
{kind=link}
Background
Bleeding patients or those undergoing procedures that are at high risk of bleeding may require correction of their INR. Multiple products can be used to achieve this, including fresh frozen plasma (FFP). FFP contains many substances, including clotting factors, fibrinogen, plasma proteins, electrolytes, and anticoagulant factors. It is sometimes said that the intrinsic INR of FFP is approximately 1.6-1.7 and that it’s not possible to achieve a lower INR. This pearl will further explore these concerns.
Evidence
- What is the INR of FFP?
- The mean INR of FFP appears to be ~1.1 (0.9-1.3) [1,2].
- Reports that the intrinsic INR of FFP is 1.6-1.7 may be based on the clinical experience of not being able to achieve an INR <1.6-1.7 with FFP.
- Is it possible to “normalize” the INR with FFP alone?
- Several studies have found that it’s difficult to achieve an INR <1.7 with only FFP [3,4]. However, other studies were able to achieve lower average INR values [2,5,6].
- Overall, these studies found that there was a significantly greater decrease in INR when the pre-FFP INR was higher, but there was a much smaller decrease when the INR was closer to the normal range.
- Why does FFP appear to have diminishing returns when the pre-FFP INR is lower?
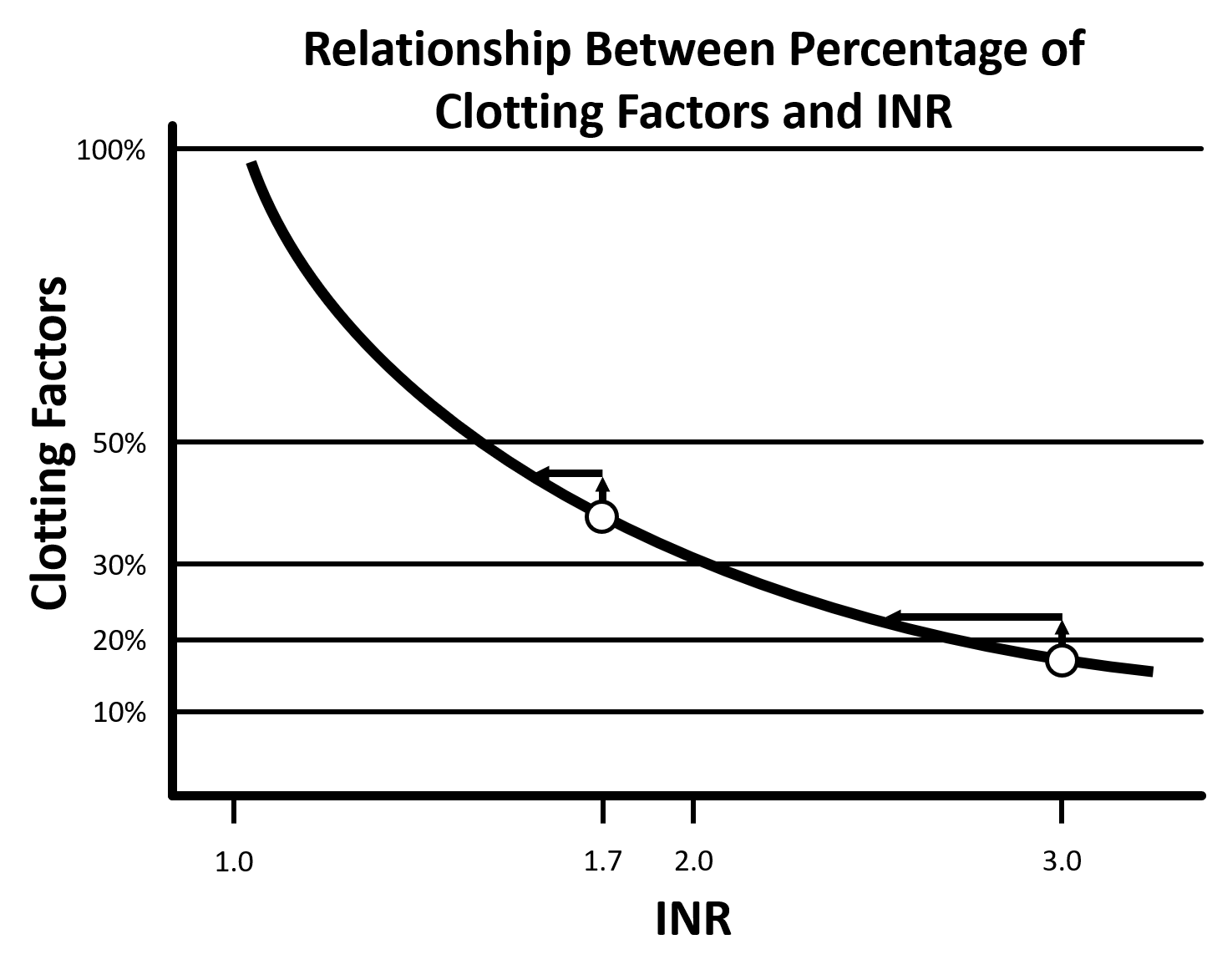
- The relationship between the INR and percentage of clotting factors present in the blood is not linear (see figure) [7].
- For example: An increase of ~5% in clotting factors may decrease the INR from 3 to 2.5 but the same amount of FFP may only reduce an INR of 1.7 to 1.6.
{kind=link}
-
- Additionally, the table below also demonstrates that small volumes of FFP result in large changes when the initial INR is elevated, but very large amounts of FFP are required to achieve an INR of 1.3 no matter the initial INR (see table).
| Amount of FFP to Achieve a Target INR Based on Pre-FFP INR | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Target INR | |||||||||
| 1.3 | 1.7 | 3.0 | |||||||
| Initial INR | Volume (L) | Dose (mL/kg) | Factor (%) | Volume (L) | Dose (mL/kg) | Factor (%) | Volume (L) | Dose (mL/kg) | Factor (%) |
| 6.0 | 4.5 | 64 | 45 | 2.5 | 36 | 25 | 1.5 | 21 | 15 |
| 5.0 | 4.3 | 61 | 43 | 2.3 | 32 | 23 | 1.0 | 14 | 10 |
| 4.0 | 4.0 | 57 | 40 | 2.0 | 29 | 20 | 0.5 | 7 | 5 |
| 3.0 | 3.5 | 50 | 35 | 1.5 | 21 | 15 | – | – | – |
| 2.0 | 2.5 | 36 | 25 | 0.5 | 7 | 5 | – | – | – |
-
- Given the above data, the issue preventing the achievement of an INR <1.7 appears to be the dose/volume of FFP required and not the intrinsic INR of FFP.
- Does the INR need to be <1.7 to achieve hemostasis?
- Since the INR only provides limited information regarding a single aspect of anticoagulation status, complete normalization for the INR to control bleeding is usually not necessary [6].
- An INR elevation alone does not indicate a patient is coagulopathic or at an increased risk of bleeding [7]. Additionally, an INR elevation in patients with liver dysfunction likely reflects an overall state of decreased factor production, both procoagulant and anticoagulant factors [8].
- The target INR varies depending on multiple patient factors and planned interventions, but an INR of 1.0 is likely not necessary to prevent bleeding or achieve hemostasis.
Bottom Line
- A unit of FFP has an INR of ~1.1, but this doesn’t mean it can easily normalize the INR.
- There is a non-linear relationship between percentage of clotting factors and the INR, resulting in diminishing returns from each unit of FFP as the INR decreases.
- Very large doses of FFP may be required to fully correct an elevated INR, which frequently precludes its use.
- Complete normalization of the INR is not required to achieve hemostasis or prevent bleeding from a procedure.
Want to learn more about EM Pharmacology?
Read other articles in the EM Pharm Pearls Series and find previous pearls on the PharmERToxguy site.
References
- Holland LL, Foster TM, Marlar RA, Brooks JP. Fresh frozen plasma is ineffective for correcting minimally elevated international normalized ratios. Transfusion. 2005;45(7):1234-1235. doi: 10.1111/j.1537-2995.2005.00184.x. PMID: 15987373.
- Only AJ, DeChristopher PJ, Iqal O, Fareed J. Restoration of normal prothrombin time/international normalized ratio with fresh frozen plasma in hypocoagulable patients. Clin Appl Thromb Hemost. 2016;22(1):85-91. doi: 10.1177/1076029614550819. PMID: 25294634.
- Holland LL, Brooks JP. Toward rational fresh frozen plasma transfusion: The effect of plasma transfusion on coagulation test results. Am J Clin Pathol. 2006;126(1):133-139. doi: 10.1309/NQXH-UG7H-ND78-LFFK. PMID: 16753596.
- Abdel-Wahab OI, Healy B, Dzik WH. Effect of fresh-frozen plasma transfusion on prothrombin time and bleeding in patients with mild coagulation abnormalities. Transfusion. 2006;46(8):1279-1285. doi: 10.1111/j.1537-2995.2006.00891.x. PMID: 16934060.
- Müller MCA, Straat M, Meijers JCM, et al. Fresh frozen plasma transfusion fails to influence the hemostatic balance in critically ill patients with a coagulopathy. J Thromb Haemost. 2015;13(6):989-997. doi: 10.1111/jth.12908. PMID: 25809519.
- McCully SP, Fabricant LJ, Kunio NR, et al. The International Normalized Ratio overestimates coagulopathy in stable trauma and surgical patients. J Trauma Acute Care Surg. 2013;75(6):947-953. doi: 10.1097/TA.0b013e3182a9676c. PMID: 24256665.
- Dzik W “Sunny.” Reversal of drug-induced anticoagulation: old solutions and new problems. Transfusion. 2012;52(s1):45S-55S. doi: 10.1111/j.1537-2995.2012.03690.x. PMID: 22578371.
- Harrison MF. The misunderstood coagulopathy of liver disease: a review for the acute setting. West J Emerg Med. 2018;19(5):863-871. doi: 10.5811/westjem.2018.7.37893. PMID: 30202500.
Author information
The post INR reduction with FFP – How low can you go? appeared first on ALiEM.