
{kind=link}
{kind=link}
Managing casualties in high-risk environments like active violent incidents, unstable buildings from explosion or earthquake, and houses on fire is inherently challenging. Adding the possibility of CBRN (chemical, biological, radiological, or nuclear) contamination to that management plan adds additional complexity.
While many fire departments have hazmat teams to deal with CBRN situations, the time pressures of managing traumatic injuries on a contaminated casualty may force medical management before specialized hazmat teams arrive.
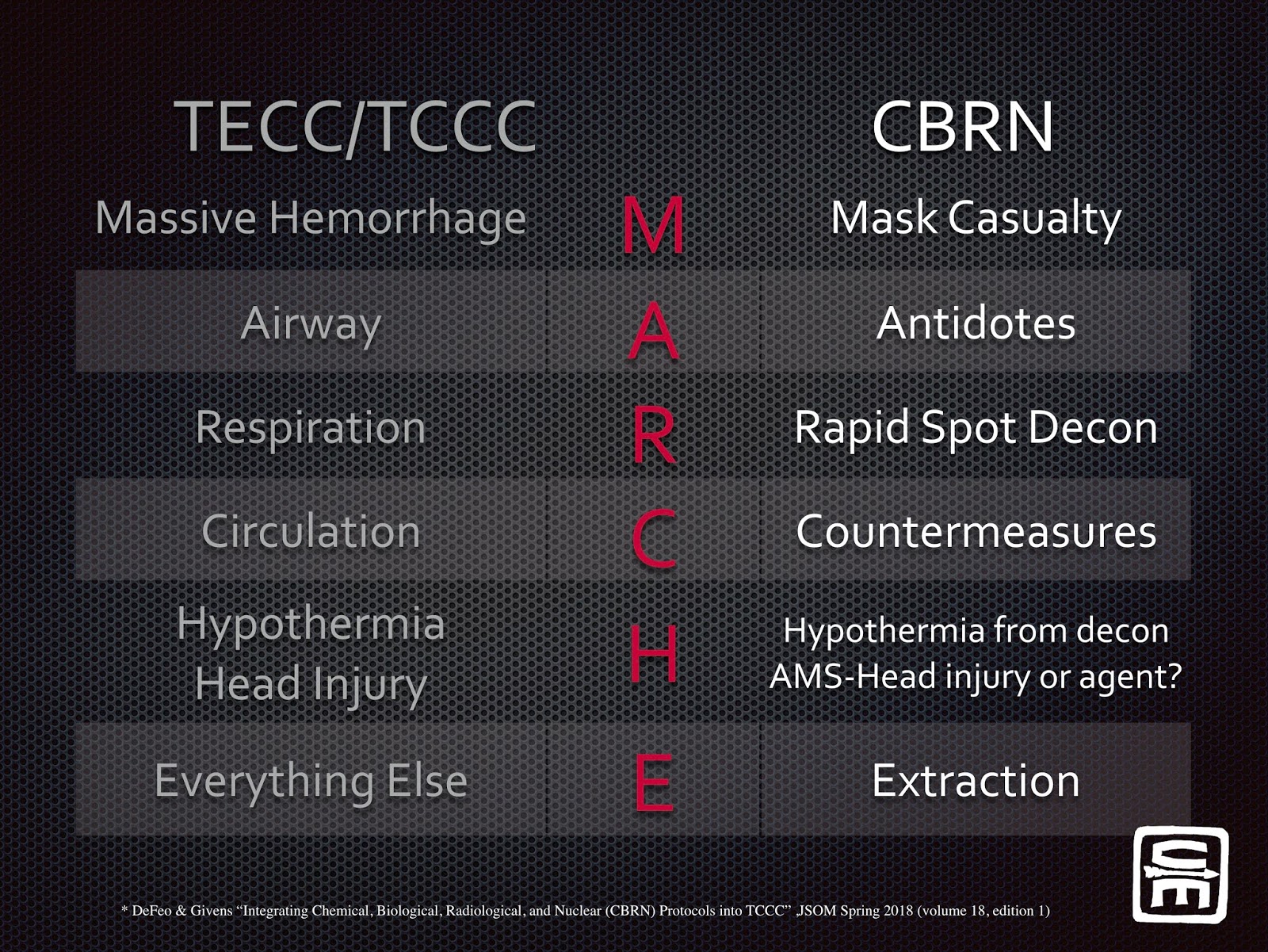
A must-read article for anyone interested in a systematic approach to managing trauma patients in a CBRN environment is Devon DeFeo’s article “Integrating Chemical, Biological, Radiological, and Nuclear (CBRN) Protocols into TCCC” published in the Journal of Special Operations Medicine Spring 2018 (volume 18, edition 1).
In this article, DeFeo and Givens outline how to combine TCCC and CBRN into what they call MARCHE2. The C-TECC Guidelines Committee will be publishing CBRN guidelines shortly.
The benefit of using the standard MARCHE mnemonic in high-risk environments is that each letter corresponds to a specific step in casualty management. Since casualties in a CBRN environment will likely also have traumatic injuries, using the same memory tool as an aid to CBRN patient treatment in these very complex situations can be useful and offer some “cognitive unloading” for the rescuers.
While we find it helpful anytime we are managing severely injured patients to ask the question “What is killing the casualty now,” DeFeo adds “is it the agent or the wound?”1 These questions become even more critical in a CBRN situation. For example, a lethal VX nerve agent exposure can kill a casualty within minutes. A mustard agent exposure could be fatal in hours to days. A mustard agent exposed casualty with massive hemorrhage will succumb to their bleeding long before the toxic effects of the agent exposure.
Patients with CBRN exposure are likely initially treated or found in the hot zone / care under fire / direct threat phase of care. “Sometimes the agent is like the bullet, think care under fire.”2 Any medical intervention you would not perform while taking fire probably shouldn’t be done at the casualty’s point of contamination either. Casualty management here is largely to extract the wounded and medical providers in the safest way possible, while only performing immediately life-saving interventions.
CIANURO y su ANTIDOTO "Nithiodote". MANEJO INTOXICACION POR HUMO DE INCENDIOS. SEMICYUC / CYANOKIT
Dr Ramon REYES, MD,
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
{kind=link}
Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/groups/PDFgratisMedicina #DrRamonReyesMD
https://www.facebook.com/DrRamonReyesMD
https://www.instagram.com/drramonreyesmd/
https://www.pinterest.es/DrRamonReyesMD/
https://twitter.com/eeiispain
Blog
http://emssolutionsint.blogspot.com/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html
TELEGRAM
Group https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q