
Salt Lake City, UT is at an elevation of 4226 ft above sea level. This flirts with the lower cutoff for a high altitude environment where minor hypoxemia is known to occur. A high altitude environment has an elevation between 1500-3500m (4921-11,483ft). (Wilderness medicine, Auerbach et al. 4th edition, 2001. Chapter 1, High Altitude Medicine: Peter H Hackett, Robert C Roach.)
Salt Lake City is not the only major population center in a high altitude environment:
- Santa Fe, NM. 7298 ft.
- Flagstaff, AZ. 7000 ft.
- Denver, CO. 5160 ft.
- Bozeman, MT. 4793 ft.
- Fort Davis, TX. 4900 ft.
- Mexico City, Mexico. 7380 ft.
- San Antonio, TX. 650 ft. (Salim’s hometown)
It is possible to calculate a ‘normal’ oxygen saturation for any elevation above sea level. This altitude adjusted ‘normal’ saturation level can then be used within the PERC rule.
For those of you whose last physics class was last century, there is a dizzying amount of physics and math involved in the calculation of altitude adjusted normal oxygen saturation that will be left to the end of the post.
Rather than relying on scientifically valid projections of expected oxygen saturations and optimistically applying those numbers to our high altitude centers we can consider data from a prospective validation of the PERC rule performed at altitude (5280 ft) that used an oxygen saturation cutoff of 90% instead of 95%. [cite source=”pubmed”]18272098[/cite]
Assessment of the Pulmonary Embolism Rule-Out Criteria Rule for Evaluation of Suspected Pulmonary Embolism in the Emergency Department.
Study Design:
- This was a secondary analysis of a prospectively collected database for the validation of Wells criteria. [cite source=”pubmed”]15520710[/cite]
Population:
- Data collected from August 2001-June 2002 at a community emergency department in Colorado. All data were collected before the publication or presentation of the PERC rule.
- Consecutive patients in 120 randomly generated 8 hour shifts with clinical suspicion for PE.
Excluded:
- Non English speaking
- Recently (<6months) or currently pregnant
- Morbidly Obese (>350lb) (CT scanner weight limit)
- Prior non-cancer related diagnosis of thrombophilia
- Age <18 or >85 years
- Critically ill / unable to consent
- Known recent D-dimer value (either normal, or elevated)
Measurements:
- Oxygen saturation was measured with pulse oximetry (not via ABG)
- All patients had either CT pulmonary angiogram or V/Q scan to evaluate for presence of PE on initial presentation.
- Each of the PERC rule variables were dichotomized and considered negative if they met the prespecified PERC rule criteria, with the exception of the oxygen saturation cutoff. If the oxygen saturation was 90% or higher on room air the variable was considered negative. This 90% cutoff was used to adjust for the altitude (5280 ft).
Outcomes:
- Diagnosis of PE after initial evaluation
- Diagnosis of any venous thromboembolism during 3 month follow up
- Death due to venous thromboembolism
Results:
- 176 patients were eligible for enrollment during the study period.
- 23 were excluded (2 patients met 2 of the exclusion criteria)
- 7 for age exclusion
- 6 for known D-dimer
- 4 for recent / current pregnancy
- 3 for morbid obesity
- 3 for critical illness / inability to consent
- 2 for being non-English speaking
- 16 patients declined to participate
- 3 patients were missed due to patient volume in the ED
- 23 were excluded (2 patients met 2 of the exclusion criteria)
- Data was examined on 134 patients
- 14 patients had PE on initial ED presentation
- 2 had VTE (1 PE, 1 DVT) on follow up
- In total, 16/132 (12%) had PE
- 19/134 (14%) patients met the criteria for the PERC rule, with a 100% sensitivity, and 16% specificity
- Of the low pretest probability patients, 13/60 (22%) met PERC rule criteria, with a 100% sensitivity
- 1/60 of these low risk patients had a PE
Altitude Adjusted PERC Oxygen Saturation:
24/126 patients had saturations <90% (13 data variables were missing, none of them impacted the PERC rule stratification as each of the patients with missing data had at least one other variable that was positive.) Of the hypoxic patients, 6 (25%) had a PE. This accounts for 38% (6/16) of all the PE patients.
Strengths:
- Prospective study
- Answers a geographically relevant clinical question with a goal of decreasing unnecessary testing
Limitations:
- Small sample size
- Single center
- Secondary analysis of previously collected data set
- Convenience sample of 120 randomly selected shifts during study period.
- Altitude adjusted saturation of 90% based on elevation (5280ft) cannot be generalized to lower elevation population centers without individualized data / calculations
- PERC rule was used on a total of 74 moderate and high risk patients who had 15 of the 16 pulmonary emboli diagnosed.
- In this study no PE’s were missed using the PERC rule on moderate and high risk patients. Despite this the PERC rule is best applied to low risk patients only.
Potential Impact to Practice:
This prospective validation of the PERC rule using an oxygen saturation cutoff of 90% can allow the consideration of an altitude adjusted oxygen saturation cutoff when using the PERC rule on low risk patients in other high elevation centers.
Intermountain Healthcare (Salt Lake City, UT) uses an electronic clinical decision tool to assist clinicians in their evaluation of patients suspected of PE. This tool uses a cutoff of 90% based on an elevation of 4226ft.
The Math:
Oxygen saturation can be calculated based on the Severinghaus equation which assumes a temperature of 37 degrees celcius, and pH of 7.4. [cite source=”pubmed”]35496[/cite]
The Severinghaus equation converts PaO2 to Oxygen saturation. The mathematical degree of difficulty involved in this equation is beyond the scope of this blog. The table below lists the conversion from PaO2 to oxygen saturation:
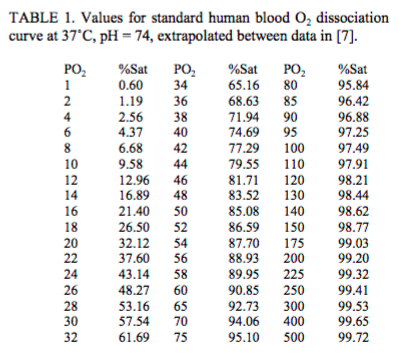{kind=link}
Table 1. Values for standard Human blood O2 dissociation curve at 37 degrees C, pH 7.4 (Severinghaus, 1979)
PaO2 is calculated by finding the PAO2 (Alveolar partial pressure of oxygen) and adjusting for the A-a gradient. A normal A-a gradient for a young adult non-smoker is between 5-10mmHg. The A-a gradient increases with age. A conservative estimate for A-a gradient is (Age/4)+4. So a 40 year old should have an A-a gradient less than 14.
- PAO2 = PIO2 – PACO2/R
- PIO2 = FiO2(Patm-PH2O)
- At higher altitude, barometric pressure (Patm) drops. With FiO2 fixed at 21%, as Patm falls, so does PIO2
- R (0.8) is the respiratory exchange ratio (CO2 produced / Oxygen consumed)
- PH2O is typically constant at 47mmHg
- PAO2 = FiO2 (Patm-PH2O) – (PaCO2/0.8)
Clinical Bottom Line:
An altitude adjusted oxygen saturation cutoff below the traditional 95% value can be used for the PERC rule when evaluating for PE in low risk patients at high elevations. Before changing to an altitude adjusted oxygen saturation cutoff all involved parties (ED, ICU, Internal Medicine, Thrombosis service, Pulmonology) should agree on the cutoff value, and the method used to calculate it.
Post Peer Reviewed By: Salim Rezaie (Twitter: @srrezaie) and Anand Swaminathan (@EMSwami)
The post Altitude Adjusted PERC Oxygen Saturation appeared first on REBEL EM - Emergency Medicine Blog.