



What They Did:
- Sub study of the High Sensitivity Cardiac Troponin T assay for rapid Rule-out of Acute Myocardial Infarction
- ≈1300 patients from 12 centers in Europe, USA, and Australia evaluated
- Multicenter, international diagnostic study evaluating patients for a rapid rule-out AMI protocol using a 1-hour high sensitivity cTnT
Outcomes:
- Performance characteristics of symptoms for ACS
Inclusion:
- Patients presenting to the ED with symptoms suggestive of AMI
- Onset or maximum discomfort within the previous 5 hours
Exclusion:
- Renal failure requiring HD
- Trauma
- Cardioversion
- Defibrillation
- Thrombolytic therapy
- CABG within the prior 30 days
- Hospitalized for AMI within the last 3 weeks
- Pregnant and breastfeeding women
Results:
- 213/1282 (17%) AMI rate
- 21 STEMIs
- 192 NSTEMIs
- 4 Independent Predictors for Diagnosis of AMI:
- Radiation to Right Arm or Shoulder: OR 3.0; 95% CI 1.8 – 5.0
- 10% of entire study cohort
- Chest Pressure: OR 2.5; 95% CI 1.3 – 4.6
- 70% of entire study cohort
- Worsened by Physical Activity: OR 1.7; 95% CI 1.2 – 2.5
- 30% of entire study cohort
- Radiation to Left Arm or Shoulder: OR 1.7; 95% VI: 1.1 – 2.4
- 35% of entire study cohort
- Patients with more than 1 of these symptoms were more likely to have AMI
- Radiation to Right Arm or Shoulder: OR 3.0; 95% CI 1.8 – 5.0
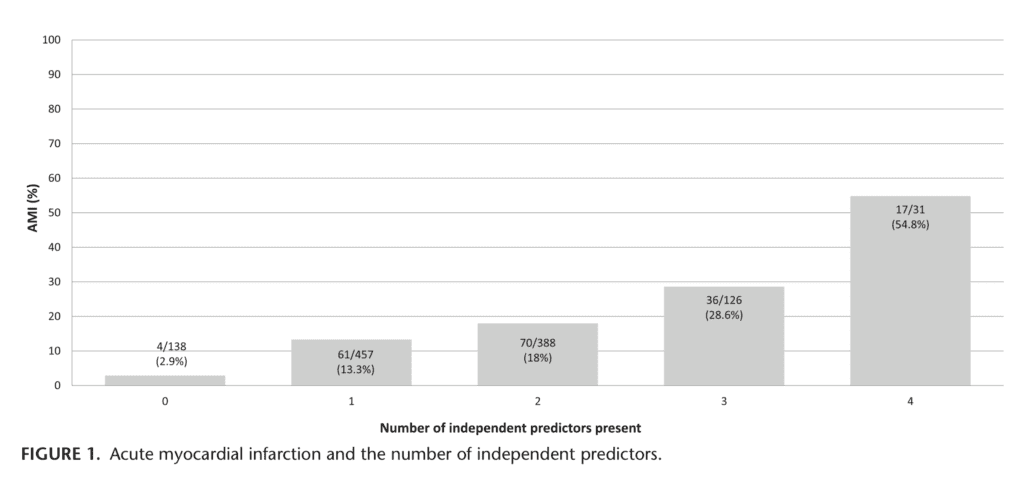

- If all 4 symptoms present, 55% of these patients had a diagnosis of AMI, but there were only 31/1282 (2.4%) of patients with all 4 symptoms in this study
- Relationship between myocardial infarct size and AMI symptoms. Statistically significant, symptoms in the highest troponin T quartile cohort (Troponin T ≥5300ng/L) were:
- Right arm/shoulder radiation (33.3% of pts; P = 0.014)
- Cervical radiation (24.1%; P = 0.02)
- Supramammillary right location (22.2% of pts; P = 0.009)
- Pulling chest pain (7.4% of pts; P = 0.037)
- Ventral radiation (pain to the back) (3.7%; P = 0.018)
Strengths:
- AMI adjudicated by 2 independent cardiologists
- Symptoms prospectively recorded
- Used high sensitivity cTn. Most prior studies have used CK-MB and older definitions of AMI
- Multicenter study. Most prior studies were single center
- Used multivariate analysis in evaluating patients.Most prior studies did not use this statistical method to determine independent predictors of AMI
- Definite ECG interpretation was not required before inclusion which ensures a large patient population with chest pain included for analysis
- First study to report on size of MI and correlate with specific symptoms
Limitations:
- Only patients with chest pain included in this study. Many patients with AMI will not present with chest pain as their primary symptom (i.e. atypical symptoms)
- Diaphoresis, syncope and change in mental status were not recorded in this study
- Patents with atypical, non-cardiac symptoms may not have been enrolled in this study if clinical suspicion of MI was low which could introduce a bias against symptoms that might be predictive of non-AMI
Discussion:
- Although in previous studies pleuritic chest pain, sharp chest pain, positional chest pain, or chest pain that is worse with palpation have been symptoms that were associated with a non-AMI diagnosis, no symptoms in this study were independently associated with a non-AMI diagnosis
- Swap CJ et al. JAMA 2005 – Decreased Likelihood of AMI [2]:
- Described as Pleuritic Pain: LR 0.2 (95% CI 0.1 – 0.3)
- Described as Positional Pain: LR 0.3 (95% CI 0.2 – 0.5)
- Described as Sharp Pain: LR 0.3 (95% CI 0.2 – 0.5)
- Reproducible Pain with Palpation: LR 0.3 (95% CI 0.2 – 0.4)
- Panju AA et al JAMA 1998 – Decreased Likelihood of AMI [3]:
- Pleuritic Chest Pain: LR 0.2
- Chest Pain that is Sharp or Stabbing: LR 0.3
- Positional Chest Pain: LR 0.3
- Chest Pain Reproduced by Palpation: LR 0.3
- There was also no correlation between duration of symptoms and diagnosis of AMI in this study
Author Conclusion:“In this large multicenter trial, only 4 symptoms were associated with the diagnosis of AMI, and no symptoms that were associated with a non-AMI diagnosis.”
Clinical Take Home Point: Pay closer attention to patients with chest pain that radiates to their right arm. In this multicenter study of patients with chest pain presenting to the ED, chest pain radiation to the right arm is more predictive of AMI than chest pain radiating to the left arm.
References:
- McCord J et al. Symptoms Predictive of Acute Myocardial Infarction in the Troponin Era: Analysis From the TRAPID-AMI Study. Crit Pathw Cardiol 2019. PMID: 30747759
- Swap CJ et al. Value and Limitations of Chest Pain History in the Evaluation of Patients with Suspected Acute Coronary Syndromes. JAMA 2005. PMID: 16304077
- Goodacre S et al. How Useful are Clinical Features in the Diagnosis of Acute, Undifferentiated Chest Pain? Acad Emerg Med 2002. PMID: 11874776
For More on This Topic Checkout:
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post TRAPID-AMI: Predictive Symptoms of Acute Myocardial Infarction (AMI) appeared first on REBEL EM - Emergency Medicine Blog.