
ANC = WBC x (neutrophil% + band%)
- Mild: 1000 – 1500
- Mod: 500 – 1000
- Severe: 100 – 500
- Profound: <100
Background:
- Neutrophils directly combat infection and are important to coordinating the body’s overall immune response.
- The loss of these cells leads to immunosuppression as well as decreased responsiveness of the immune system as a whole
- Patients with neutropenia will not only get very sick very quickly, but also will have blunted immune response and may not localize signs of infection well
- Fever or malaise may be their only presenting symptoms.
- Patients with hematologic malignancies are at highest risk for suffering profound and prolonged neutropenia. Particularly high risk are those undergoing induction chemotherapy or stem cell transplant. Allogeneic stem cell grafting is higher risk than autologous.
Neutropenic Fever: Fever (one reading of 38.3C or sustained 38.0C) + ANC < 500 cells/mm3 or expected to fall to < 500 cells/mm3 within the next 48 hours
Common problem during chemotherapy:
- 10-50% of patients with solid malignancy and >80% of patients with hematologic malignancy will experience at least one episode of neutropenia (IDSA 2010, Klastersky 2004 )
- Associated with high morality:
- ~90% without antibiotics (Perron 2014 , Klastersky 2009 )
- ~2-21% when treated with early antibiotics (Clarke 2011 , Kruderer 2006 )
- Higher mortality rates with co-morbidities and hematologic malignancies
- Time to antibiotic administration has been shown to directly impact mortality (Perron 2014 , Rosa 2014 , Marín 2015 )
Causes of Neutropenia (Gibson 2014 ):
- Overconsumption
- Sepsis
- Autoimmune disease (SLE, rheumatoid arthritis, etc)
- Underproduction by bone marrow
- Malnutrition – alcoholism, anorexia, etc
- Myelodysplastic syndrome
- Post-viral: varicella, measles, rubella, influenza, hepatitis, Epstein-Barr virus, HIV
- Drug induced: clozapine, methimazole, sulfasalazine, bactrim, b-lactam antibiotics, NSAIDs, ticlopidine, cephalosporins, chemotherapy
Chemotherapy:
- Includes many drugs and drug regimens, all with the goal of killing rapidly dividing cells. Of note, this particularly affects:
- Cancer cells – this is the reason chemotherapy works as treatment
- Neutrophils – with a life cycle of only 1-6 days, their numbers are impacted dramatically by chemotherapy
- Mucosa – destruction of dividing cells thins mucosal barriers, putting these patients at high risk for mucositis and bacterial invasion
- This creates a dangerous situation where the body’s barriers against bacterial invasion are broken down and, thus, the ability to combat infection is severely blunted. Antibiotics are effectively the only thing standing between these patients and overwhelming sepsis
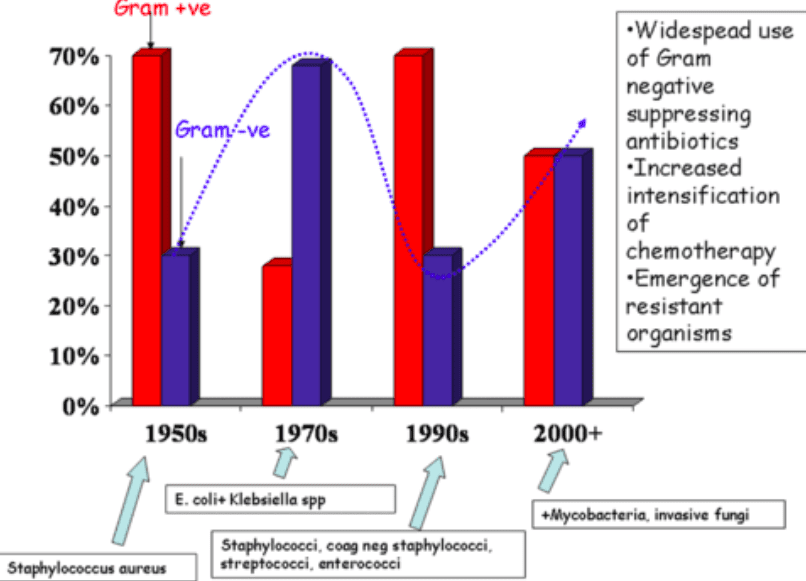
Pathogens (Gudiol 2013 ) :
- The pathogens responsible for neutropenic fever have changed over time.
- Initially, Gram (-) organisms translocated from the gut caused majority of cases of neutropenic fever
- This changed in the 1990s. Gram(+) infections became more common due to more fluoroquinolone prophylaxis against Gram (-) organisms and due to more prevalent use of indwelling catheters for outpatient treatment
- Over the past decade, there has been a resurgence of Gram (-) organisms due to increasing antibiotic resistance, particularly multidrug resistant E coli and klebsiella
- Given the increasing rates of antibiotic resistance, antibiotic stewardship is becoming increasingly important
- In the ED, we can contribute to antibiotic stewardship by checking old cultures and obtaining new ones prior to initiation of antibiotics
{kind=link}
ED Evaluation and Management:
- Resuscitate if necessary
- Patients with neutropenic fever may rapidly progress to septic shock
- Give appropriate fluids, vasopressors, and antibiotics
- Antibiotics need to be given as quickly as possible if unstable
- Perform a complete review of systems and physical exam looking for signs of focal infection
- Basic Blood Work
- CBC, BMP, LFTs, bilirubin levels
- Blood cultures
- If indwelling catheter present: 1 set from each line of indwelling catheter + 1 peripheral set
- If no indwelling catheter present: 2x peripheral sets
- Additional testing based on signs and symptoms:
- Respiratory symptoms
- Chest X-Ray
- Sputum cultures
- Dysuria
- Urinalysis
- Urine culture
- Abdominal pain
- CT abdomen and pelvis
- If diarrhea present, consider C difficile PCR (if available)
- Basic Blood Work
- Isolation
- Good hand hygiene is the most effective way to prevent these patients obtaining nosocomial infections
- Use standard barrier precautions
- Keep anyone with potentially communicable illness out of the patient’s room – visitors, other patients, or healthcare workers
- Any stem cell transplant patient should be in a private room. If they have an allogenic transplant, use a HEPA filter with >12 air exchanges per hour
- Isolation is important for neutropenic patients, but do not let waiting on an isolation room delay obtaining cultures and initiating antibiotics
- Specific Pathologies
- Mucositis
- Mucositis is a high risk feature indicative of bacterial invasion through thinned mucus membrane barriers
- Signs and Symptoms
- Oral pain, erythema, edema, or lesions
- Sinus pain or pressure
- Rectal pain or lesions, any swelling suggestive of perirectal abscess
- Abdominal pain
- Inspect the rectum for swelling possibly indicative of perirectal abscess.
- Digital rectal exam is generally discouraged due to concern of inducing bacteremia if mucus membranes are damaged in the process (CDC 2005 )
- Mucositis
{kind=link}
- Neutropenic Enterocolitis (Typhlitis)
- A feared complication of neutropenic fever is direct bacterial invasion of the intestinal mucosa causing necrotizing infection
- Most commonly at the ileocecal junction
- It presents with classic triad of neutropenia, fever, and RLQ pain. Mortality approaches 50% when present (Gorschlüter 2005 )
- Surgery is avoided unless the bowel perforates, as these patients have poor wound healing and high surgical complication rates
{kind=link}
- Determine whether the patient is high or low risk
- High Risk Factors
- HD instability
- Hematologic malignancy
- Uncontrolled or widespread malignancy
- Induction chemotherapy / hematopoietic stem cell transplant
- ANC <100
- >7 days of ANC <500
- Medical comorbidities (particularly COPD, cardiac disease, or diabetes)
- Low Risk Factors
- HD stable
- Solid tumor malignancy
- ANC >500
- Neutropenia expected to last <7 days
- No comorbidities
- MASCC and CISNE risk calculators
- MASCC (MASCC Score)
- Low risk = 21-26
- High risk = <21
- The MASCC Score will identify more patients as low risk, but will have more treatment failures / bounce-backs than the CISNE score (Ahn 2017 , Coyne 2016 )
- MASCC (MASCC Score)
- High Risk Factors
-
- CISNE Score (CISNE Score)
- Low risk = 0
- Intermediate risk = 1-2
- High risk = 3-8
- CISNE Score (CISNE Score)
-
-
- The CISNE score will identify fewer patients as low risk, but will result in fewer treatment failures/bounce-backs than the MASCC score (Ahn 2017 , Coyne 2016 )
- Default to using whichever score your oncologist is more comfortable with
-
- Antibiotic Selection
- Check old cultures for prior infections and sensitivities (if available).
- Follow your hospital’s protocol (if available). This will have been formulated based on local resistance patterns and likely with input from your institution’s oncologists.
- High Risk Patients will need hospitalization and IV antibiotics.
- General approach for IV antibiotic therapy
- Begin with single broad spectrum agent which includes pseudomonas coverage such as cefepime, piperocillin-tazobactam, or a carbepenem
- Penicillin allergies other than anaphylaxis are not considered a contraindication to the use of cephalosporins such as cefepime
- If patient has anaphylactic reaction to penicillins, consider broad coverage with ciprofloxacin plus clindamycin or aztreonam plus vancomycin (IDSA 2010)
- Do not routinely start vancomycin. Add vancomycin if there is clinical suspicion for Gram (+) infection
- Signs of mucositis or cellulitis
- Indwelling catheter present on arrival
- Prior MRSA infection
- Patient already on Gram (-) prophylaxis such as fluoroquinolone
- Consider adding additional agents for unstable patients, or patients in which antibiotic resistant organisms are suspected (patient has known colonization or patient population has high endemic rates)
- MRSA: vancomycin, linezolid, or daptomycin
- VRE: linezolid or daptomycin
- Extended spectrum beta lactamase (ESBL) producing orgamisms: carbapenem
- Carbapenemase producing organisms (such as klebsiella): polymixin-colistin or tigecycline
- If there is clinical suspicion for influenza (or positive PCR testing), treatment with oseltamivir is recommended
- Other antiviral and antifungal agents should NOT be started routinely
- Antiviral + Antifungal Therapies
- Only start antiviral or antifungal therapies if the patient has a known viral or fungal infection (ex: patient spikes a fever while already on antifungal treatment) or if they have a clinical picture strongly suggestive of viral or fungal etiology
- Antifungals are generally not initiated until a patient has had >4 days of fever unresponsive to antibiotic treatment with no clear source identified
- Low risk patients
- If the patient has no high risk features, is found to be low risk on MASCC or CISNE scoring, and has good oncology follow-up, it may be preferable to discharge them home with 24hr oncology followup
- Send patients home ONLY after discussion with the patient’s oncologist and only if there are no high risk features present
- Outpatient antibiotic choice
- Ciprofloxacin plus amoxicillin-clavulanate is recommended by IDSA guidelines for oral empiric therapy (IDSA 2010)
- Levofloxacin or ciprofloxacin monotherapy, or ciprofloxacin plus clindamycin are less well studied but are commonly used
- Avoid fluoroquinolones if the patient is already on fluoroquinolone prophylaxis
Take Home Points:
- There are many causes of neutropenia, chemotherapy being by far the most dangerous
- Febrile neutropenia is a condition conveying high mortality. Early administration of antibiotics is the only factor known to reduce this mortality
- For a patient with neutropenic fever, remember that the body’s own flora is the greatest danger. Isolate, but do not wait to initiate treatment
- Check old blood cultures and obtain new cultures prior to starting treatment
- Identify low risk patients and send them home with PO antibiotics and close oncology follow-up in conjunction with your oncologist
Guest Post By
Joseph Bennett, MD
PGY3 Resident
NYU/Bellevue Emergency Medicine Residency
For More on This Topic Checkout:
- Infectious Disease Society of America 2010 Clinical Practice Guidelines
- Life in the Fast Lane: Febrile Neutropaenia
- Uptodate: overview of neutropenic fever syndromes
- EMRAP: Risk stratification of neutropenic fever
- MDCalc: MASCC Score
- MDCalc: CISNE Score
References:
- Ahn S et al. Comparison of the MASCC and CISNE scores for identifying low-risk neutropenic fever patients: analysis of data from three emergency departments of cancer centers in three continents. Support Care Cancer. 2018; 26(5):1465-1470. PMID: 29168032
- Clarke RT et al. Improving the immediate management of neutropenic sepsis in the UK: Lessons from a national audit. Br J Haem. 2011; 153(6):773-9. PMID: 21517822
- Coyne Cj et al. Application of the MASCC and CISNE Risk-Stratification Scores to Identify Low-Risk Febrile Neutropenic Patients in the Emergency Department. Ann Emerg Med. 2017;69(6):755-764. PMID: 28041827 .
- Ellis M. Febrile Neutropenia. Annals of New York Academy of Sciences. 2008;1138: 329-50. PMID: 18837909
- Freifeld AG et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America, Clin Infect Dis 2011: 52(4):e56-93. PMID: 21258094
- Gibson C, Berliner N. How we evaluate and treat neutropenia in adults. Blood. 2014 Aug 21;124(8):1251-8; quiz 1378. PMID: 24869938
- Gorschlüter M, Mey U, Strehl J, et al. Neutropenic enterocolitis in adults: systematic analysis of evidence quality. Eur J Haematol 2005; 75:1. PMID: 15946304
- Gudiol C et al. Changing aetiology, clinical features, antimicrobial resistance, and outcomes of bloodstream infection in neutropenic cancer patients. Clin Microbiol Infect 2013; 19:474. PMID: 22524597
- Klastersky J. The changing face of febrile neutropenia-from monotherapy to moulds to mucositis. Why empirical therapy? J Antimicrob Chemother. 2009;14(Suppl 1):i14–i15. PMID: 19372173
- Klastersky J. Management of fever in neutropenic patients with different risks of complications. Clin Infect Dis. 2004;39(Suppl. 1):S32–S37. PMID: 15250018
- Kuderer NM, Dale DC, Crawford J, Cosler LE, Lyman GH. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006;106(10):2258-66. PMID: 16575919
- Marín M et al. Factors influencing mortality in neutropenic patients with haematologic malignancies or solid tumours with bloodstream infection. Clinical Microbiology and Infection. 2015, 21:6, 583-590. PMID: 25680311
- Perron T, Emara M, Ahmed S. Time to antibiotics and outcomes in cancer patients with febrile neutropenia. BMC Health Services Research. 2014;14:162. PMID: 24716604
- Rosa RG, and Goldani LZ. Cohort Study of the Impact of Time to Antibiotic Administration on Mortality in Patients with Febrile Neutropenia. Antimicrob Agents Chemother. 2014 Jul; 58(7): 3799–3803. PMID: 24752269
- Stiff, PJ. Coding for Mucositis. From presentation at ICD-9-CM Coordination and Maintenance Committee Meeting. Loyola University Medical Center. Centers for Disease Control. Sept 30, 2005.
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie) and Anand Swaminathan, MD (Twitter: @EMSwami)
The post Neutropenic Fever appeared first on REBEL EM - Emergency Medicine Blog.