
5 MITOS SOBRE EL USO DE TORNIQUETES English/Español Control for the Injured Course "Stop The Bleed" / Control de Sangrados para el Herido
TORNIQUETE TQ DE EXTREMIDAD TIE (TOURNIQUET IN EMERGENCY). Antiguo Torniquete Compresor de Emergencias Ejercito Español "TORNIQUETE DE EXTREMIDAD ADRCE" . Video Estudio del torniquete de dotación del Ejército de Tierra Overview of the tourniquets used by the Army by Valentín González Alonso emssolutionsint.blogspot.com/2017/01/torniquete-compresor-de-emergencias.html
UnicGuias, Directrices y Protocolos validados cientificamente y endosados en base a medicina basada en evidencias al dia 11 Septiembre del 2018; STOP THE BLEED-Comite de Trauma Colegio Americano de Cirujanos y consenso de Hartford, CTECC, CoTCCC y DoD, TCC-LEFR Dr. Peter Pons, PHTLS, ATLS y los 8 ERRORES en el Control de Sangrados del Dr. Peter Pons, FACEP
Improvisación de un Torniquete TQ como último recurso ante hemorragia masiva de extremidades y sin recursos by CoTCCC.
https://youtu.be/0T0TO-DMTfI
Demostracion by #DrRamonReyesMD https://emssolutionsint.blogspot.com/2022/05/improvisacion-de-un-torniquete-tq-como.html #TQ #Tourniquet #Torniquete #TCCC #CoTCCC #Hemorragia #BleedingControl
Control de Sangrados España. STOPTHEBLEED BCon Basic by TACMED España
Tirador Activo: STOP THE BLEED "StopTheBleed" CONTROL DE SANGRADOS. Bleeding Control Basic. ESPAÑOL
8 trampas "ERRORES" a evitar en el control de hemorragia by Dr. Peter Pons, MD FACEP
Tactical Medics vs Rescue Task Force
| 5 MITOS SOBRE EL USO DE TORNIQUETES English/Español Control for the Injured Course "Stop The Bleed" / Control de Sangrados para el Herido |
{kind=link}
TORNIQUETE TQ DE EXTREMIDAD TIE (TOURNIQUET IN EMERGENCY). Antiguo Torniquete Compresor de Emergencias Ejercito Español "TORNIQUETE DE EXTREMIDAD ADRCE" . Video Estudio del torniquete de dotación del Ejército de Tierra Overview of the tourniquets used by the Army by Valentín González Alonso emssolutionsint.blogspot.com/2017/01/torniquete-compresor-de-emergencias.html
https://youtu.be/0T0TO-DMTfI
GUIA DE SOPORTE VITAL PARA SEGURIDAD PRIVADA COMO PRIMER INTERVINIENTE EN INCIDENTES ARMADOS. by Juan Jose Pajuelo Castro y David Grevillen Carretero. SEMES 2018
http://emssolutionsint.blogspot.com.es/2018/02/guia-de-soporte-vital-para-seguridad.html
PROTOCOLO PARA INTERVENCIONES DE SOPORTE VITAL EN INCIDENTES DE MÚLTIPLES VÍCTIMAS POR ATENTADOS TERRORISTAS ABRIL 2016 (Actualizado Marzo 2018) by Juan Jose Pajuelo
8 trampas a evitar en el controlhemorragias
Guia de Soporte en Incidentes con Amenaza para Primer Interviniente Policial by Juan Jose Pajuelo Castro emssolutionsint.blogspot.com/2018/07/guia-de-soporte-en-incidentes-con.html
TACTICAL COMBAT CASUALTY CARE Handbook version 5 May 2017 emssolutionsint.blogspot.com/2017/07/tactical-combat-casualty-care-handbook.html
Updated TCCC Guidelines (31 JAN 2017) "Actualizacion 2017 de las Guias" Tactical Combat Casualty Care emssolutionsint.blogspot.com/2012/07/presentacion-del-programa-phtls-tccc.html
TCCC TACTICAL COMBAT CASUALTY CARE Quick Reference Guide First Edition 2017 FREE PDF emssolutionsint.blogspot.com/2018/07/tccc-tactical-combat-casualty-care.html
Updated TCCC Guidelines (31 JAN 2017) "Actualizacion 2017 de las Guias" Tactical Combat Casualty Care emssolutionsint.blogspot.com.es/2012/07/presentacion-del-programa-phtls-tccc.html
MANUAL DE SOPORTE VITAL AVANZADO EN COMBATE Ministerio de Defensa España 2014 http://emssolutionsint.blogspot.com.es/2016/02/manual-de-soporte-vital-avanzado-en.html
COMTOMS TACTICAL MEDIC HANDBOOK 2013 Edition
Guías para el Manejo de Heridos en Incidentes Intencionados con Múltiples Víctimas y Tiradores Activo "MACTAC" emssolutionsint.blogspot.com/2016/12/guias-para-el-manejo-de-heridos-en.html
Manejo de Heridos en Incidentes Intencionados Múltiples Víctimas y Tiradores Activos 09/07/2017 emssolutionsint.blogspot.com/2018/07/manejo-de-heridos-en-incidentes.html
TERRORISMO Y SALUD PÚBLICA - "GESTIÓN SANITARIA DE ATENTADOS TERRORISTAS POR BOMBA" emssolutionsint.blogspot.com/2013/08/terrorismo-y-salud-publica-gestion.html
TRAUMA DE TORAX: DOCENA DE LA MUERTE en trauma toracico
https://emssolutionsint.blogspot.com.es/2013/01/penetrating-chest-trauma-photo-trauma.html
75th Ranger Regiment Trauma Management Team (Tactical) Ranger Medic Handbook FREE pdf emssolutionsint.blogspot.com.es/2018/02/75th-ranger-regiment-trauma-management.html
SPECIAL OPERATIONS FORCES Medical Handbook Free PDF emssolutionsint.blogspot.com/2018/02/special-operations-forces-medical.html
Balística de las heridas: introducción para los profesionales de la salud, del derecho, de las ciencias forenses, de las fuerzas armadas y de las fuerzas encargadas de hacer cumplir la ley http://emssolutionsint.blogspo
Guía para el manejo médico-quirúrgico de heridos en situación de conflicto armado by CICR http://emssolutionsint.blogspo
CIRUGÍA DE GUERRA TRABAJAR CON RECURSOS LIMITADOS EN CONFLICTOS ARMADOS Y OTRAS SITUACIONES DE VIOLENCIA VOLUMEN 1 C. Giannou M. Baldan CICR http://emssolutionsint.blogspo
Manual Suturas, Ligaduras, Nudos y Drenajes. Hospital Donostia, Pais Vasco. España http://emssolutionsint.blogspo
Manual de suturas. Menarini http://emssolutionsint.blogspo Técnicas de Suturas para Enfermería ASEPEYO y 7 tipos de suturas que tienen que conocer estudiantes de medicina http://emssolutionsint.blogspo
Manual Práctico de Cirugía Menor. Grupo de Cirugia Menor y Dermatologia. Societat Valenciana de Medicina Familiar i Comunitaria http://emssolutionsint.blogspo
Protocolo de Atencion para Cirugia. Ministerio de Salud Publica Rep. Dominicana. Marzo 2016 http://emssolutionsint.blogspo
Manual de esterilización para centros de salud. Organización Panamericana de la Salud http://emssolutionsint.blogspo
Asistencia de salud en peligro: la importancia de proteger al personal de salud en zonas de guerra PDF Gratis http://
SERVICIOS PREHOSPITALARIOS Y DE AMBULANCIAS EN SITUACIONES DE RIESGO. PDF GRATIS http://
PDF Update on Prehospital Trauma Courses, NAEMT, Alex Eastman, Lieutenant and Deputy Medical Director, City of Dallas http:// emssolutionsint.blogspot.co m.es/2016/12/ phtls-prehospital-trauma-li
Tactical Emergency Casualty Care (TECC) Guidelines for First Responders with a Duty to Act Guías para Primeros Respondedores con Deber de Actuar “En Acto de Servicio” (Fuerzas de Seguridad, Bomberos no SEM) emssolutionsint.blogspot.com/2018/07/tactical-emergency-casualty-care-tecc.html
PAGINA FCEBOOK
TACMED Spain Medicina Tactica España GRUPO https://www.facebook.com/groups/311284402300505/
TERRORISMO Y SALUD PÚBLICA - "GESTIÓN SANITARIA DE ATENTADOS TERRORISTAS POR BOMBA" emssolutionsint.blogspot.com/2013/08/terrorismo-y-salud-publica-gestion.html
TRAUMA DE TORAX: DOCENA DE LA MUERTE en trauma toracico
https://emssolutionsint.blogspot.com.es/2013/01/penetrating-chest-trauma-photo-trauma.html
75th Ranger Regiment Trauma Management Team (Tactical) Ranger Medic Handbook FREE pdf emssolutionsint.blogspot.com.es/2018/02/75th-ranger-regiment-trauma-management.html
SERVICIOS PREHOSPITALARIOS Y DE AMBULANCIAS EN SITUACIONES DE RIESGO. PDF GRATIS http://
PDF Update on Prehospital Trauma Courses, NAEMT, Alex Eastman, Lieutenant and Deputy Medical Director, City of Dallas http:// emssolutionsint.blogspot.co m.es/2016/12/ phtls-prehospital-trauma-li
Stop The Bleed Campaign - App Now Available
Th e Uniformed Services University/National Center for Disaster Medicine and Public Health Stop the Bleed app is now available. The app contains a 5-minute video, Q&A, a quiz, and other resources. Download the free app from Google and Apple iTunes .
Ahi dejamos para los que se estan tomando el cafe de media mañana y para los que inician el dia del otro lado del charco,,, el #ChamanTacticoMD https://www.youtube.com/watch?v=R4UBk6mtwzI&feature=youtu.be ver detenidamente,,, datos importantes...
TORNIQUETE DE EXTREMIDAD TIE (TOURNIQUET IN EMERGENCY). Antiguo Torniquete Compresor de Emergencias Ejercito Español "TORNIQUETE DE EXTREMIDAD ADRCE" . Video Estudio del torniquete de dotación del Ejército de Tierra Overview of the tourniquets used by the Army by Valentín González Alonso
Informacion en el enlace http:// emssolutionsint.blogspot.co m.es/2017/01/ torniquete-compresor-de-eme
¿Cómo sobrevivir a un tiroteo en la escuela u oficina? Preparación Contra Tiradores Activos. PREVENCIÓN ATAQUES CON VEHÍCULOS Video http://emssolutionsint.blogspot.ae/2016/06/como-sobrevivir-un-tiroteo-en-la.html
"StopTheBleed". Tirador Activo: STOP THE BLEED "StopTheBleed" CONTROL DE SANGRADOS. Bleeding Control Basic. ESPAÑOL
Control de Sangrados España. STOPTHEBLEED BCon Basic by TACMED España
{kind=link}
| TORNIQUETE DE EXTREMIDAD TIE (TOURNIQUET IN EMERGENCY). Antiguo Torniquete Compresor de Emergencias Ejercito Español "TORNIQUETE DE EXTREMIDAD ADRCE" . Video Estudio del torniquete de dotación del Ejército de Tierra Overview of the tourniquets used by the Army by Valentín González Alonso Informacion en el enlace http:// emssolutionsint.blogspot.co m.es/2017/01/ torniquete-compresor-de-eme |
{kind=link}
{kind=link}
{kind=link}
https://t.me/joinchat/FpTSAEHYjNLkNbq9204IzA
{kind=link}
{kind=link}
{kind=link}
El instructor Félix Carmona pone el dedo en la llaga y nos habla de una costumbre que nuestras FCS y FCSE deben adoptar: el material sanitario policial.
GUIA DE SOPORTE VITAL EN INCIDENTES CON AMENAZA ELEVADA PARA PRIMER INTERVINIENTE POLICIAL by Juan Jose Pajuelo. España 2017 Descargate la guia: Guía para Primer Interviniente Policial El objetivo de estas Guías no es otro que resumir de manera breve y concisa los pasos ideales (en ocasiones lo ideal no es lo real) para una valoración y manejo iniciales de las principales causa de muerte evitable, hasta la llegada de los Servicios de Emergencia, en los compañeros o ciudadanos heridos. Se pretende que estas Guías aborden la asistencia inicial, en el contexto de una intervención o incidente donde exista un alto nivel de amenaza, en el que se vean involucrados los “policías de a pie”, puesto que ha quedado demostrado que son los primeros (y en ocasiones los únicos) en abordar inicialmente tanto al incidente en sí mismo, como a las víctimas si se han producido. Un incidente con alto nivel de amenaza no se limita a sucesos como atentados terroristas con múltiples víctimas, si no que contempla también otro tipo de circunstancias como incidentes con individuos armados y/o, aglomeraciones populares con individuos violentos. Toman como referencia las Directrices para Primeros Intervinientes con la Obligación de Asistir (First Responders with a Duty to Act) del Comité del Tactical Emergency Casualty Care que, al igual que estas Guías, son meras recomendaciones y no protocolos rígidos que deben adaptarse a la legislación vigente y, a las especificidades de cada Institución/Servicio/Organismo. Con independencia de lo mencionado anteriormente, tienen como objetivo final estandarizar un lenguaje y unas actuaciones a nivel nacional dado que, están basadas en la evidencia científica “in vivo” y, en las lecciones aprendidas de muchos profesionales nacionales e internacionales. Estas recomendaciones/guías, no sustituirán el buen juicio clínico. Por lo tanto, se espera que las recomendaciones que se presentan a continuación sirvan de ayuda para todo aquél personal policial que se pueda ver involucrado en un incidente con un nivel de amenaza elevado, a la hora de enfrentarse al manejo de las principales causas de muerte evitable que se producen en actuaciones con un alto nivel de amenaza. |
{kind=link}
{kind=link}
Viendo lo que está sucediendo en estos países más avanzados, podemos hacernos una idea de lo que nos podremos encontrar en Europa en unos años. Por eso, no es raro ver en el cinturón de un agente de policía americano, un torniquete o un kit de primeros auxilios, para heridas de armas de fuego, en el chaleco antibalas interior.
1) TORNIQUETES
Se recomienda aplicarlo en la parte superior de las extremidades, ya que existe un solo hueso y la artería deja de sangrar haciendo presión contra él. Se puede cortar una 80% de hemorragia apretando fuertemente el torniquete y el resto con la barra de presión.
{kind=link}
El torniquete CAT está hecho de materiales ligeros y resistentes, lo que permite contener la hemorragia de la extremidad dañada sin problemas. Según tengo entendido, la marca que lo fabrica asegura sólo un uso del mismo. Además, éste es del que más copias chinas hay extendido. Si un torniquete no te cuesta más de 25 o 28 euros en adelante, no te fíes. Ten cuidado con las copias baratas. Te puede costar la vida.- El torniquete SOFT se encuentra realizado según los consejos de las Fuerzas de Operaciones Especiales Norteamericanas, las cuales querían un torniquete robusto y reutilizable. Por ello, la barra que posee para girar y apretar la cinta de contención de la hemorragia es de aluminio, por lo que el conjunto en sí pesa algo más que el torniquete CAT. Además, es mucho más fácil de colocar a otra persona, gracias a su clip de apertura. Aunque sea reutilizable, sería conveniente no darle más de un uso, por si acaso.
2) GASA DE COMBATE
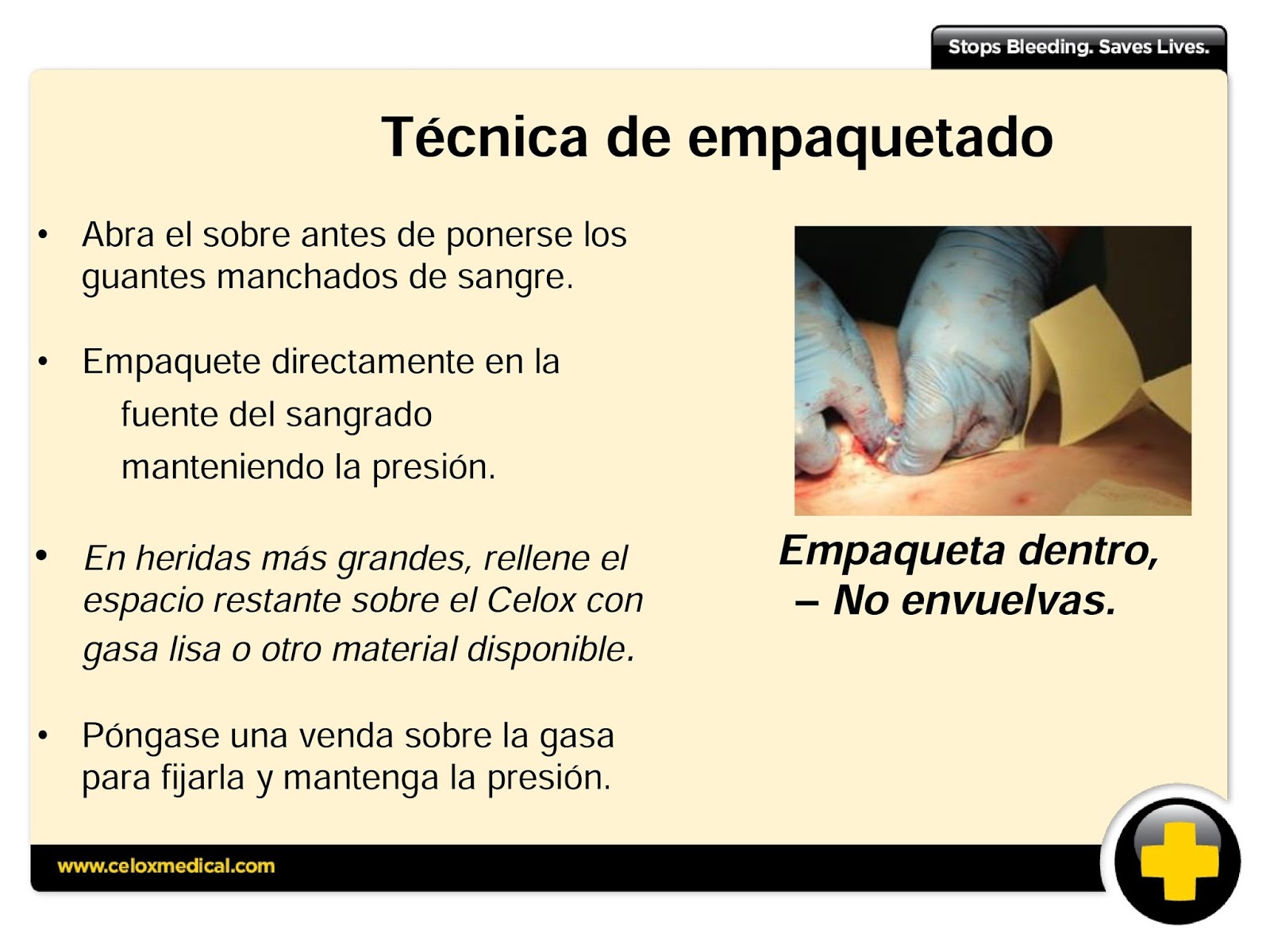
Si la herida no sangra abundantemente, se puede usar en vez del torniquete. Lo malo es que es muy “invasiva” (hay que meterla con los dedos en el interior de la herida) y eso debe ser muy doloroso, aunque si la vida está en juego, es un mal menor.
El mejor uso que se le puede dar es en las heridas de unión de partes del cuerpo (axilas, ingles y cuello), ya que en esos sitios no se puede colocar un torniquete. A la hora de introducir el vendaje en la herida, se debe hacer de dentro hacia fuera y, conforme vamos subiendo, de derecha a izquierda. Así no nos dejaremos ningún hueco sin tapar. Luego, cuando ya tengamos la herida “empaquetada”, la presionaremos (más o menos durante 5 minutos) para contener la hemorragia.
Por supuesto, hay mucho material de este tipo de otras marcas, como puede ser el ChitoGauze o el Celox Rapid Gauze, que realizan la misma función.
3) CELOX
La forma de usarlo es echar los gránulos en la herida abierta y presionar con una gasa durante unos minutos. Así pararemos la hemorragia. Se sirve en paquetes de 15 y 35 gramos, siendo el paquete más grande la mejor relación calidad-precio.
Lo malo de este granulado es que, cuando hay mucho viento, no se puede aplicar correctamente. Para ello existe otro producto de la misma marca que permite verter el contenido en el interior de la herida. Se llama “Celox A”.
Es como una especie de jeringuilla llena de este gránulo, pero hay que meterlo en el interior de la herida, con lo que debe doler una barbaridad, pero en esos momentos, ya se sabe.
4) PARCHE TORÁCICO
- El básico solamente es un adhesivo que se pone sobre la herida. Con éste hay que vigilar al herido por si se agobia y hay que despegárselo un poco durante unos segundos, volviéndoselo a poner bien, rápidamente.
- Hay otros modelos que tienen una especie de canales o válvulas que permiten la salida del aire durante la exhalación, pero impide su entrada en la inspiración. Se suelen vender en pack de 2 parches, pero también existen paquetes individuales. El pack de 2 parches está bien, por si existe orificio de entrada y salida.
5) VENDAJES
6) HERRAMIENTA MULTIUSO
Algunos de estos cortadores llevan su propia funda que se puede acoplar al cinturón de servicio, lo cual es una ventaja, ya que siempre lo llevaremos encima. Existen de varios tipos y tamaños, por lo que nos da un abanico amplio para su elección. Muchos de ellos incorporan una punta, en el extremo opuesto, que permite romper cristales de vehículos. La marca Gerber parece ser la que mejor precio tiene.
Conclusión
Es importante recibir formación y si no la recibes, búscala por tu cuenta. Puede que algún día lo agradezcas.
Resultados:
Comentarios
Dispositivos adecuados
(2) http://www.ncbi.nlm.nih.gov/pubmed/19106667
| STOP THE BLEED Presentacion para Descarga. B-Con es GRATIS y se ha diseñado para que profesionales sanitarios puedan convertirse en multiplicadores, para asi reducir las muertes prevenibles por sangrados producidos por heridas exanguinantes, fue deseo del Dr. Norman McSwain que estos conocimientos quedaran libres, bajo la custudia cientifica del Colegio Americano de Cirujanos y ha sido desarrollado el contenido por el Dr. Peter Pons bajo los Protocolos y Sistemas de Educacion del PHTLS-NAEMT. http:// Compartimos gratuitamente http:// JORNADAS GRATUITAS DE REDUCCION DE MUERTES POR SANGRADO EN TRAUMA CURSOS B-CON BLEEDING CONTROL FOR THE INJURED http:// emssolutionsint.blogspot.co m.es/2017/01/ propuesta-jornada-de-reducc http:// emssolutionsint.blogspot.co m.es/2016/07/ the-hartford-consensus-iv-c #BCon #PHTLS #EMS #STOPTHEBLEED#TRAUMA Mision Medico Encargado de TACEVAC para la Union Europea Torniquetes la controversia En la foto el Dr. Ramon Reyes Diaz y el Mayor Medico Cirujano Toracico y Cardiovascular Георги Кесов del Ejercito Bulgaro, Director Medico de las Fuerzas Especiales Bulgaras. Mali-Africa Mayo 2016. @drramonreyesdiaz Guías para el Manejo de Heridos en Incidentes Intencionados con Múltiples Víctimas y Tiradores Activo Bleeding Control by American College of Surgeons and The Hartford Consensus IV #STOPTHEBLEED #EMS #TCCC #PHTLS #ESPAÑA #EJERCITOESPAÑOL #TORNIQUETE #CAT #STAT #RAT #BCON #NAEMT #NATO #OTAN The American College of Surgeons has a number of resources available on their BleedingControl.org website to help the public learn more about bleeding control and how to act in a situation that requires immediate responders. Stop the Bleed Resources Visit BleedingControl.org for: The Hartford Consensus IV: A Call for Increased National Resilience |
American College of Surgeons Releases Hartford Consensus Compendium Wed, Sep 16, 2015 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Blood gushes from virtual leg injury to help train combat medics
Immediately following the active shooter disaster at the Sandy Hook Elementary School in Newtown, CT, Dr. Norman McSwain agreed to be a founding member of the Joint Committee to Develop a National Policy to Increase Survival from Active Shooter and Intentional Mass Casualty Events. Dr. McSwain brought the dedication, passion, and intellect for which he was famous to the Hartford Consensus deliberations.
He fiercely advocated for an organized coordinated prehospital response that incorporated hemorrhage control by immediate bystander responders, a change in focus of the mission of law enforcement to include immediate stopping of life-threatening hemorrhage of victims, and an urgent response by emergency medical personnel to treat and transport trauma patients to the appropriate trauma hospitals. He recognized that time was a critical factor for patients who had massive bleeding.
Through this work, his commitment to excellent prehospital care has been given to millions of trauma patients worldwide. Throughout his career Dr. McSwain was been honored by the American College of Surgeons Committee on Trauma and numerous other professional organizations. However, it was his personal commitment to excellent individual care of the patient, his personal example of the compassionate trauma surgeon, and his kind, caring desire to help people from all walks of life that will always be remembered.
He was a good friend, an excellent person, and an example for all of us that will be forever captured by his greeting to everyone: “What have you done for the good of mankind today?” May he rest in peace.
{kind=link}
| One-handed tourniquet application and immediate responder hemorrhage control PHTLS B-Con Bleeding Control for the Injured Course Hartford Consensus III |
{kind=link}
312-202-5328
or
Sally Garneski
312-202-5409
pressinquiry@facs.org
{kind=link}
The Hartford Consensus III: Implementation of Bleeding Control
PUBLISHED JULY 1, 2015
Professional first responders
Building educational capabilities
Roundtable on bystanders: Our nation’s immediate responders
- Air Medical Physician Association
- American Academy of Physician Assistants
- American Ambulance Association
- American Association of Critical Care Nurses
- American Association for the Surgery of Trauma
- American College of Emergency Physicians
- American College of Surgeons
- American Heart Association
- American Hospital Association
- American Nurses Association
- American Osteopathic Association
- American Physical Therapy Association
- American Public Health Association
- American Trauma Society
- Association of Air Medical Services
- Association of State and Territorial Health Officials
- Eastern Association for the Surgery of Trauma
- Emergency Nurses Association
- Emergency Medical Services Labor Alliance
- International Academies of Emergency Dispatch
- International Association of Chiefs of Police
- International Association of Emergency Managers
- International Association of Emergency Medical Services Chiefs
- International Association of Firefighters
- International Association of Fire Chiefs
- Major Cities Chiefs Association
- National Association of Emergency Medical Technicians
- National Association of School Nurses
- National Association of State EMS Officials
- National Athletic Trainers Association
- National Emergency Management Association
- National Volunteer Fire Council
- Society of Emergency Medicine Physician Assistants
- Society of Trauma Nurses
- Trauma Center Association of America
- White House personnel
- Interagency Bystander Workgroup team leaders
- Federal invitees
The Hartford Consensus III: Implementation of Bleeding Control
Joint Committee to Create a National Policy to Enhance Survivability from Intentional Mass-Casualty and Active Shooter Events
Chairman, Hartford Consensus
Vice-President, Academic Affairs
Hartford Hospital
Board of Regents,
American College of Surgeons
17th U.S. Surgeon General
Medical Director, Prehospital Trauma Life Support
Tulane University
Chairman, Committee on Tactical Combat Casualty Care
Department of Defense Joint Trauma Systems
President, The Hartford
Chair, Board of Directors
Hartford Hospital
President, American College of Surgeons
Massachusetts General Hospital, Boston
Assistant Secretary of Defense for Health Affairs, Department of Defense
Director for Medical Preparedness Policy,
National Security Council Staff
The White House
Administrator, U.S. Fire Administration
Federal Emergency Management Agency
Department of Homeland Security
Major Cities Police Chiefs Association
Chief of Trauma, Parkland Memorial Hospital
University of Texas Southwestern Medical Center
Assistant Secretary, Health Affairs
Chief Medical Officer,
Department of Homeland Security
Physician to the Vice-President
The White House
Director, Emergency Medical Services
Federal Bureau of Investigation
Distinguished Visiting Fellow,
Harvard University, School of Public Health
8th Deputy Administrator,
Federal Emergency Management Agency
Chief Emeritus, Emergency Medicine
Massachusetts General Hospital
Research Scientist, Hartford Hospital
Johns Hopkins University
Senior Medical Officer,
Johns Hopkins Center for Law Enforcement Medicine
Vice-Chair, Committee on Trauma
American College of Surgeons
Eastern Virginia Medical School
Chief, Division of Acute Care Surgery
University of Texas Health Science Center
Department of Surgery
University of Arizona
Chair, Committee on Trauma
American College of Surgeons
The University of Texas Health Science Center at San Antonio
Military Assistant to the Assistant Secretary of Defense for Health Affairs
Department of Defense
Physician-in-Chief,
R Adams Cowley Shock Trauma Center
University of Maryland School of Medicine
Medical Director, Trauma Center
Mayo Clinic
Trauma, Emergency Surgery and Surgical Critical Care
Department of Surgery
Massachusetts General Hospital
The Bleeding Control for the Injured (B-Con) course was developed by NAEMT's PHTLS Committee with leadership provided by Dr. Peter Pons and Dr. Norman McSwain.
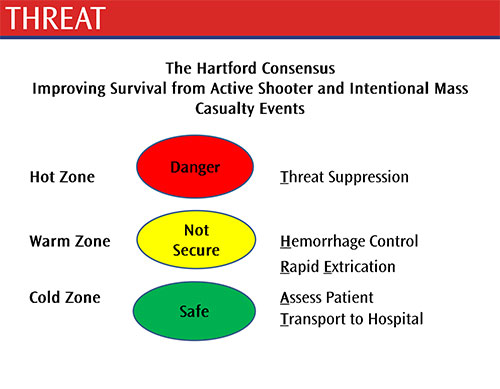
The course was developed in response to efforts by the U.S. Departments of Homeland Security and Health and Human Services to increase collaboration between law enforcement, the fire service and EMS in responding to active shooter/IED/mass casualty events. B-Con is consistent with the recommendations of the Hartford Consensus on Improving Survival from Active Shooter Events. The Hartford Consensus recommends that an integrated active shooter response should include the critical actions contained in the acronym THREAT: 1.Threat
2.Hemorrhage control
3.Rapid Extrication to safety
4.Assessment by medical providers
5.Transport to definitive care
The Hartford Consensus Group recommends that the response to a traumatic incident, whether involving an active shooter or some other cause of injury, in fact begins with bystander response. It is with this in mind that the B-Con course was developed and is now being offered.
This new 2 ½ hour course teaches participants the basic life-saving medical interventions, including bleeding control with a tourniquet, bleeding control with gauze packs or topical hemostatic agents, and opening an airway to allow a casualty to breathe. The course is designed for NON tactical law enforcement officers, firefighters, security personnel, teachers and other civilians requiring this basic training. Course materials include a PowerPoint presentation and instructor notes, instructor’s guide, and skill station guide.
A separate, additional PowerPoint module is included in the course materials specifically for law enforcement participants. This module provides an orientation to the content of the Hartford Consensus and the changing approach to active shooter and other complex and hazardous responses.
At the completion of the course, participants will be able to:
•Explain the rationale for early use of a tourniquet for life-threatening extremity bleeding.
•Demonstrate the appropriate application of a tourniquet to the arm and leg.
•Describe the progressive strategy for controlling hemorrhage.
•Describe appropriate airway control techniques and devices. •Demonstrate the correct application of a topical hemostatic dressing (combat gauze).
{kind=link}
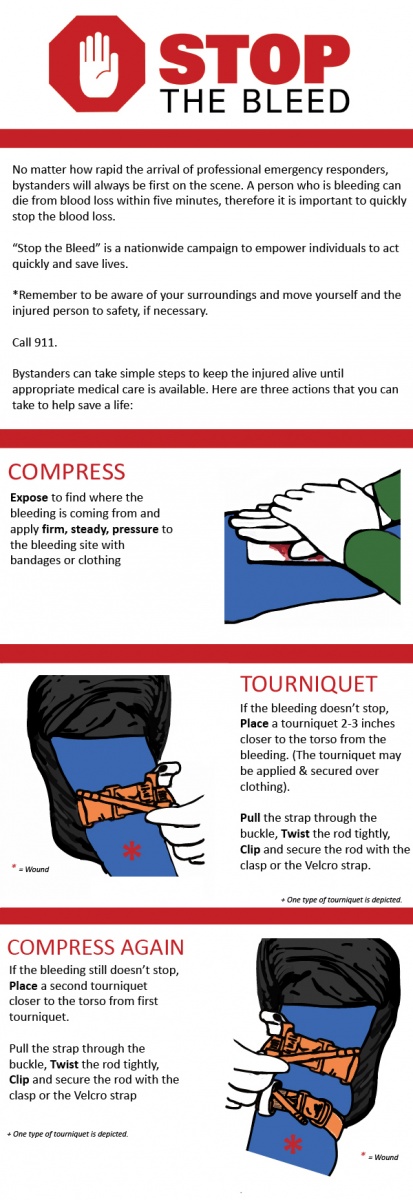
Compress
Tourniquet
Compress Again
More Information
- Download the steps above as a shareable infographic (229 KB JPG)
- Download a high resolution copy of the "Stop the Bleed" logo (152 KB JPG)
- Army Combat Casualty Care Research Program
{kind=link}
{kind=link}
{kind=link}
Control de Sangrados para el Herido By NAEMT.
5 MITOS SOBRE LOS TORNIQUETES
- Los torniquetes se deben utilizar solamente como último recurso.
- 232 pacientes
- 428 torniquetes aplicados
- El torniquete CAT fue aplicado un 79% de las veces
- No se apreciaron lesiones causadas por su aplicación (necrosis, fallo renal, amputaciones, necesidad de fasciotomia)
- No se realizó una sola amputación debido al uso del torniquete
- Eliminar la amenaza (Threat supression)
- Control de la hemorragia (Hemorrhage control)
- Extracción rápida a un lugar seguro (Rapid Extrication to safety)
- Evaluación por personal sanitario (Assessment by medical providers)
- Traslado para el tratamiento definitivo (Transport to definitive care)
- La colocación de un torniquete es igual a la pérdida de la extremidad.
- Los cinturones son el mejor torniquete.
- Los torniquetes improvisados constituyen equipación médica adecuada.
- Este es el mejor torniquete.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PHTLS B-Con Bleeding Control for the Injured Course / Control de Sangrados para el Herido By NAEMT |
Mejorando la supervivencia en Incidentes con Tiradores Activos (B-Con Course) Curso Control de Sangrados en el Herido
(Active Shooter Events): El Consenso Hartford
Comité Conjunto para Crear una Política Nacional para Mejorar la Supervivencia en
Incidentes De Múltiples Víctimas en Tiroteos
Hartford, CT 2 de Abril de 2013
Dr. Lenworth Jacobs, Hartford Hospital, Board of Regents, American College of Surgeons
Dr. Norman McSwain, Medical Director, Prehospital Trauma Life Support
Dr. Michael Rotondo, Chair, American College of Surgeons Committee on Trauma
Dr. David Wade, Chief Medical Officer, FBI
Dr. William Fabbri, Medical Director, Emergency Medical Support Program, FBI
Dr. Alexander Eastman, Major Cities Chiefs Association (Lt. Dallas Police Department)
Dr. Frank Butler, Chairman, Committee on Tactical Combat Casualty Care
John Sinclair, International Director and Immediate Past Chair International Association of Fire Chiefs- EMS Section (Fire Chief, Kittitas Valley Fire and Rescue)
Introducción
Los recientes sucesos de múltiples víctimas en tiroteos ocurridos en América han tenido un
profundo efecto en todos los sectores de la sociedad. Las comunidades médicas, de las
Fuerzas de Seguridad, de rescate/bomberos y de los SEM han sentido la necesidad de dar
respuestas. Es importante que estos esfuerzos se realicen de manera coordinada para crear
políticas que puedan mejorar la supervivencia de las víctimas producidas en estos
incidentes. Tales políticas deben proporcionar una aproximación sincronizada entre las
múltiples agencias que se encuentre inmediatamente disponible para las comunidades
afectadas por dichas tragedias.
El Colegio Americano de Cirujanos y el Federal Bureau of Investigation (FBI) han
colaborado conjuntamente para proporcionar altos representantes de todas las disciplinas
anteriormente mencionadas, para elaborar un documento que estimule el debate y en última
instancia conduzca a estrategias para mejorar la supervivencia de las víctimas. La
conferencia de un día de duración, el 2 de Abril de 2013 en Hartford, Connecticut, recibió
contribuciones de expertos médicos, de las Fuerzas de Seguridad, de
bomberos/rescatadores, de primeros intervinientes del SEM y de militares. La conferencia
consistió en actualizaciones de datos y evidencias extraídos de experiencias civiles y
militares recientes y, fue sensible al papel desempeñado por múltiples agencias que
participaron en incidentes de múltiples víctimas por tiroteo. La reunión, conocida como
Conferencia del Consenso Hartford (Hartford Consensus Conference), generó un
documento conceptual titulado “Mejora de la Supervivencia en Incidentes de Tiradores
Activos” (“Improving Survival from Active Shooter Events.”) El propósito de este
documento es promover las políticas locales, estatales y nacionales para mejorar la
supervivencia en estas situaciones poco comunes, pero terroríficas. Este ensayo corto
describe métodos para minimizar la pérdida de vidas humanas en estos terribles incidentes.
Planteamiento del Problema
Los incidentes de tiradores activos/múltiples víctimas son una realidad en la vida actual
americana. A medida que nuestra experiencia en este tipo de eventos se va acumulando, va
quedando claro que las respuestas tradicionales por parte de las Fuerzas de Seguridad,
bomberos/rescatadores y SEM no están adecuadamente alineadas para maximizar la
supervivencia de las víctimas.
Control Precoz de la Hemorragia para Mejorar la Supervivencia
Históricamente, la respuesta a los tiroteos ha consistido en una operación segmentada y
secuencial de seguridad pública, con la priorización de la seguridad como uno de los
objetivos de las Fuerzas de Seguridad (detener el tiroteo), seguido por el resto de medidas
de respuesta y recuperación. A medida que evolucionamos, las acciones iniciales para el
control de la hemorragia deben formar parte de la respuesta de las Fuerzas de Seguridad y,
los conocimientos para el control de la hemorragia, tienen que ser una parte central de sus
habilidades. Maximizar la supervivencia implica un sistema actualizado e integrado que
pueda alcanzar múltiples objetivos de forma simultánea.
Las lesiones de riesgo vital en incidentes con tiradores activos, como los producidos en Fort
Hood, Tucson y en Aurora, son similares a las que nos podemos encontrar en combate. La
experiencia militar nos ha enseñado que la causa principal de muerte evitable en una
víctima con trauma penetrante es la hemorragia. Los programas Tactical Combat Casualty
Care (TCCC), cuando son implementados con un apoyo sólido de los jefes, han producido
una reducción drástica de las muertes evitables. Reconociendo que los incidentes con
tiradores activos pueden ocurrir en cualquier comunidad, el Consenso Hartford anima al uso
de las técnicas y equipos existentes, validados por más de una década de evidencia clínica
bien documentada.
El Consenso Hartford recomienda que una respuesta integrada para tirador activo debe
incluir las acciones críticas contenidas en el acrónimo THREAT:
1. Eliminar la amenaza (Threat suppression)
2. Control del la Hemorragia (Hemorrhage control)
3. Extracción Rápida a zona segura (Rapid Extrication to safety)
4. Evaluación por personal sanitario (Assessment by medical providers)
5. Traslado para el tratamiento definitivo (Transport to definitive care)
Mientras que algunos pueden considerar añadir habilidades para el control de la hemorragia
como otro requisito en la formación en tiempos de recursos económicos limitados, los
conceptos son simples, probados y relativamente económicos; ya han sido adoptadas como
la mejor práctica por muchas agencias de las fuerzas de seguridad. La mejor forma de
controlar la hemorragia exanguinante por lesiones en extremidades se consigue mediante el
uso de torniquetes, mientras que la mejor forma de controlar la hemorragia interna
producida por heridas penetrantes en el tórax y el tronco se consigue mediante el traslado
rápido al hospital. Una respuesta óptima a un suceso con tirador activo incluye la
identificación y la enseñanza de conjuntos de habilidades apropiados a cada nivel de
respuesta, sin tener en cuenta la afiliación de las Fuerzas de Seguridad o de los
bomberos/rescatadores/SEM. El algoritmo THREAT incorpora los conceptos probados de
autoayuda y de ayuda por el compañero (self-care and buddy-care).
Respuesta Integrada
La asistencia a las víctimas es una responsabilidad compartida por las Fuerzas de
Seguridad, bomberos/rescatadores, y SEM. Los resultados óptimos dependen de la
comunicación entre el personal de seguridad pública. La respuesta a un incidente con
tirador activo es un proceso que requiere la coordinación entre las Fuerzas de Seguridad y el
personal sanitario/de evacuación. Dicha coordinación incluye:
Definiciones compartidas de términos empleados en incidentes con heridos en tiroteos.
Desarrollo conjunto de protocolos locales para la respuesta a incidentes con tiradores activos.
Prioridad de la inclusión de incidentes con tiradores activos en el entrenamiento y simulacros para mejorar la familiarización con los protocolos conjuntos desarrollados.
Conclusión
El Consenso Hartford busca mejorar la supervivencia en los incidentes con tiradores activos. El uso del algoritmo THREAT y una mejor respuesta integrada por parte de las Fuerzas de Seguridad, bombeos/rescatadores y SEM, ofrecen a las comunidades un mecanismo para minimizar la pérdida de vidas humanas en estos incidentes.
La Asociación Nacional de Técnicos de Emergencias Médicas (NAEMT) anunció la publicación de un curso para enseñar al personal civil las mismas técnicas de control de sangrados aprendidas en Iraq y Afganistán que han demostrado aumentar la supervivencia a lesiones mortalmente peligrosas. El curso “Bleeding Control for the Injured”, o mejor conocido como B-Con, está basado en la evidencia más actualizada de cómo atender una persona severamente herida.
| PHTLS Medical Director Attends Hartford Consensus III Dr. Norman McSwain (front left), medical director of the Prehospital Trauma Life Support (PHTLS) Committee and professor of Surgery at Tulane University, attended the third meeting of the Hartford Consensus group last month in Hartford, Conn. Participants from public safety and the medical community developed strategies to increase survivability in mass casualty shootings. This third meeting builds on documents known as th e Hartford Consensus I and II, which outline the needed response to active shooters as THREAT (Threat suppression; Hemorrhage control; Rapid Extrication to safety; Assessment by medical providers; and Transport to definitive care). Learn more about the Hartford Consensushttp://goo.gl/omWXQb Curso PHTLS Bcon Bleeding Control for the Injured Course / Control de Sangrados para el Herido By NAEMT |
.jpg){kind=link}
What is “Stop the Bleed”?
“Stop the Bleed” at Orlando Health
IPSA InfoBrief: Stop the Bleed
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PHTLS B-Con Bleeding Control for the Injured Course
| 5 MITOS SOBRE EL USO DE TORNIQUETES English/Español Control for the Injured Course "Stop The Bleed" / Control de Sangrados para el Herido |
MAS LIBROS MEDICINA Y SALUD
Les Esperamos en nuestro Grupo en TELEGRAM Soc. IberoAmericana de Emergencias
Todos Nuestros VIDEOS en YouTube
| 5 MITOS SOBRE EL USO DE TORNIQUETES English/ Español Control for the Injured Course "Stop The Bleed" / Control de Sangrados para el Herido |
{kind=link}
{kind=link}
MANUAL DE ATENCIÓN AL PARTO EN EL ÁMBITO EXTRAHOSPITALARIO. Ministerio de Sanidad, Servicios Sociales e Igualdad. España
¿Qué es el parto velado "Parto Empelicado" o nacer con bolsa intacta? by NATALBEN.com
{kind=link}
Hemos estado entrenando al personal de escolta del Ministro de Defensa de Republica Dominicana y en las practicas del uso del torniquetes hemos utilizado el CAT, SAM XT, SICH, TIE, DINPRO, los Mejores valorados por instructores y más de 48 Estudiantes;
1. DINPRO ganador Ucrania https://emssolutionsint.blogspot.com/2022/12/torniquete-dinpro-hecho-en-ucrania.html
2. SICH Ucrania https://emssolutionsint.blogspot.com/2023/05/torniquete-strengthened-individual.html
3. TIE España https://emssolutionsint.blogspot.com/2017/01/torniquete-compresor-de-emergencias.html
Mayo 23-25 del 2023
Ministerio de Defensa de la Republica Dominicana
Advertencia: El Dr. Ramon Reyes, MD no tiene compromisos personales, ni comerciales con ninguna de las marcas anteriormente mencionada
Contactos con el Dr. Ramon Reyes, MD https://emssolutionsint.blogspot.com/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html