




What Article are we Discussing:
- Ferguson I et al. Propofol or Ketofol for Procedural Sedation and Analgesia in Emergency Medicine – The POKER Study: A Randomized Double-Blind Clinical Trial. Ann Emerg Med 2016 [Epub Ahead of Print] PMID: 27460905
What They Did:
- Multicenter, Randomized Double-Blind Trial of adult patients requiring deep sedation
- Randomized to 1:1 ketofol vs propofol
- ≥18 years of age requiring deep procedural sedation
- Excluded if allergy to ketamine, soy products or eggs
Outcomes:
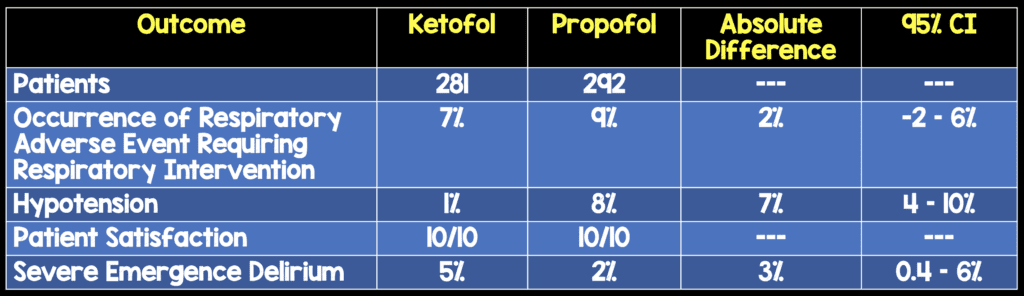
- Primary: Occurrence of respiratory adverse event requiring an intervention
- Desaturation SpO2≤93%
- Apnea = No Capnography Trace for ≥15seconds
- Hypoventilation = RR ≤8 breaths/min
- Laryngospasm
- Aspiration = Persistent hypoxia plus infiltrates on CXR
- Secondary:
- Hypotension SBP <90mmHg
- Patient Satisfaction
Results:

Strengths:
- Sedating physician, Procedural physician, Registered nurse, and patient were all blinded to contents of “study drug” syringes used
- Data available on primary outcome on all patients enrolled
- Largest study to compare ketofol in a 1:1 ratio in a single syringe with equivalent volumes of 1% propofol for ED procedural sedation and analgesia
Limitations:
- Convenience sample which could lead to a selection bias
- There was no control for prophylactic oxygen delivery or pre-procedural opiate use, which could have introduced confounders into the study.
- Use of a combined physiologic and intervention-based outcome measure is not an objective outcome. Different physicians will have different triggers that cause them to intervene. (i.e. The physiologic parameters are objective however physician intervention is subjective. )
- Australian studies on satisfaction may differ from US satisfaction
Discussion:
- This study was powered to demonstrate a reduction in the primary endpoint by 20 – 10%
- Hypotension occurred more often in the propofol arm vs the ketofol arm (8% vs 1% respectively). This was a statistically significant finding, however the clinical significance of this is questionable at best, as most patients hypotension was self limiting with only a few requiring a fluid bolus
- Although pain scores at 30 minutes post procedure were lower in the ketofol group, this did not affect patient satisfaction
- Labeling syringes with different medications, plus keeping track of how much of what medication you have given, seems to add additional math and the potential for more complications with dosing of ketofol, when there really hasn’t been any major improvements in patient oriented outcomes
- There have been 2 other studies that have compared propofol to ketofol for procedural sedation and analgesia:
- Andolfatto G et al 2012: Randomized, double-blind trial of ketofol vs propofol of 284 patients with a primary outcome of adverse respiratory events. Adverse respiratory events were experienced in 30% of patients receiving ketofol and 32% in the propofol group, which was not statistically significant. [2]
- Miner JR et al 2015: Randomized, double-blind trial of propofol, 1:1 ketofol, vs 4:1 ketofol of 271 patients with a primary outcome of frequency of airway and respiratory adverse events leading to an intervention. The primary outcome occurred in 29% of the propofol group, 19% in the 1:1 ketofol group, vs 32% in the 4:1 ketofol group which was also not statistically significant. [3]
Author Conclusion: “Ketofol and propofol resulted in a similar incidence of adverse respiratory events requiring the intervention of the sedating physician. Although propofol resulted in more hypotension, the clinical relevance of this is questionable, and both agents are associated with high levels of patient satisfaction.”
Clinical Take Home Point: It appears that in adults requiring procedural sedation and analgesia, Ketofol has a similar incidence of adverse respiratory events requiring intervention when compared to propofol, but with the hypothetical addition of increased complexity of keeping track of multiple medications and syringes, that MIGHT LEAD to more medication errors (if you don’t play your cards right). At this time I would recommend folding your hand when it comes to ketofol.
References:
- Ferguson I et al. Propofol or Ketofol for Procedural Sedation and Analgesia in Emergency Medicine – The POKER Study: A Randomized Double-Blind Clinical Trial. Ann Emerg Med 2016 [Epub Ahead of Print] PMID: 27460905
- Andolfatto G et al. Ketamine-Propofol Combination (Ketofol) Versus Propofol Alone for Emergency Department Procedural Sedation and Analgesia: A Randomized Double-Blind Trial. Ann Emerg Med 2012; 59 (6): 504 – 12. PMID: 22401952
- Miner JR et al. Randomized, Double-blinded, Clinical Trial of Propofol, 1:1 Propofol/Ketamine, and 4:1 Propofol/Ketamine for Deep Procedural Sedation in the Emergency Department. Ann Emerg Med 2015; 65: 479 – 488. PMID: 25441247
For More Thoughts on This Topic Checkout:
- Salim Rezaie at ALiEM: Ketofol – Is this the “Game Changer” of Procedural Sedation and Analgesia?
- Simon Carley at St. Emlyn’s: JC – Is Ketofol Worth the Hassle?
- Scott Magee at The Bottom Line: Propofol or Ketofol for Procedural Sedation and Analgesia in Emergency Medicine: The POKER Study
Post Peer Reviewed by: Scott Wieters (Twitter: @EMedCoach)
The post The POKER Trial: Go All in on Ketofol? appeared first on REBEL EM - Emergency Medicine Blog.