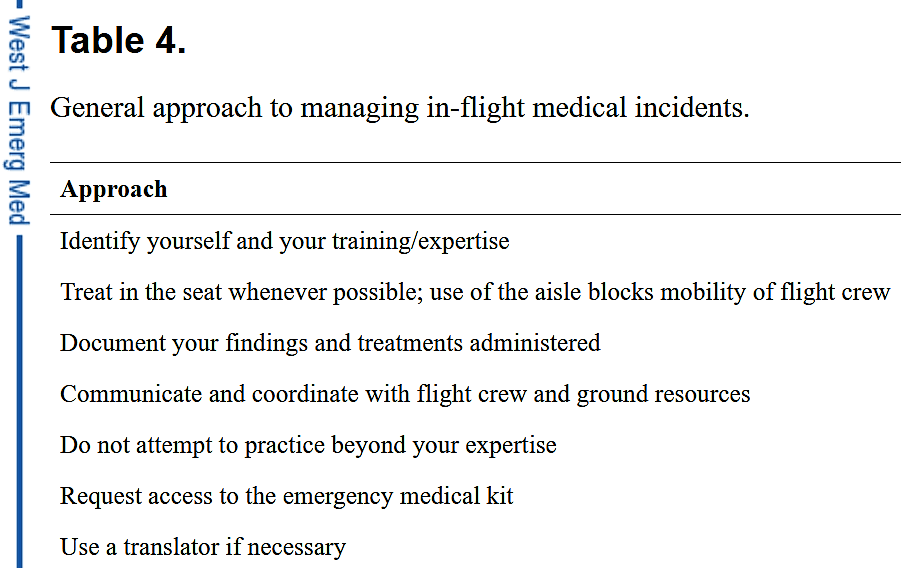
In-Flight Advice For Volunteer Docs
1. Introduce yourself to the cabin crew and state your qualifications.
2. Ask the patient for his or her permission before performing a thorough history and physical exam.
3. Use an interpreter if necessary.
4. If the patient's condition is critical, request diversion to the nearest appropriate airport.
5. Cooperate with a medical response center and coordinate with airport medical staff.
5. Cooperate with a medical response center and coordinate with airport medical staff.
6. Keep a written medical record of your patient encounter.
7. Perform only treatments you are qualified to administer.
Source: N. Engl. J. Med. 2002;346:1067-73
An overhead speaker rings several times and is followed by a brief burst of static.
"Ladies and gentlemen, if there is a medical doctor on board, please notify the nearest flight attendant. Once again, if there is a medical doctor on board, please notify the nearest flight attendant."
On a recent US Airways flight from Phoenix to Philadelphia, this announcement was followed by tragedy with the death of a 73-year-old passenger. The plane made an emergency landing in Pittsburgh, where paramedics were waiting to provide emergency care. The man was pronounced dead at the scene, and a subsequent medical examiner's report attributed the death to a cardiac condition.
Unique Aspects of In-Flight Emergencies
An emergency physician is ideally suited to volunteer to assist during an in-flight medical emergency. Emergency medicine provides a breadth of training across all age groups and organ systems. Our ability to improvise and focus on the diagnosis and immediate care of sick patients sets us apart as a specialty.
Providing medical assistance at 36,000 feet is nevertheless a daunting proposition. Lower air pressure (cabin pressure is maintained at 5,000 to 8,000 feet), cramped quarters, and the roar of engine noise make an overcrowded county ED seem an ideal working environment by comparison.
Providing medical assistance at 36,000 feet is nevertheless a daunting proposition. Lower air pressure (cabin pressure is maintained at 5,000 to 8,000 feet), cramped quarters, and the roar of engine noise make an overcrowded county ED seem an ideal working environment by comparison.
Common In-Flight Emergencies
The actual incidence of medical emergencies during commercial air travel is unknown. In a report using data from British Airways published in the BMJ in 2000, Nigel Dowdall estimated 1 in-flight emergency per 11,000 passengers. MedAire, a medical assistance company that provides remote assistance to several commercial airlines in the United States, responds to an average of 17,000 calls per year.
Common emergencies include chest pain, syncope, asthma exacerbations, and GI complaints. Air travel in the cheap seats has often been described as "economy class syndrome," a sort of midair version of Virchow's triad: dehydration, immobilization, and predisposing factors increasing the risk of deep vein thrombosis.
What's Available on a Flight?
FAA regulations require all U.S. commercial airlines weighing 7,500 pounds or more and serviced by at least one flight attendant to carry a defibrillator and an enhanced emergency medical kit. Flight attendants must be certified in CPR, including the use of an AED, every 2 years. Pilots must also be trained in the use of the AED.
An emergency physician responding to an in-flight emergency is unlikely to have an ACLS cart packed in his or her carry-on luggage. The standard emergency medical kit, which is based on recommendations by the Aerospace Medical Association's (AsMA) air transport medicine committee, includes a stethoscope, syringes and IV catheters in a range of sizes, and commonly used medications (see box).
While most domestic airlines carry this kit, there are no international regulations requiring the complete kit to be available.
What Are Your Options?
There are no federal regulations or guidelines on the management of an in-flight medical emergency. A growing number of airlines now utilize the services of remote emergency response centers. MedAire, for example, offers 24-hour consultation via call centers staffed by emergency physicians. If medically trained passengers volunteer their assistance, they are required to work with cabin crew and the response center's physician. If there is no call made to a call center, the volunteer physician must work with cabin crew and can suggest treatment or diversion options.
Medical-Legal Liability
Federal legislation contained in the Air Carrier Access Act of 1998 has provided limited protection and guidance for physicians and other medical professionals who volunteer their services during flight. Volunteers must be "medically qualified," render care in good faith, and receive no monetary compensation to be protected under this Act.
The legislation states that "an individual shall not be liable for damages in any action brought in a Federal or State court arising out of the acts or omissions of the individual in providing or attempting to provide assistance in the case of an in-flight medical emergency unless the individual, while rendering such assistance, is guilty of gross negligence or willful misconduct."
There are no documented cases of a physician being sued for providing assistance during an in-flight emergency. A review article published in 2002 by Grendau and DeJohn in the New England Journal of Medicine offers several suggestions for physicians who volunteer to help during an in-flight emergency (see box).
Other Resources
Several organizations currently work in the field of aviation medicine, including AsMA, the International Air Transport Association (IATA), and the International Civil Aviation Organization (ICAO). Many members of these organizations have advocated in recent years for a registry of in-flight medical emergencies to assist with research, training, and quality improvement.
Dr. Claude Thibeault, medical adviser for the IATA and member of the Air Transport Medicine committee of the AsMA, said, "If we had a good repository of data, that would help when we stock the medical kits. [The kits] are based on opinions, not data."
Dr. Claude Thibeault, medical adviser for the IATA and member of the Air Transport Medicine committee of the AsMA, said, "If we had a good repository of data, that would help when we stock the medical kits. [The kits] are based on opinions, not data."
No matter how well stocked the kits are, in-flight medical emergencies are inevitable given the size of the commercial airline industry. According to Dr. Thibeault, "People don't realize that an aircraft is a taxi; it is not meant to transport sick people. But because it transports so many people, it is bound to transport a sick person once in while."
He also said an equal measure of the debate on this issue should focus on prevention, and "emphasis should be placed on the physician's responsibility to tell patients whether or not they should travel."
For now, emergency physicians who are frequent fliers can familiarize themselves with in-flight medical resources. And when it comes to responding to a medical emergency during commercial air travel, expect the unexpected.
DR. CHANDRA is a faculty member and a practicing emergency physician at New York Hospital Queens. DR. CONRY is a first-year emergency medicine resident at New York Hospital Queens.
The Emergency Medical Kit
{kind=link}
Medications
Epinephrine 1:1,000
Antihistamine, injectable (inj.)
Dextrose 50%, inj. 50 mL (or equivalent)
Nitroglycerin tablets or spray
Major analgesic, inj. or oral
Sedative anticonvulsant, inj.
Antiemetic, inj.
Bronchial dilator inhaler
Atropine, inj.
Corticosteroid, inj.
Diuretic, inj.
Medication for postpartum bleeding
Normal saline
Acetylsalicylic acid for oral use
Oral beta-blocker
Epinephrine 1:10,000
List of medications: generic name plus trade name if indicated on the item
Antihistamine, injectable (inj.)
Dextrose 50%, inj. 50 mL (or equivalent)
Nitroglycerin tablets or spray
Major analgesic, inj. or oral
Sedative anticonvulsant, inj.
Antiemetic, inj.
Bronchial dilator inhaler
Atropine, inj.
Corticosteroid, inj.
Diuretic, inj.
Medication for postpartum bleeding
Normal saline
Acetylsalicylic acid for oral use
Oral beta-blocker
Epinephrine 1:10,000
List of medications: generic name plus trade name if indicated on the item
Equipment
Stethoscope
Sphygmomanometer
Airways, oropharyngeal
Syringes
Needles
IV catheters
Antiseptic wipes
Gloves
Sharps disposal box
Urinary catheter
Intravenous fluid system
Venous tourniquet
Sponge gauze
Tape adhesive
Surgical mask
Flashlight and batteries
Thermometer (nonmercury)
Emergency tracheal catheter
Umbilical cord clamp
Basic life support cards
Advanced life support cards
Sphygmomanometer
Airways, oropharyngeal
Syringes
Needles
IV catheters
Antiseptic wipes
Gloves
Sharps disposal box
Urinary catheter
Intravenous fluid system
Venous tourniquet
Sponge gauze
Tape adhesive
Surgical mask
Flashlight and batteries
Thermometer (nonmercury)
Emergency tracheal catheter
Umbilical cord clamp
Basic life support cards
Advanced life support cards
Source: Aerospace Medical Association
More: In-flight Medical Emergencies {kind=link}
The Art of EMS
by Steve Whitehead
8 tips for responding to in-flight emergencies Now that I have half a dozen or so of these experiences under my belt, here’s what to expect when responding to a medical assistance call on a flight
Now that I have half a dozen or so of these experiences under my belt, here’s what to expect when responding to a medical assistance call on a flight
Original from www.ems1.com
Last night I went to a Tai Kwon Do black belt testing to watch a friend who was testing for a fourth-dan master belt. It was a pretty impressive affair, capped off by watching my friend break a tall stack of bricks, and break his hand in the process. He then proceeded to walk around the forum shaking hands with everyone using his bloody, broken hand.
I was invited to attend because of a friendship, but it was also made clear by several of the instructors that it would be nice if I could come, you know … "just in case."
This sort of thing happens to all of us from time to time.
As cliché as it sounds, very few of us really take off the uniform when our work day is over. Being an EMT or a paramedic is a 24/7 job.
Our neighbors know that we work in emergency services. Our friends and family look to us for advice and medical guidance.
Happy to help
I’m not complaining. I wouldn’t want it any other way.
In fact, I get a little perturbed when friends or family describe a significant injury or illness that they didn’t tell me about because, "Well, we just didn’t want to bother you."
And don’t even get me started on the time when my father, visiting from out of state, drove himself to the hospital with chest pain because he didn’t want to wake me up.
I think most of us make peace with the fact that we are always on call to some extent. In fact, the majority of us prefer it. I don’t know if it’s like this in other professions. I’ve been in emergency service for my entire working career.
I’m not sure if construction workers or accountants get called to ply their trade outside of their work environment, or if tax preparers ever get the urgent knocks on their door from neighbors who are about to miss a filling deadline.
I don’t know if people who work in sales get calls from friends asking for advice on how to best word their Ebay furniture description or if dental hygienists get asked about the best toothbrush.
I do know that I’ve never heard any of them called for while flying on an airplane.
I have, on several occasions, heard urgent requests for medical assistance while flying. I’ve even responded to these requests when the call went unanswered.
The first time I stood up and offered my help to the flight crew, I had no idea what to expect. Now that I have half a dozen or so of these experiences under my belt, I thought I might pass on a few tips for responding to in-flight emergencies.
1. Don’t depend on the flight crew for medical assistance
They are trained in basic CPR and AED operations. They also receive some basic medical training as part of their annual required emergency training.
They will be more than happy to take direction and bring you things that you need, but they are not clinicians. They are typically very happy to receive your assistance but, for the most part, they will leave the emergency to you.
2. You won’t be the only one
United Airlines reports that three out of four requests for assistance are answered by a qualified medical professional, so it’s likely you won’t be the only one who responds to the call for assistance.
Talk with the other medical providers and decide who would like to take the lead and who would like to assist. Don’t assume that you are the most qualified person to take care of the patient.
Having said that, don’t automatically differ to the highest level of training. A family practice physician or a pediatric nurse may be more comfortable assisting than leading the patient evaluation.
3. Have your ID handy
The plane will likely have a fairly extensive medical kit, but don’t expect to get your hands on it without proper identification. The crew will accept your help, but they can only turn the kit over to someone who has a valid medical identification.
If you don’t have the proper ID, they may not even tell you that the kit exists.
4. Know what you have to work with
Inside the kit you’ll find a blood pressure cuff and a stethoscope, as well as IV supplies, first round cardiac arrest medications and several commonly used emergency medications.
You may also find intubation supplies and basic trauma dressings. Don’t forget you have an AED available as well. Call for it sooner rather than later if you think you might need it.
They also should have supplemental oxygen for one person for the duration of the flight, but if you are using high flow rates you may want to assess the supply. Flight attendants can also apply oxygen but will probably prefer to let you do it.
5. Know your limits
Regardless of what medical equipment is made available to you, you are still obligated to stay within the limits of your scope of practice, your training and your local protocols. Make good clinical decisions and don’t get too far out in the weeds when you’re operating off-duty and outside of your response area.
6. Clear some space
You can ask to move passengers around if you and the patient need more room. Unless the flight is filled, the crew should be able to accommodate you.
You’ll have to decide if you’d prefer to assist the patient and return to your seat to check on them periodically, or if you’d like to remain with them for the duration of the flight.
7. Phone for help if necessary
It’s a good idea to keep your local ER phone numbers in your cell phone. Most planes have several options to make a phone call from inside the plane.
If you’re assisting with a medical emergency, your local doctors back home should be more than happy to help you out with some advice and direction.
8. Advise an emergency landing
If you deem the emergency significant enough to divert to an alternate location, you’ll need to speak with the captain about your options. Remember that you are only there to advise and recommend. It isn’t your aircraft and it isn’t your emergency.
Depending on your location and a myriad of other factors, landing the plane at an alternate location might not be possible even for the most critical of medical emergencies. Act in the patient’s best interest, but understand that diverting to an alternate airport isn’t as easy as steering an ambulance toward a different hospital.
Sometimes, answering the call for assistance on a day off, especially in the middle of a busy travel day at 30,000 feet above ground can be an inconvenience, but most of us wouldn’t want it any other way.
Hopefully, the next time you hear a request for assistance on an airplane, you’ll feel a bit more comfortable about offering your help.
About the author
Steve Whitehead, NREMT-P, is a firefighter/paramedic with the South Metro Fire Rescue Authority in Colo. and the creator of blog The EMT Spot. He is a primary instructor for South Metro's EMT program and a lifelong student of emergency medicine. Reach him through his blog at steve@theemtspot.com or at Steve.Whitehead@EMS1.com.
Related: http://www.ems1.com/pediatric-care/articles/2016286-Doctor-treats-toddler-in-cardiac-arrest-on-plane/
"Some times the Onboard Health professional must think and make inventor to save a life"
| Table 1 Study characteristic and incidence of in-flight medical emergencies Go to the Table 1 link |
{kind=link}
| Table 2 In-flight emergencies by diagnosis Go to the Table 2 link |
{kind=link}
| Table 3 In-flight emergencies by diagnosis Go to the Table 3 link |
{kind=link}
| Table 3 cont In-flight emergencies by diagnosis Go to the Table 3 link |
{kind=link}
| Table 4 In-flight emergencies by diagnosis Go to the Table 4 link |
{kind=link}
| Table5 In-flight emergencies by diagnosis Go to the Table 5 link |
{kind=link}
Is there a doctor on board? In-flight medical emergencies
{kind=link}
Doctor Channels MacGyver to Help Asthmatic Toddler Aboard Transatlantic Flight
Improvised nebulizer during In-flight Medical Emergencies
{kind=link}
{kind=link}
| In-flight emergencies Dr. Ramon REYES DIAZ, MD AA American Airlines |
{kind=link}
| In-flight emergencies Dr. Ramon REYES DIAZ, MD Iberia Airlines |
{kind=link}
|
{kind=link}
American Airlines
December 10, 2015
Dear Dr. Ramon Reyes Diaz:
Please accept our company's formal "Thank You" for the assistance you provided aboard your recent flight. We are all grateful that you were on board and freely offered your medical expertise when it was needed most. Without a doubt, you greatly improved a difficult situation.
As a tangible expression of our appreciation for volunteering your time and experience, we have added 50,000 miles to your AAdvantage® account. This mileage adjustment should appear in your account in a few days. You can view your account viahttp://www.aa.com/aadvantage. These miles can also be used to claim AAdvantage® awards.
I realize your offer of assistance was not motivated by any potential reward. Nevertheless, we wanted you to know how much your efforts were appreciated -- and that we look forward to serving you again soon. It will be our privilege to welcome you aboard American when your plans call for travel by air.
Sincerely,
Dr. Jeral Ahtone, MD.
Director, Medical and
Occupational Health Services
AA Ref#1-5004788459
| Dr. Ramon A. Reyes Diaz, MD How airlines deal with in-flight medical emergencies 1 in every 604 flights involves medical situation, study says. In-flight Medical Emergencies "Be Prepared" |
{kind=link}
"Hoy 08 Diciembre 2015, después de tantas emergencias manejadas en vuelos comerciales, he te nido una que me ha impactado. 86 años parada cardíaca súbita, vuelo Dallas-Miami (aterrizaje de emergencias en New Orleans). Luego de nuestro esfuerzo y de las chicas de sobrecargo de American Airlines y una enfermera de EUA, pudimos recuperar la paciente y entregarla a los médicos del aeropuerto de Lousiana con TA 130/80 Oxymetria 97% FC: 86 totalmente consciente y orientada en tiempo y espacio. Gracias RCP-AHA, Gracias AED, Gracias TEAM Work, Gracias. Salir del Avion con alausos de más de 300 personas y que el capitan te espere a la salida en posicion de atencion en señal de agradecimiento y respeto. Coño gracias medicina bendita que arrebatas a la muerte parte de su trabajo." Gracias mil veces a la mas noble de las profesiones. gracias por permitirme hacer medicina con dignidad y gracias por el respeto al esfuerzo sin esperar nada a cambio" By Dr. Ramón Reyes Diaz, MD
Articulo relacionado
How airlines deal with in-flight medical emergencies 1 in every 604 flights involves medical situation, study says. In-flight Medical Emergencies "Be Prepared" http://goo.gl/tQiWMi
LIBROS MEDICINA Y SALUD
https://www.facebook.com/ pg/DrRamonReyesMD/photos/ ?tab=album&album_id=6208833
Articulo relacionado
How airlines deal with in-flight medical emergencies 1 in every 604 flights involves medical situation, study says. In-flight Medical Emergencies "Be Prepared" http://goo.gl/tQiWMi
| How airlines deal with in-flight medical emergencies 1 in every 604 flights involves medical situation, study says. In-flight Medical Emergencies "Be Prepared" |
{kind=link}
https://www.facebook.com/ pg/DrRamonReyesMD/photos/ ?tab=album&album_id=6208833
Free PDF IATA Medical Manual 11th Edition June 2018/ Manual Medico de IATA "International Air Transport Association"
Covid-19: Mapa interactivo de restricciones de Viajes by IATA/ Timatic
IATA propone una estrategia de seguridad multinivel para la reanudación de la industria. Covid-19
¿Fallecimiento de pasajero en Vuelo? Protocolo IATA
¿Cuales son las posibilidades de ser in infectado en un Avión de Coronavirus?
¿QUE ES TELEMEDICINA? Marco de implementación de un Servicio de Telemedicina OMS / OPS pdf
How airlines deal with in-flight medical emergencies? 1 in every 604 flights involves medical situation, study says. In-flight Medical Emergencies "Be Prepared"
Guidance for Vaccine and Pharmaceutical Logistics & Distribution IATA by IATA. Covid-19
LIBROS GRATIS #PDF solo dirígete al enlace de las fotos y allí tienes el enlace en donde puedes descargar de forma legal y sin trucos tu libro. Dr. Ramon Reyes, MD @DrRamonReyesMD https://lnkd.in/eVpFyzZ #DrRamonReyesMD
Blog EMS SOLUTIONS INTERNATIONAL
¿Quién es el Dr. Ramon Reyes, MD?
Blog 8,302,914 visitas por IP https://lnkd.in/daWAMq9
Twitter 422 seguidores
https://lnkd.in/ekwWq-f
LinkedIn 5451 seguidores
https://lnkd.in/dnPGwGY
Pinterest 4170 seguidores Mas de 628,000 visitas mensuales
https://lnkd.in/dareieA
Instagram 3728 seguidores
https://lnkd.in/eQsjZsz
Facebook 99329 seguidores
https://lnkd.in/e7P6RTa
Facebook del Blog EMS SSOLUTIONS INTERNATIONAL
62852 seguidores
https://lnkd.in/dyeuGFwh
Grupo de TELEGRAM EMERGENCIAS 4327 miembros
https://lnkd.in/eVUqu5a
Grupo de TELEGRAM TACMED 613 miembros
https://t.me/CIAMTO
Luces de aeronaves. Aviones
https://emssolutionsint.blogspot.com/2022/12/luces-de-aeronaves-aviones.html
Medicina Aeronáutica: Conceptos Generales (Libro) PDF Gratis https://emssolutionsint.blogspot.com/2018/07/medicina-aeronautica-conceptos.html
MEDEVAC / TACEVAC / CASEVAC / AROMEDICINA / TRANSPORTE AEROMEDICO
https://emssolutionsint.blogspot.com/2019/08/medevac-tacevac-casevac-aromedicina.html
IATA Medical Manual / Manual Medico de IATA "International Air Transport Association" Free PDF https://emssolutionsint.blogspot.com/2011/05/iata-medical-manual-manual-medico-de.html
Les esperamos en nuestro grupo en TELEGRAM