



REBEL Cast Ep96: Heroin OD – Is a 2-Hour Observation Protocol Long Enough?
Article: Heaton et al. Retrospective Review of Need for Delayed Naloxone or Oxygen in Emergency Department Patients Receiving Naloxone for Heroin Reversal. JEM 2019. PMID: 30961922
Clinical Question: What is the safety of a 2-hour observation period for heroin overdose patients who have received naloxone?
What They Did: A single-center retrospective chart review of patients who presented to the emergency department for heroin overdose who received naloxone (n=806). The primary outcome was the rate of intervention, grouped by length of observation period at the time of intervention.
Primary Outcome: Observed rate of intervention (i.e. repeat dose of naloxone or supplemental oxygen) 2 hours after the initial naloxone dose
Inclusion: Patients who presented to the emergency department for heroin overdose between January 1, 2009 through December 31, 2014 who received naloxone
Exclusion Criteria:
- If the chart did not indicate that heroin overdose was the cause of the presentation to the emergency department (e.g., if the chart noted opioids but did not specify the type of opioid or if the chart noted prescription opioid use)
- Missing prehospital or emergency department chart data (i.e. route, dosage, and time of initial naloxone dose)
Results:
1384 patient visits were for heroin-related complaints, and only 844 patients received naloxone. For demographics, most patients were male, and the most common mode of transportation was by ambulance. Most patients in this cohort used heroin intravenously, 13% required 2 doses of naloxone, 2.5% required ≥3 doses of naloxone, and most patients received naloxone prehospitally (78%). Polysubstance use that included other opioids were excluded from the study, but other coingestants were common.
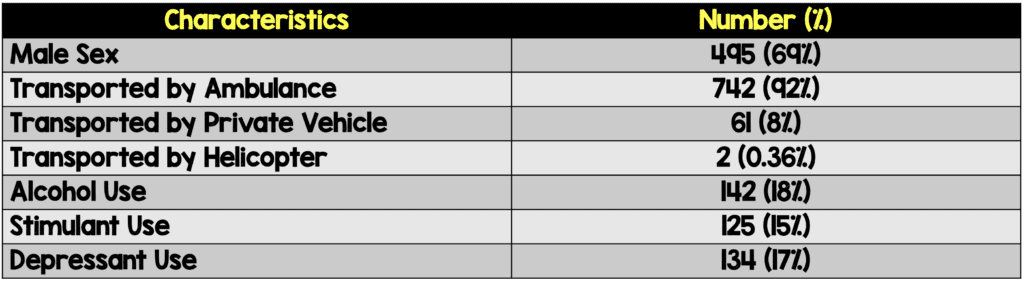

Table: Demographics
The median initial naloxone dose was 2.0 mg. For patient outcomes, 5 percent were intubated by the prehospital team and 2 percent were intubated by the emergency physician in the emergency department. 80 percent of patients were discharged home, 8 percent were admitted to the medicine floor, 3 percent were admitted to the ICU, 5 percent were admitted to psychiatry, and 2 percent left against medical advice. 0.62% (5 patients) died as a result of heroin. 7 patients experienced pulmonary edema, and 6 of 7 of the cases of pulmonary edema were identified before 2 hours of observation.
37 patients (4.6% of patients) required an intervention, either supplemental oxygen or repeat naloxone dosing, greater than 2 hours after the observation period began. 15 patients (1.9% of patients) required either supplemental oxygen or repeat naloxone dosing greater than 3 hours after the observation period began. 7 patients (0.9% of patients) required either supplemental oxygen or repeat naloxone dosing greater than 4 hours after the observation period began.


Table: Patients who required repeat naloxone or supplemental oxygen, hours after observation period began
56% (n=458) of patients were found to have polysubstance use, as determined by self-report and toxicological testing (urine or serum testing). Depressant use (e.g., barbiturates, benzodiazepines, or antipsychotics) was correlated with the use of repeat naloxone doses (p < 0.01).
Strengths:
- This study provides further evidence for a topic that is controversial in emergency medicine and toxicology literature, and heroin overdose is frequently encountered in the emergency department
Limitations:
- This study was only for patients presenting with reported heroin overdose and does not apply to other opioids; however, both in this study and in practice it is often difficult to determine what substance was used
- Routes of administration of heroin may affect the pharmacokinetics
- Intranasal naloxone has different pharmacokinetics than intravenous or intramuscular naloxone, with persistence of plasma concentrations for a longer duration of time (5)
- The outcome of requiring supplemental oxygen or repeat naloxone dosing are influenced by individual physician practice, and perhaps a more objective primary outcome would have been better (i.e. the reason for supplemental O2 was not present for every patient)
- Repeat naloxone administration is a surrogate for recurrent opioid toxicity. It is unclear whether repeat doses were given due to hypoxia, altered mental status, or other reasons
- If naloxone was given by EMS en route to the hospital, the time at presentation to the emergency department was listed as the time naloxone was administered. It is important to note that this study was therefore testing for the duration of the observation period and not the time from naloxone administration in all cases
- The number of patients with polysubstance use and preexisting conditions was too small for analysis of these subgroups
- The true rate of polysubstance use is most likely underestimated in this trial as self-reporting was used instead of toxicology screens on every patient. Although toxicology testing can confirm a particular substance it does not necessarily indicate intoxication at the time the test was performed
Discussion:
- This study found that 4.6% of patients required an intervention of either repeat naloxone dosing or supplemental oxygen after 2 hours of observation. This study provides evidence against the 1-hour observation period (4). Also, although this study was not designed specifically for prehospital medicine, it provides evidence against non-transportation of patients after treatment with naloxone.
- The majority of patients (60%) who required interventions after 2 hrs received naloxone dosages ≥2mg and 90% received naloxone dosages ≥1mg. Additionally all but one case of pulmonary edema (6 out of 7) and aspiration pneumonia (16 of 17) were evident within 2hrs of ED arrival. An observation period of 3 hours would have identified all but 2 of these cases (1 for each adverse event).
- We have discussed the HOUR protocol before on REBEL EM (Link is HERE ) looking at a 1-hour observation protocol and felt it was too focused on throughput and missed too many complications. In that cohort only 1 patient required an additional dose of naloxone after the 1 hour mark. However, if the patients in this trial were used, a one-hour observation period would have missed significantly more complications (i.e. repeat naloxone dosing or O2 administration).
Authors’ Conclusions:
“A 2-h ED observation period for heroin overdose patients reversed with naloxone resulted in a delayed intervention rate of 5%. Clinicians may consider a 3-h observation period, with extra scrutiny in polysubstance abuse.”
Clinical Take-Home Point:
A 1-hour observation period after naloxone administration for suspected heroin overdose is too short a period of observation. Consider at least a 3-hour observation period and perhaps longer if the patients have consumed coingestants.
References:
- Heaton et al. Retrospective Review of Need for Delayed Naloxone or Oxygen in Emergency Department Patients Receiving Naloxone for Heroin Reversal. JEM 2019. PMID: 30961922
- Nelson L, Lewin N, Howland MA, Hoffman R, Goldfrank L, Flomenbaum N. Goldfrank’s Toxicologic Emergencies. 9th ed. New York, NY: McGraw-Hill Medical; 2015.
- Willman MW et al. Do Heroin Overdose Patients Require Observation After Receiving Naloxone? Clin Toxicol 2017. PMID: 27849133
- Clemency BM et al. Hospital Observation Upon Reversal (HOUR) with Naloxone: A Prospective Clinical Prediction Rule Validation Study. Acad Emerg Med 2019. PMID: 30592101
- McDonald R et al. Pharmacokinetics of Concentrated Naloxone Nasal Spray for Opioid Overdose Reversal: Phase I Healthy Volunteer Study. Addiction. 2018. PMID: 29143400
For More on This Topic Checkout:
- REBEL EM: The HOUR Trial – Clinical Decision Rule for Opioid OVerdose Patients in the Emergency Department
- Tox and Hound: Great! Naloxone Worked! Now What?
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Cast Ep96: Heroin OD – Is a 2-Hour Observation Protocol Long Enough? appeared first on REBEL EM - Emergency Medicine Blog.