
A 24 year-old woman presents to your Emergency Department after a motor vehicle collision. She was the restrained driver of a car that collided head-on with another vehicle. She is complaining only of chest pain and appears uncomfortable and anxious. The monitor shows sinus tachycardia and you spot a sternal fracture on her chest x-ray. After IVF and Fentanyl, she remains slightly tachycardic and you wonder:
- Do I need to send a troponin?
- If the troponin is negative does this patient need to be admitted?
- What other testing should I consider in the Emergency Department?
Blunt Cardiac Injury
Definition: There is no standard definition of blunt cardiac injury (BCI). In general, BCI refers to any blunt trauma to the heart. This can range from mild to severe injuries including:
- Cardiac contusions
- Dysrhythmias after trauma
- Ventricular wall rupture
Epidemiology:
- Estimated incidence of BCI in thoracic trauma varies greatly with reported values ranging from 8 to 71%. This large range results from a lack of clear definition and diagnostic criteria. (Pasqaule 1998 , Singh 2018 )
- One recent study found a BCI incidence of 25% among patients with blunt thoracic trauma. (Emet 2010 )
- Most commonly injured anatomy (Anterior Structures):
- Right ventricle
- Right atrium
- Less commonly injured:
- Left ventricle and atrium
- Septum, valves, and coronary arteries (extremely RARE). (Karalis 1994 )
Causes:
Suspect BCI in any patient with significant thoracic trauma or direct precordial impact including:
- Motor vehicle accidents (most common)
- Pedestrians struck by motor vehicles
- Crush injuries
- Blast injuries
- Deceleration injuries
A significant amount of force is normally required for BCI to occur. Up to 20% of death due to motor vehicle crashes is attributed to BCI. (Schultz 2004 , Singh 2018 )
{kind=link}
A word (or two) in Latin…
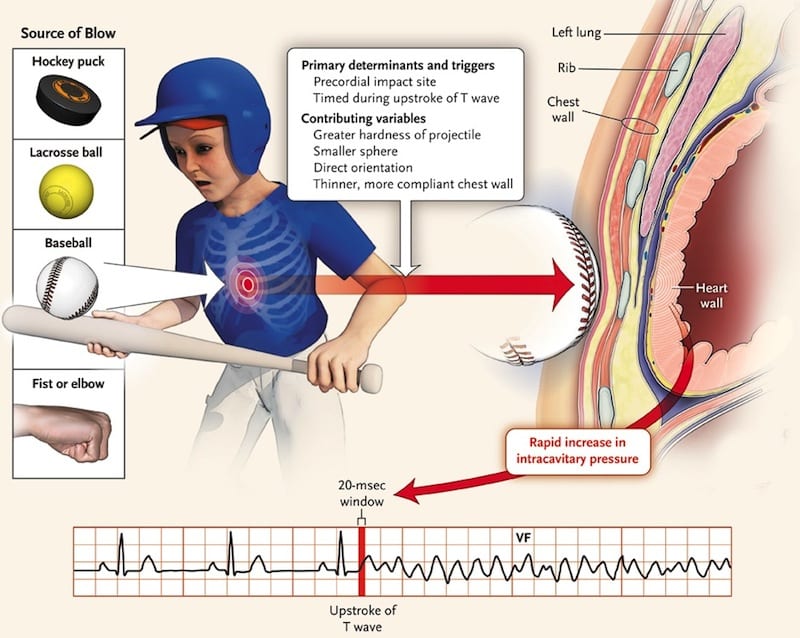
Commotio Cordis (Borjesson 2009 )
- Latin for “disturbance of the heart”
- Second leading cause of death in young athletes after hypertrophic cardiomyopathy (HCM)
- Sudden death after a seemingly low-impact blow to the chest by a hard projectile most commonly
- Baseballs
- Lacrosse balls
- Hockey pucks
- The fatal nature of the blow requires an unlucky combination of impact location, velocity, and projectile hardness occurring just milliseconds before the peak of a T wave
- This results in ventricular fibrillation followed by sudden death
Pathophysiology:
The pathophysiology of BCI depends upon which of the injuries has occurred
- Pericardial injury:Pericardial laceration, perforation, hematoma
- Atrial and Ventricular injury
- Wall rupture
- Myocardial contusions (most common and most innocuous)
- Valvular injury: Cardiac valve, papillary muscle, and chordae tendineae tears or ruptures
- Coronary vessel injury
- Intimal disruption
- Thrombosis
- Dissection
Signs & Symptoms:
- Symptoms:
- Most common symptom is chest pain
- Symptoms will widely depend on the extent of BCI
- Signs:
- Dysrhythmias (most commonly sinus tachycardia, atrial fibrillation)
- Chest wall deformities or ecchymosis
- Pulse deficits
- Hypotension
- New murmurs
- New heart failure
- Rales
- Muffled heart sounds
- Distended neck veins
- Pericardial effusion or tamponade
The most severe BCIs result in wall rupture in any of the chambers and these patients typically do not survive to ED presentation. (Shorr 1987 , Calhoon 1986 , Yousef 2014 )
Pediatric patients have increased compliance of the thoracic cavity and there may be no outward signs of trauma to raise suspicion of BCI.
Associated Injuries (Schultz 2004 ):
- Head injury
- Extremity injury
- Rib fracture
- Aortic injury
- Hemothorax
- Pulmonary contusion
- Pneumothorax
- Flail chest
- Sternal fracture
- Abdominal solid organ injury
- Spinal injury
Immediate Management:
- Clinicians should proceed with initial stabilization of the trauma patient
- Hypotension in the trauma patient should be initially approached as due to hemorrhage rather than from a purely cardiac cause
- A FAST (Focused Assessment with Sonography for Trauma) exam should be performed immediately after the primary survey is completed
- Consider an “Extended” exam (EFAST) and include views of the anterior thorax to evaluate for pneumothorax
- Persistent tachycardia after volume resuscitation, adequate pain control, and exclusion of intrathoracic or intraabdominal hemorrhage should raise suspicion of possible BCI
Testing and Treatment:
- Electrocardiogram
- 12-lead EKG is an important screening tool in the patient with potential BCI and can quickly guide the patient’s disposition
- New abnormalities on EKG such as
- Dysrhythmias (i.e. atrial fibrillation)
- Conduction delays (bundle branch blocks)
- ST segment elevations or depressions warrant continued telemetry monitoring
-
- The most common rhythm encountered after BCI is sinus tachycardia followed by atrial fibrillation
- EKGs should be repeated with any change in the patient’s symptomatology or hemodynamic status
EKG Findings in Blunt Cardiac Injury (Foil 1990 ):
- Chest X-ray
- Helpful initial test to evaluate thoracic trauma
- Certain injuries visible on x-ray are commonly associated with but do not guarantee BCI:
- Sternal fractures (Sadaba 2000 )
- Multiple rib fractures
- Echocardiography
- Part of a comprehensive evaluation for BCI
- Pericardial effusions and tamponade should be ruled out early with FAST exam
- Transthoracic Echocardiography (TTE)
- Can be performed at the bedside by EM physicians
- Provides an impression of:
- Overall cardiac contractility (organization, ejection fraction)
- Wall motion abnormalities
- Turbulent blood flow
- Intraventricular or intraatrial thrombi
- Visualization limited in up to 1/3 of patients due to poor echocardiographic views
- Transesophageal Echocardiography (TEE) is more sensitive in detecting injuries that require intervention (wall and valve ruptures)
- Time to surgery was significantly shorter for patients with BCI identified on TEE. (Chirillo 1996 )
- TTE should be repeated with any change in the patient’s status (Chirillo 1996 , Labovitz 2010 )
- Cardiac biomarkers
- Utility of cardiac biomarkers such as troponin remains unclear
- Presence of a single elevated troponin does little to help guide further management or intervention except for increasing the likelihood of admission and cardiology consultation
- Optimal timing for troponin measurement remains unknown
- A review of prospective studies demonstrated that a negative troponin had 100% negative predictive value for subsequent cardiac complications (Guild 2014 ). However, the ideal timing of checking that troponin is unknown
- Elevations in troponin can also be attributed to significant non-thoracic trauma
- CK-MB is not a recommended biomarker in BCI and has not been shown to correlate with morbidity or mortality from BCI (Fulda 1997 )
- There is no gold standard or recommendation for the routine use of cardiac biomarkers to characterize or prognosticate BCI
- Chest Computed Tomography (CT)
- CT with significant thoracic trauma raises the suspicion for BCI and should lead to further investigations
- CT is not sensitive as it has been shown to miss injuries then found on echo (Hammer 2016 )
Published Guidelines:
- The Eastern Association for the Surgery of Trauma (EAST) published a set of guidelines for the evaluation and care of those with BCI: (Clancy 2012 )
- Level 1 Evidence:
- Obtain an electrocardiogram (EKG) on all patients with suspected BCI
- Level 2 Evidence:
- If the EKG reveals a new abnormality (dysrhythmia, ST changes, heart blocks), admit the patient for continuous EKG (telemetry) monitoring. Compare to a previous EKG whenever available
- BCI can be ruled out in patients with a normal EKG and a negative troponin I although the optimal timing of troponin measurement remains undetermined
- Obtain an optimal TTE or a TEE on patients who are hemodynamically unstable or with persistent new arrhythmias
- Those with sternal fractures but also with a normal EKG and troponin I do not have to be continuously monitored
- Troponin I are the preferred cardiac enzymes. Creatinine phosphokinase levels are not useful
- Nuclear studies offer little when compared with Echocardiography and do not need to be obtained routinely
- Level 3 Evidence:
- Among patients with BCI, surgery is not contraindicated, given appropriate monitoring in
- The elderly with known cardiac disease
- Hemodynamically unstable patients
- Those with new EKG abnormalities on admission
- Measure troponin I on patients with suspected BCI. If elevated, admit to a monitored setting and follow serial troponins although the best timing of measurement has not been determined
- Cardiac CT or MRI can be useful in differentiating acute MI from BCI to help guide further management
Take Home Points
- No single test can be used to exclude BCI. However a thorough physical exam combined with a 12-lead EKG, troponin measurement, and echocardiography can be used to characterize BCI and direct care
- Obtain a 12-lead EKG in all thoracic trauma patients
- A chest x-ray may help to identify associated injuries. However, isolated musculoskeletal injuries such as sternal fractures do not correlate with a risk of BCI
- Bedside TTE can quickly evaluate for life-threats such as cardiac tamponade; A TEE is both sensitive and specific across the spectrum of BCI pathology and is part of a comprehensive evaluation
- BCI can be excluded in a patient without EKG abnormalities and a negative troponin I
Guest Post By:
Katrina D’Amore, MD
PGY-4 Resident
St. Joseph’s Regional Medical Center Emergency Department
References:
- Schultz JM, Trunkey DD: Blunt cardiac injury. Crit Care Clin 2004; 20(1): 57-70. PMID: 14979329
- Pasqu ale M, Fabian TC: Practice management guidelines for trauma from the Eastern Association for the Surgery of Trauma. J Trauma 1996; 44: 941; Discussion 956. PMID: 9637148
- Singh S, Angus LD: Blunt Cardiac Injury. NCBI Bookshelf StatPearls 2018. PMID: 30335300
- Emet M, et al: Assessment of cardiac injury in patients with blunt chest trauma. Eur J Trauma Emerg Surg 2010; 36 (5): 441-7. PMID: 26816225
- Shorr RM, et al: Blunt thoracic trauma. Analysis of 515 patients. Ann Surg 1987; 206: 200. PMID: 3606246
- Calhoon JH, et al: Management of blunt rupture of the heart. J Trauma 1986; 26: 495. PMID: 3723615
- Borjesson M, Pelliccia A: Incidence and aetiology of sudden cardiac death in young athletes: an international perspective. Br J Sports Med 2009; 43: 644. PMID: 19734497
- Rodriguez A, Turney SZ: Blunt injuries of the heart and pericardium, in Turney SZ, et al (eds) Management of Cardiothoracic Trauma. Baltimore MD, Williams & Wilkins, 1990.
- Tenzer ML: The spectrum of myocardial contusion: a review. J Trauma 1985; 25: 620. PMID: 2989545
- Yousef R, Carr JA: Blunt cardiac trauma: a review of the current knowledge and management. Ann Thoracic Surg 2014; 98 (3): 1134-40. PMID: 25069684
- Foil MB, et al: The asymptomatic patient with suspected myocardial contusion. Am J Surg 1990; 160: 638 discussion 642. PMID: 2252127
- Sadaba JR, et al: Management of isolated sternal fractures: determining the risk of blunt cardiac injury. Ann R Coll Surg Engl 2000; 82: 162-66. PMID: 10858676
- Clancy K, et al: Screening for blunt cardiac injury: An Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg 2012; 73(5) Supplement 4. PMID: 23114485
- Salim A, et al: Clinically significant blunt cardiac trauma: role of serum troponin levels combined with electrocardiographic findings. J Trauma 2001; 50: 237. PMID: 11242287
- Edouard AR, et al: Circulating cardiac troponin I in trauma patients without cardiac contusion. Intensive Care Med 1998; 24: 569. PMID: 9681778
- Guild CS, et al: Negative predictive value of cardiac troponin for predicting adverse cardiac events following blunt chest trauma. South Med J 2014; 107(1): 52-6. PMID: 24389788
- Reid CL, et al: Chest trauma: evaluation by two-dimensional echocardiography. Am Heart J 1987; 113: 971. PMID: 3565247
- Hiatt JR, et al: The value of echocardiography in blunt chest trauma. J Trauma 1988; 28(7): 914-22. PMID: 3398089
- Chirillo F, et al: Usefulness of transthoracic and transoesophageal echocardiography in recognition and management of cardiovascular injuries after blunt chest trauma. Heart. 1996;75(3):301. PMID: 8800997
- Karalis DG, et al: The role of Echocardiography in blunt chest trauma: a transthoracic and transesophageal echocardiographic study. J Trauma 1994; 36: 53. PMID: 8295249
- Labovitz AJ, et al: Focused cardiac ultrasound in the emergent setting: a consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. J Am Soc Echocardiogr 2010; 23 (12): 1225. PMID: 21111923
- Nagy KK, et al: Determining which patients require evaluation for blunt cardiac injury following blunt chest trauma. World J Surg 2001; 25(1): 108-11. PMID: 11213149
- Fulda GJ, et al: An evaluation of serum troponin T and signal-averaged electrocardiography in predicting electrocardiographic abnormalities after blunt chest trauma. The Journal of trauma: Injury, Infection, and Critical Care 1997; 43(2): 304-12. PMID: 9291377
- Hammer MM, et al: Imaging in blunt cardiac injury: Computed tomographic findings in cardiac contusion and associated injuries. Injury 2016; 47(5): 1025-30. PMID: 26646729
- Agarwal D, Chandra S: Challenges in the diagnosis of blunt cardiac injuries. Indian J Surg 2009; 71: 245-53. PMID: 23133167
- Bellal J, et al: Identifying the broken heart: predictors of mortality and morbidity in suspected blunt cardiac injury. Am J of Surg 2016; 211(6): 982-88. PMID: 26879418
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami) and Salim Rezaie, MD (Twitter: @srrezaie)
The post Blunt Cardiac Injury (BCI) appeared first on REBEL EM - Emergency Medicine Blog.