
{kind=link}
Pathophysiology
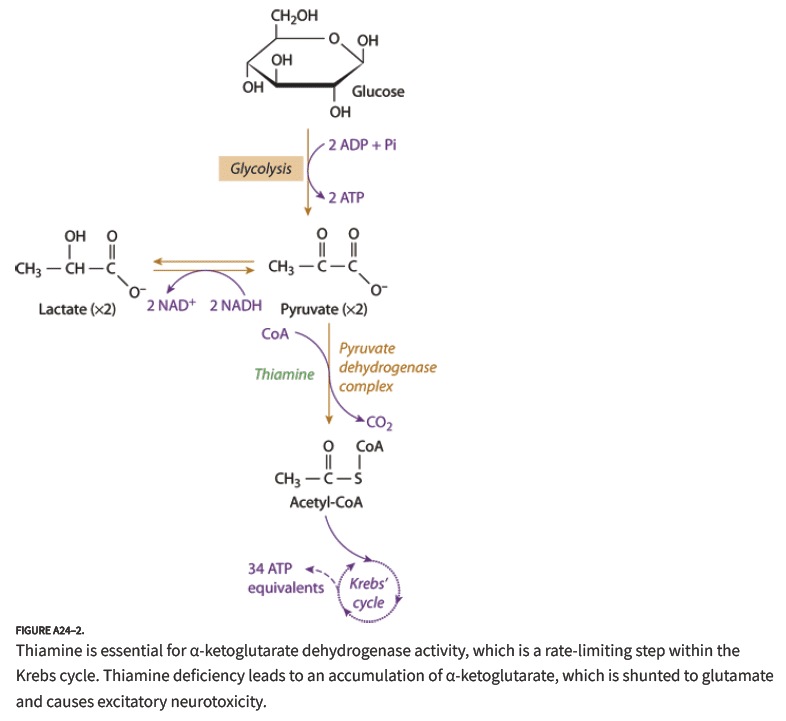
- Thiamine is a cofactor for the enzyme pyruvate dehydrogenase
- This enzyme converts pyruvate to acetyl-CoA
- Acetyl-CoA enters the Krebs cycle and ATP is produced
- Without thiamine, the Krebs cycle breaks down leading to ATP depletion affecting the brain and heart
At Risk Populations
- US incidence of 0.2 – 2% (Hoffman 2015 )
- Affects people with malnutrition or malabsorption
- Specific groups
- Chronic alcoholics
- Bariatric surgery patients
- AIDS patients
- Active malignancy
- Hyperemesis gravidarum
- Eating disorder patients
- Bone marrow transplant recipients
- CHF on furosemide (furosemide enhances renal elimination of thiamine)
History and Physical Examination
- Patients will have a history of malnutrition or malabsorption
- Classic Triad
- Ataxia
- Ophthalmoplegia (classically nystagmus and lateral rectus palsy)
- Altered Mental Status/Confusion
- All three features present in < 10% of patients (Donnino 2007 )
- Hypotension and hypothermia may be seen
- Elevated lactate levels are common due to interruption of the Krebs cycle (Donnino 2007 )
- Clinical Assessment Tool
- Dietary deficiencies
- Oculomotor abnormalities
- Cerebellar dysfunction
- Altered mental status or mild memory impairment
- > 2 of above components is diagnostic
Management
{kind=link}
- Preventive care: Thiamine 100 mg IV/IM
- Parenteral route recommended as many of these patients have abnormal GI absorption
- IV better than IM as many patents have diminished muscle mass making absorption less predictable
- Should be provided to all groups at risk of thiamine deficiency (see above)
- Unclear how long this provides protection for. Best estimates are about 1-2 weeks (Hoffman 2015 )
- Treatment of Wernicke’s Encephalopathy
- Basics
- Check glucose and supplement as needed
- Check electrolytes as concomitant electrolyte deficiencies (magnesium, potassium etc) are common
- Thiamine 500 mg IV Q8 X 3 days
- Follow with thiamine 250 mg IV Q24 X 3-5 days
- Ophthalmoplegia can improve in hours while altered mental status and ataxia are frequently more delayed in improvement if they improve at all
- Basics
Take Home Points
- Wernicke encephalopathy is characterized by ataxia, altered mental status and ophthalmoplegia but patients are unlikely to have all these components
- Suspect Wernicke encephalopathy in any patient that is at risk of malnutrition or malabsorption and has any one of the classic symptoms
- Prophylactic administration of thiamine 100 mg IV/IM to at risk patients can prevent development of the disease
- Once Wernicke encephalopathy has developed, it must be treated with high-dose, IV thiamine
Read More
- ER Cast: What You Don’t Know About Wernicke’s Encephalopathy
- LITFL: Thiamine Deficiency
- EMRAP: Remember to Take Your Vitamins
- ALiEM: Mythbusting the Banana Bag
References
- Hoffman RS. Antidotes in Depth. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR. eds. Goldfrank’s Toxicologic Emergencies, 10e New York, NY: McGraw-Hill; 2015. [Access Emergency Medicine ]
- Donnino MW et al. Myths and Misconceptions of Wernicke’s Encephalopathy: What Every Emergency Physician Should Know. Ann Emerg Med 2007; 50: 715-21. PMID: 17681641
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Wernicke Encephalopathy appeared first on REBEL EM - Emergency Medicine Blog.