
 EM Journal Update: Safety of Using Wells’ Clinical Model With D-Dimer To Manage Patients In The ED With Suspected Pulmonary Embolism
EM Journal Update: Safety of Using Wells’ Clinical Model With D-Dimer To Manage Patients In The ED With Suspected Pulmonary Embolism
Background: In the US, pulmonary embolism (PE) kills 100,000 people each year and over 360,000 new cases of PE are diagnosed each year (Horlander 2003). Currently, the gold standard for diagnosing PE is the computed tomographic pulmonary angiography (CTPA). Patients with PE present with varying symptoms, from anxiety and tachycardia, to shortness of breath and syncope. Thus, it is difficult to exclude this life-threatening diagnosis and thus far there is no validated method to exclude PE. Prior work from this group derived and validated Wells’ criteria for calculating clinical probability of PE, and using it to determine which patients should get serial ultrasonography, venography, or angiography after an equivocal ventilation perfusion (VQ) scan (Wells 1998). Now, this group examines how the D-dimer assay, together with Wells’ clinical model can help manage PE patients.
Clinical Question: Can the D-dimer assay be used with Wells’ clinical model to safely manage patients in the emergency department (ED) with suspected pulmonary embolism?
Article: Wells PS et al. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001; 135(2): 98-107. PMID: 11453709
Population: Adults > 18, who presented to four EDs in Canada with suspicion for PE, due to acute onset of new or worsening shortness of breath or chest pain, with symptoms for less than 30 days.
Exclusions: Suspected deep venous thromboembolism (DVT) in upper extremity as a likely source of PE, no symptoms of PE in the last 3 days, on anticoagulation for over 24 hours, expected survival less than 3 months, contrast media is contraindicated, pregnant, geographically inaccessible (unable to follow-up).
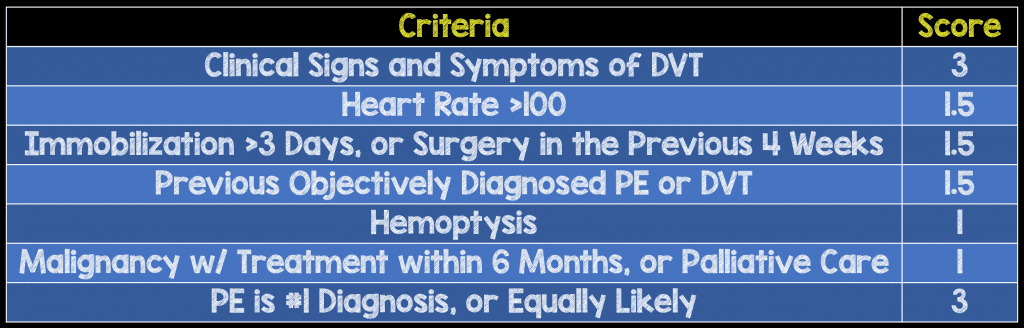
Intervention: Emergency Medicine doctors determined the clinical probability of PE using Wells’ criteria (Table 1.) as low, moderate, or high pre-test probability. All patients also had d-dimer testing.
Table 1. Wells’ criteria for calculating clinical probability of PE
Per the algorithm (Figure 1), those patients that had a low pre-test probability and a negative D-dimer, did not undergo any further testing and PE was considered excluded. All other patients underwent a VQ scan. If the VQ scan was non-diagnostic, patients had bilateral lower extremity deep venous ultrasonography.
Patients in whom PE was excluded, were followed for three months for venous thromboembolism (VTE) events.
![]()
Figure 1. Diagnostic algorithm for initial evaluation of patients with suspected PE.
Outcomes:
- Primary: Proportion of patients who had a VTE, during 3-month follow up, among patients in whom the diagnosis of PE had been excluded
- Secondary: Safety of combined clinical model and D-dimer when algorithm was followed correctly
Design: Prospective, cross-sectional
Primary Results:
-
946 patients enrolled in the study
- 16 patients excluded as they were lost to follow up
- 930 patients were included in the study
-
86 people (9.5%) were diagnosed with PE
- 81 during initial evaluation
- 5 during follow-up
Critical Results:
-
VTE at 3-month follow up after initial negative workup (primary outcome)
- Excluded by low probability Wells + negative D-dimer = 437
- PE during follow up n = 1 (0.2%)
-
849/946 patients had PE excluded during initial workup
- 5 patients developed VTE during follow up period
- 0.6% (95% CI 0.2 – 1.4%)
- 4 of these patients did not undergo the proper initial evaluation algorithm
-
Correct protocol followed (secondary outcome)
- n = 759/849 patients not initially diagnosed with PE
- 1 patient with VTE during 3-month follow up
- 0.1% (95% CI 0.0 – 0.7%)
-
D-dimer performance
- Entire population: NPV = 97.3% (95% CI 95.8 – 98.4%)
- Low probability drop: NPV 99.5% (95% CI 98.4 – 99.9%)

Strengths:
- Study focuses on a clinically important, patient centered outcome
- Study asks a question that had not previously been addressed
- All consecutive patients were evaluated, except for the 16 that relocated outside the study region
- Wells’ clinical model to determine pre-test probability has been previously validated
- Results analyzed per intention to treat
- Of the 12 patients who died during the study, none were determined to have died due to undiagnosed PE
- VQ scans were interpreted by nuclear medicine physicians who had no knowledge of outcomes or D-dimer testing results
- A committee blinded to all patient variables adjudicated suspected outcome events during follow-up
Limitations:
- Wells’ pre-test probability calculation relies heavily on the practitioner deciding whether PE is the #1 diagnosis or equally likely
- Patients lost to follow up were excluded from analysis (as opposed to being included as “positive VTE” for worst case scenario)
- Patient follow up by appointment or by phone call which introduces recall bias.
- While analysis was per intention-to-treat, 92 patients had fewer tests than indicated, and 7 of the patients diagnosed with PE had more tests than indicated.
- The prevalence of PE in the study population was low
- VQ scans were used at the time of this study to diagnose PE, but now CTPA is the gold standard. It is unclear how the use of CTPA would have affected the results
- Inadequate data reported to calculate specificity and likelihood ratios of Wells’ + D-dimer
- The authors comment on the potential reduction in diagnostic imaging but this was neither a primary or secondary outcome
- Patients who presented from 3:30pm – 7:00am were anticoagulated with LMWH and diagnostic testing was done in the next 18hrs. It is possible some PEs could have been missed, however this strategy is very generalizable to many institutions
- Compression ultrasonography, when indicated, was performed on both lower extremities from the common femoral vein to the trifurcation of the calf veins, but the calf veins were not examined which means some distal DVTs could have been missed
Discussion:
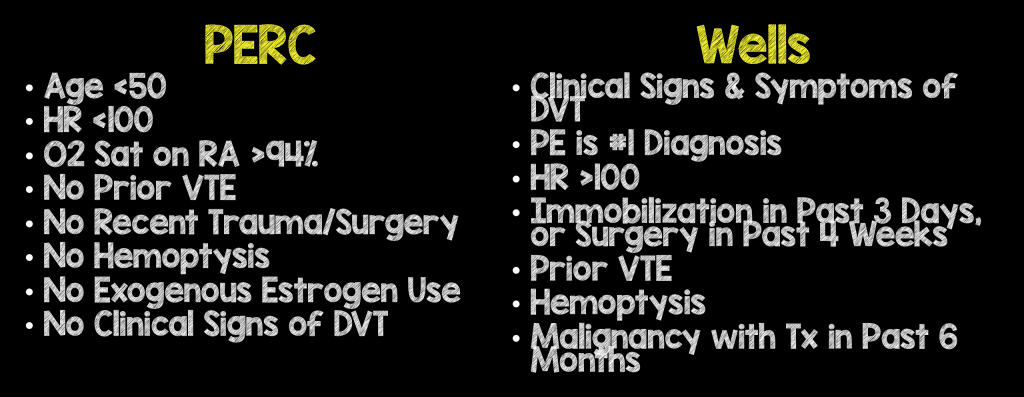
- This approach for ruling out PE has been further validated using the simplified Wells’ score (dichotomized to “PE unlikely” (score < 4) and “PE likely” (score > 5)) with a d-dimer (van Belle 2006) and has been found to perform well with an age-adjusted D-dimer (Kraaijpoel 2016)
- Since these studies, PERC was developed which allows clinicians to “rule-out” PE in patients with a low pre-test probability for PE (by gestalt, low Wells score, low Geneva or low simplified Wells) without obtaining a D-dimer

Authors Conclusions: “Managing patients for suspected pulmonary embolism on the basis of pretest probability and D-dimer result is safe and decreases the need for diagnostic imaging.”
Our Conclusion: Combined low PE pre-test probability (Wells’ criteria) and negative D-dimer has a very high NPV in excluding PE.
Potential to Impact Current Practice: Based on these results, patients with suspected PE who have a low pre-test probability per Wells’ criteria and a negative D-dimer can be discharged without further tests/imaging to work-up PE.
Bottom Line:
Wells’ criteria and D-dimer can be used to safely exclude PE in patients with a low pre-test probability and negative D-dimer.
Guest Post By:

References:
- Horlander KT et al. Pulmonary embolism mortality in the United States, 1979-1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163(14):1711-7. PMID: 12885687
- Wells PS et al. Use of a clinical model for safe management of patients with suspected pulmonary embolism. Ann Intern Med 1998; 129(12): 997-1005. PMID: 9867786
- Wiener RS et al. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(9):831-7. PMID: 21555660
- van Belle A et al. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA 2006; 259(2): 172-9. PMID: 16403929
- Kraaijpoel N et al. The performance of the original and simplified wells scores in combination with age-adjusted D-dimer testing in the diagnostic management of pulmonary embolism. Blood 2016. [Link HERE]
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Classic Journal Review – Wells + Dimer to Rule Out PE appeared first on REBEL EM - Emergency Medicine Blog.