
 Background: Acute migraine headaches are a common presentation to emergency departments. Treatment can be challenging: multiple medications are often required and allergies can limit options. Oral timolol maleate is approved by the FDA for migraine prophylaxis but is not typically effective once the migraine has started. There are some case reports of topical timolol in the treatment of acute migraine headaches [2][3] and a research letter [4] describing the use of timolol eyedrops in the treatment of acute migraine headaches. The research letter was a randomized trial of 10 patients that was not masked and therefore no definitive conclusions could be made.
Background: Acute migraine headaches are a common presentation to emergency departments. Treatment can be challenging: multiple medications are often required and allergies can limit options. Oral timolol maleate is approved by the FDA for migraine prophylaxis but is not typically effective once the migraine has started. There are some case reports of topical timolol in the treatment of acute migraine headaches [2][3] and a research letter [4] describing the use of timolol eyedrops in the treatment of acute migraine headaches. The research letter was a randomized trial of 10 patients that was not masked and therefore no definitive conclusions could be made.
Paper: Kurian A et al. Short-Term Efficacy and Safety of Topical B-Blockers (Timolol Maleate Ophthalmic Solution, 0.5%) in Acute Migraine: A Randomized Crossover Trial. JAMA Ophthalmol 2020. PMID: 33001159
Clinical Question: Can topically applied timolol maleate ophthalmic solution, 0.5% reduce pain scores at the onset of a migraine better than placebo eyedrops?
What They Did:
- Single-center, randomized, double-masked placebo-controlled crossover trial in India
- Patients randomized to receive:
- Timolol: Timolol eyedrops, 0.5% + Hydroxypropyl methylcellulose, 0.3% eyedrops
- 1 drop of 0.5% timolol ophthalmic solution = 0.25mg of timolol
- Placebo: Placebo eyedrops + Carboxymethyl cellulose, 0.5% eyedrops (i.e. artificial tears)
- Patients instructed to use 1 drop of the assigned med in each eye at the earliest onset of migraine (aura or headache)
- Another drop could be used at 10min if there was no relief with the first drop
- If no pain relief at 20min after pain onset, patients were free to use any other oral medication for pain relief:
- Acetaminophen
- Metoclopramide
- Prochlorperazine
- Prophylactic anti-migraine meds were not allowed
- Timolol: Timolol eyedrops, 0.5% + Hydroxypropyl methylcellulose, 0.3% eyedrops
- After a 3-month treatment period, patients completed a 1-month washout period and were crossed over to receive the opposite treatment for a final 3 months
Outcomes:
-
Primary: Reduction in pain score 20min after the use of study medication
- Pain reduction by 4 points on a scale of 0 to 10 or pain to zero 20 min after instillation of eyedrops
-
Secondary:
- Nonuse of an oral rescue medication
- A reduction in pain score of 0 to 4 on the pain scale at 20min without the use of any oral rescue medication
- Adverse effects due to use of study medication
Inclusion:
- ≥12 years of age
- Negative urine pregnancy test for women of childbearing age
- Clinical diagnosis of migraine
- Not taking any antimigraine medications for at least 1 month
- Willingness to undergo 7 months of follow up
Exclusion:
- Known allergy or hypersensitivity to study meds
- Pregnant, breastfeeding or planning to become pregnant during the study
- Female patients of childbearing age not using a reliable means of contraception
- Patients with bronchial asthma, bradyarrhythmias, and cardiac dysfunction
- Patients with coexistent glaucoma, in whom use of topical B-blockers was anticipated
- Patients taking systematic B-blockers
- Patients taking meds for migraine, not willing to stop existing treatment for at least 1 month
- Obstruction of lacrimal drainage
Results:
- 50 patients randomized with migraine headache
- Mean age 27.3 years (32% were between 12 and 18 years of age)
- 42/50 patients were women
- Total of 619 migraine attacks
- 284 (46%) treated with timolol
- 271 (44%) treated with placebo
- 64 (10%) occurred during the washout period when no study medications were used
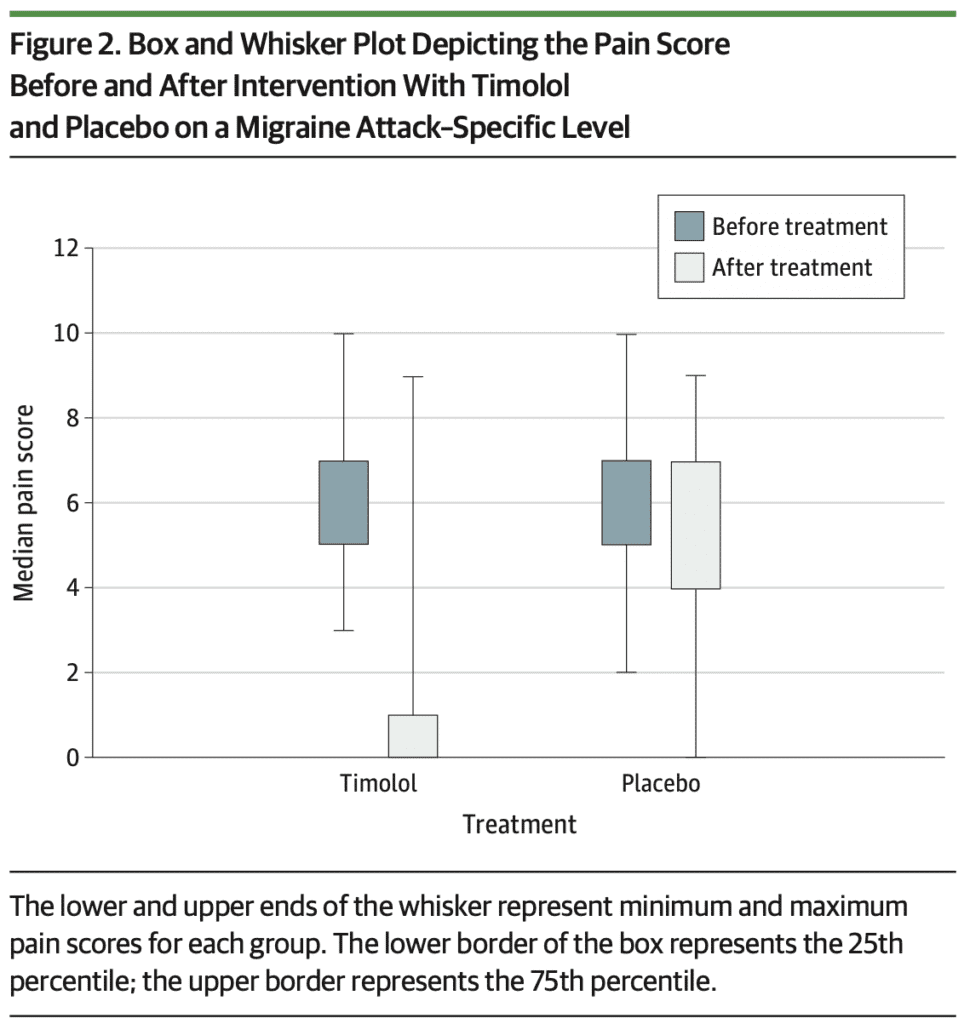
- Reduction in Pain Score by 4 Points, or to Zero, at 20 Min:
- Timolol: 233 attacks (82%)
- Placebo: 38 attacks (14%)
- Absolute Diff: 68%; 95% CI 62 to 74; p < 0.001
- 120 (42%) of the attacks treated with timolol required a second administration of drops after 10min
- Only 10 (4% of attacks treated with timolol and 11 (4%) of attacks treated with placebo recorded a pain score of ≤3
- No adverse reactions or systemic adverse effects of timolol eyedrops
Strengths:
- Largest randomized clinical trial of acute migraine treatment with B-blocker eyedrops
- Eyedrops were in identical-looking containers with labels removed to maintain masking
- All patients included in the modified intention-to-treat analysis reported adherence to the protocol
- Accounted for crossover design to look for any carryover effect (There was no significant carryover effect due to crossover)
- The mean pain score at onset of attacks was similar between groups (6.01 for timolol vs 5.93 for placebo)
Limitations:
- Small, single-centered trial
- 24% loss to follow up or withdrawal of consent
- Only included patients with migraine who had a headache. There are subgroups of migraine where headache may not always be present
- Migraine attacks that started as an aura and did not progress to headache were excluded from the analysis
- The endpoint of 20 minutes may not have been long enough to identify any systemic adverse effects out to 2 to 4 hours
Discussion:
- Utility in the ED will be limited by the fact that this needs to be given very early in the process of migraine headaches, but could potentially be a discharge medication given to prevent future ED visits
- Authors discuss that oral B-blockers may not work for acute attacks due to high first-pass metabolism of the liver and the time taken to achieve peak plasma levels. Topically administered B-blockers overcome this first-pass metabolism and therefore may work for aborting acute migraine attacks
- Pharmacokinetic data of topically administered timolol shows peak plasma levels of 0.5ng/mL can be attained in 10 min with a decrease to 0.3ng/mL after 4 hours
- A single oral dose of 20mg of timolol attains peak plasma level of 50 to 103 ng/mL at 1 to 2 hours after oral administration. Detectable levels of oral timolol can occur in 30 30 minutes with a mean plasma half-life of about 4 hours
Author Conclusion: “This randomized crossover trial supports consideration of timolol eyedrops in the acute treatment of migraine. Further research is warranted to determine if the improvements observed are sustained for a longer follow-up and with larger groups.”
Clinical Take Home Point: Topical 0.5% timolol maleate eyedrops is not ready for primetime in the acute treatment of migraine headaches, but this study is another step forward in potentially adding another medication to the other abortive treatment options available.
References:
- Kurian A et al. Short-Term Efficacy and Safety of Topical B-Blockers (Timolol Maleate Ophthalmic Solution, 0.5%) in Acute Migraine: A Randomized Crossover Trial. JAMA Ophthalmol 2020. PMID: 33001159
- Goadsby PJ et al. Migraine – Current Understanding and Treatment. NEJM 2002. PMID: 11807151
- Andersson KE et al. Beta-Adrenoceptor Blockers and Calcium Antagonists in the Prophylaxis and Treatment of Migraine. Drugs 1990. [Link is HERE]
- Cossack M et al. Timolol Eyedrops in the treatment of Acute Migraine Attacks: A Randomized Crossover Study. JAMA Neurol 2018. PMID: 29799915
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)


The post New and Interesting: Timolol Eyedrops to Treat Migraine Headaches appeared first on REBEL EM - Emergency Medicine Blog.