
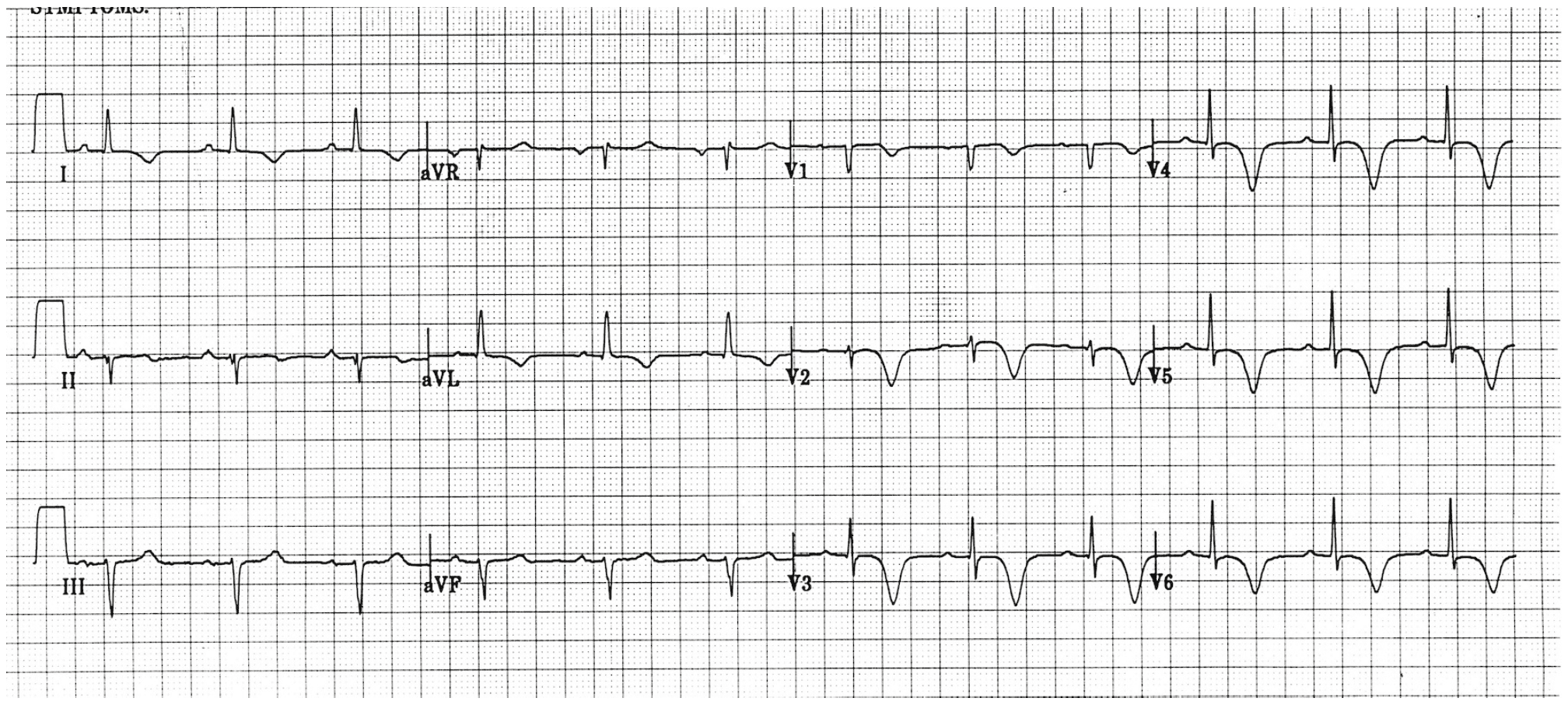
First Diagonal Branch of the Left Anterior Descending Artery Occlusion
- The 1st diagonal branch (D1) of the LAD supplies blood to the anterolateral wall of the left ventricle
- Look for:
- STE in aVL and V2
- Upright T-waves in aVL and V2
- ST-Depression and inverted T waves in Inferior Leads (III and aVF)
- STE in aVL and V2 + lack of STE in other precordial leads = 89% PPV for MI of the anterior wall caused by a D1 lesion
Image From: Macias M et al. Am J Emerg Med 2015
De Winter’s T Waves
- Concerning for proximal LAD occlusion (Present in 2% of patients)
- Look for:
- Upsloping ST-Depression at J Point in leads V1 – V4 without STE
- Tall, Symmetric T-Wave in leads V1 – V4
- STE in lead aVR +/- aVL
Images From: LITFL Blog
Left Main Coronary Artery Stenosis
- Look for:
- STE in lead aVR AND/OR
- Widespread ST-Depression
- In one study STD in leads I, II, and V4 – V6 + STE in aVR present in 90% of patients with greater than 70% stenosis of the LMCA
- Left Main Coronary Artery Occlusion will have the same findings as above but patients will be in cardiogenic shock if not coding
Image From: LITFL Blog
Wellens’ Syndrome
- Concerning for proximal critical high grad LAD occlusion
- Consider Wellens’ if:
- Active (or recent) angina chest pain
- Minimal or no cardiac biomarker elevation
- Absence of pathologic precordial Q waves
- Minimal or lack of STE (<1mm)
- No loss of precordial R-wave progression
- Characteristic T-wave abnormalities
- Two Types of Wellens’ Syndrome:
- Type A (25% of cases) consists of biphasic t waves
- Type B (75% of cases) consists of deep symmetric t waves
- Provocative Stress Testing could prove to have disastrous consequences resulting in AMI and fatal dysrhythmias
- AMI can occur within a mean of 6 – 8.5d after admission, but a mean of 21.4d after symptoms
- T-wave changes may be transient or resolve with medical management
- Look for:
- Deeply inverted T-waves in leads V1 – V4 OR
- Biphasic T-waves in leads V1 – V4
Wellens’ Type A (Image From: LITFL Blog)
{kind=link}
Wellens’ Type B (Image From LITFL Blog)
Wellens Type A (Image From LITFL Blog)
{kind=link}
Wellens Type B (Image From LITFL Blog)
Posterior Wall AMI
- Concerning for occlusion of either distal left circumflex artery or PDA of right coronary artery
- If you see STD in leads V1 – V3, the next thing to do is get a posterior ECG with leads V7 – V9 to help differentiate posterior AMI vs Anterior Ischemia
- Look for:
- Horizontal (flat) ST-Depression in leads V1 – V3
- Prominent R-wave in leads V1 – V2
- Upright T-wave in leads V1 – V3
Posterior STEMI (Image From LITFL Blog)
Posterior STEMI with Posterior Leads (Image From LITFL Blog)
Placement of Posterior Leads
Clinical Bottom Line: It is important to recognize the above 5 patterns as these are high risk ACS patients because a significant portion of the left ventricle is at jeopardy. Only 4 of the above diagnoses require activation of the cath lab immediately and the 5th requires consultation of interventional cardiology.
Cath Lab Activation:
- 1st Diagonal Branch of the Left Anterior Descending Artery Occlusion
- de Winter’s T Waves
- Left Main Coronary Artery Occlusion
- Posterior STEMI
Interventional Cardiology Consultation:
- Wellens’ Syndrome
References:
- Macias M et al. The Electrocardiogram in the ACS Patient: High-Risk Electrocardiographic Presentations Lacking Anatomically Oriented ST-Segment Elevation. Am J Emerg Med 2015. [epub ahead of print]. PMID: 26742458
For More Thoughts on This Topic Checkout:
- Taming the SRU: STEMIs in Disguise
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)
The post Five ECG Patterns You Must Know appeared first on REBEL EM - Emergency Medicine Blog.