
 From Oct 6th – 8th, 2020, Haney Mallemat (@CriticalCareNow) and his team put on an absolutely amazing online critical care conference called ResusX Rewired. ResusX is a conference designed by resuscitationists to provide clinicians with the most up to date skills and knowledge to help make a difference in your patients’ lives. Haney and his crew made a combination of short-format, high-yield lectures, and completely customizable small group sessions with procedural demos seem easy. There were so many high-quality speakers and pearls that I learned from this conference that I wanted to archive them here in one post for reference and to share with our readers/followers.
From Oct 6th – 8th, 2020, Haney Mallemat (@CriticalCareNow) and his team put on an absolutely amazing online critical care conference called ResusX Rewired. ResusX is a conference designed by resuscitationists to provide clinicians with the most up to date skills and knowledge to help make a difference in your patients’ lives. Haney and his crew made a combination of short-format, high-yield lectures, and completely customizable small group sessions with procedural demos seem easy. There were so many high-quality speakers and pearls that I learned from this conference that I wanted to archive them here in one post for reference and to share with our readers/followers.
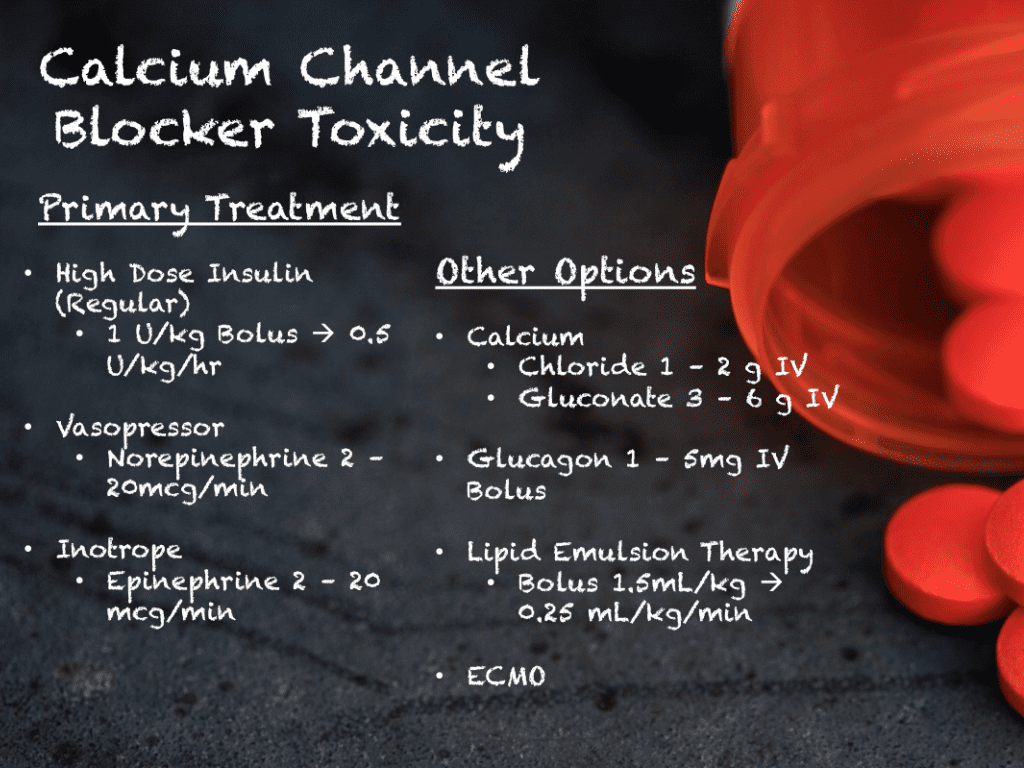
Treatment of Calcium Channel Blocker Toxicity
- High Dose Insulin (1U/kg bolus –> 1 to 10 U/kg/hr) + D10 at 0.25g/kg/hr
- Norepinephrine 2 to 20 mcg/min
- Epinephrine 2 to 20mcg/min
- CaCl 1 to 2g IV over 3min OR CaGluc 3 – 6g over 10min
- Glucagon 5mg IV
- 20% Lipid Emulsion Therapy (1.5mL/kg bolus –> 0.25mL/kg/min)
- ECMO
DKA Management via @SaraCrager
- It’s not about the sugar, it’s about the ketoacidosis
- Find the driver of the DKA (i.e. physiologic stressors)
- Normal glucose can still be DKA (i.e. euglycemic DKA)
- Normal bicarbonate + Normal pH can still be DKA (i.e. profuse vomiting)
- Intubation is a bad idea in DKA (RSI = Apnea = Worsening Acidosis = Potential Cardiac Arrest)
- Think BiPAP instead (give anti-emetics ahead of time
- Follow and replete K+
- Follow and replete Mg2+
- Bicarbonate fixes acidemia transiently and should not be routinely used
- Restore intravascular volume with balanced crystalloids
- REBEL EM Post: DKA Myths
- REBEL EM Post: Euglycemic DKA – It’s Not a Myth
Elevated Intracranial Pressure in Severe TBI via @4shikaJain
- Hypertonic Saline > Mannitol
- Mannitol
- Bolus Only
- Onset 30min
- Lasts 6hrs
- Causes Osmotic Diuresis
- Dose 0.25 – 2g/kg over 30 to 60min
- HTS (3%)
- Bolus or Drip
- Onset 5min
- Lasts 12hrs
- No Diuretic Effect
- Dose 300mL over 1hr
The Crashing Asthmatic via @EMSwami
- If usual care not working consider…
- Mg2+ 2g IV over 15min in 1st hour, then 2g IV/hr
- Epinephrine 5 to 10 mcg IVP then infusion at 1 to 20mcg/min
- Also consider Ketamine 0.3mg/kg bolus over 15min then 0.05 to 0.4mg/kghr
- REBEL Cast Ep11: The Crashing Asthmatic
TXA for Everything that Bleeds, an Update from 2019
- ICH (CRASH-3 + Pre-Hospital Study)
- No benefit in severe TBI (GCS ≤8)
- +/- benefit in moderate TBI (GCS 9 to 12)
- No benefit in mild TBI (GCS 13 to 15)
- GIB (HALT-IT)
- Exact timing of GIB hard to know
- No benefit + potential harms
- REBEL EM Post: CRASH-3 – TXA for ICH?
- REBEL EM Post: Out-of-Hospital TXA for TBI
- REBEL Cast Ep85: The HALT-IT Trial – TXA in Acute GI Bleeds
CRASH-3: GCS 9 – 12 with Biggest Potential Benefit
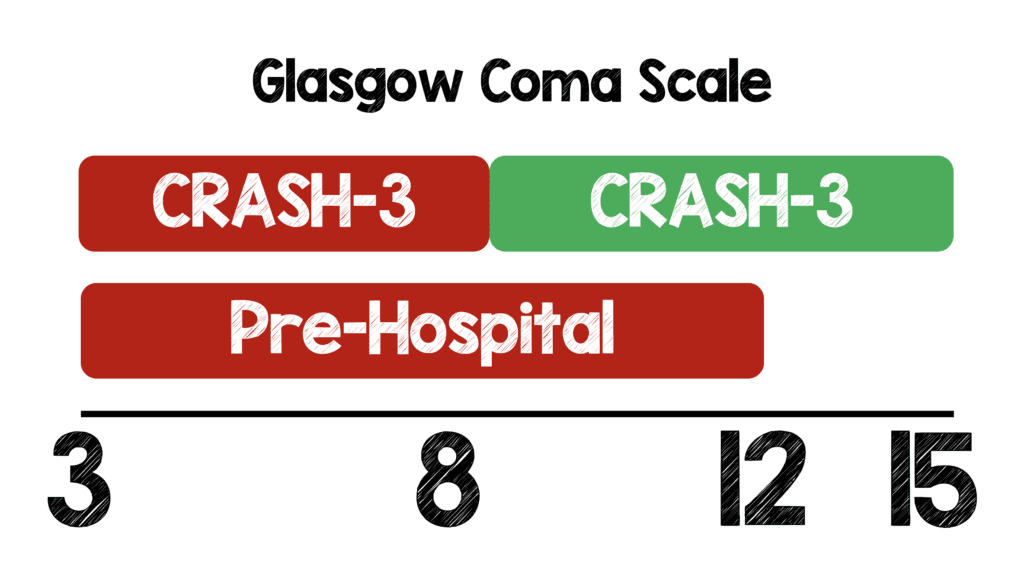
CRASH-3 found a potential benefit in intermediate severity GCS, but pre-hospital study did not divide up patients
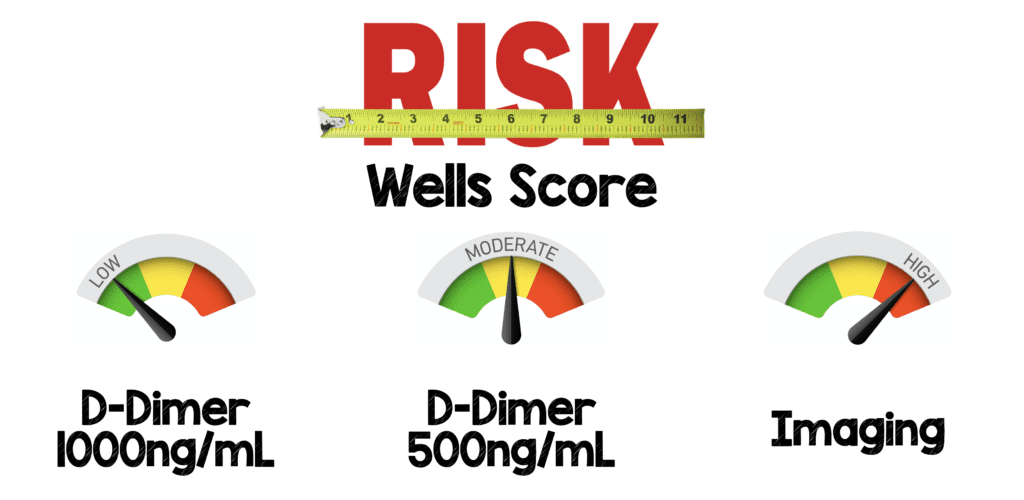
Clinical Probability Adjusted D-Dimer
- Acceptable miss rate = 1.8%
- YEARS trial missed 0.6% VTE at 90d and 0.2% death
- PEGeD trial missed 0% of VTE
- Both trials reduced ed imaging by 13 to 18%)
- Excluded cancer and pregnant pts
- Clinical adjusted d-dimer is ready for primetime
- REBEL EM Post: The YEARS Study – Simplified Diagnostic Approach to PE
- REBEL EM Post: PEGeD Study – Is it Safe to Adjust the D-Dimer Threshold for Clinical Probability?
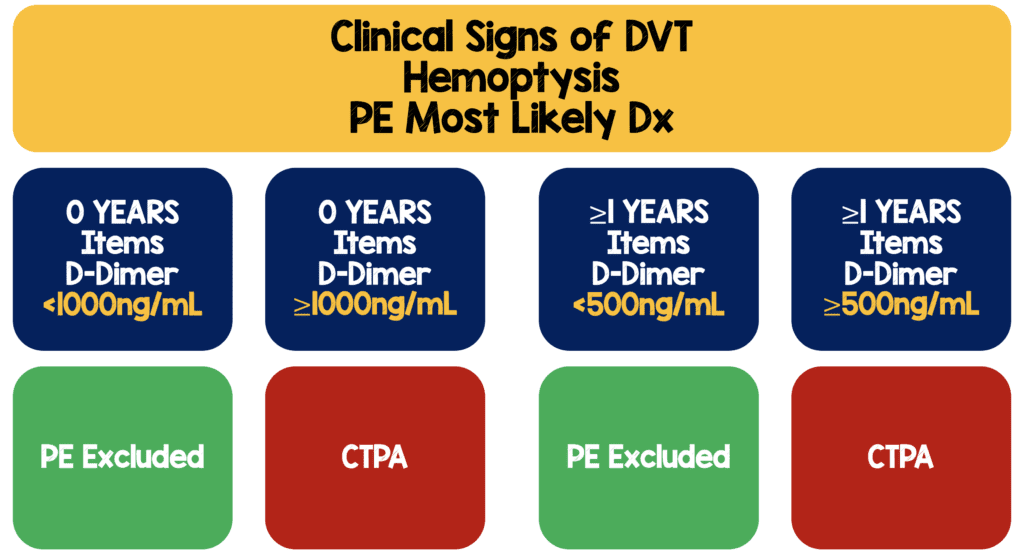
YEARS Protocol
PEGeD Protocol
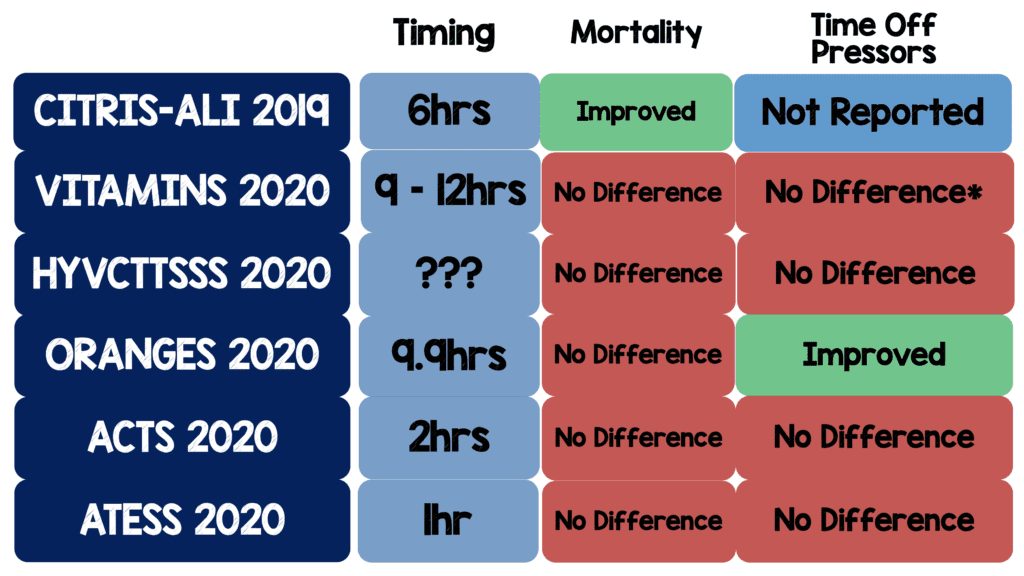
Metabolic Cocktail in Septic Shock…Maybe Not
- 5/6 RCTs with a negative primary outcome (ORANGES changed primary outcome after data collected)
- Arbitrary start point of ED arrival does not make sense as a stopwatch in a heterogenous disease that develops over time
- 5/6 RCTs showed no difference in mortality
- 5/6 RCTs showed no difference in time of pressors
- 5/5 RCTS have shown steroids alone decrease time off pressors
- REBEL Cast Ep74: Is it all About the VITAMINS in Sepsis?
- REBEL EM Post: Let’s get our ACTS Together – The Metabolic Cocktail and Septic Shock Again
- REBEL EM Post: CITRIS-ALI – Vitamin C in Patients with Sepsis and Severe Acute Respiratory Failure
- REBEL EM Post: The HYVCTTSSS Trial – The “Metabolic Cocktail” in Another RCT
- REBEL EM Post: The ORANGES Trial – Why You Can’t Just Read the Abstract
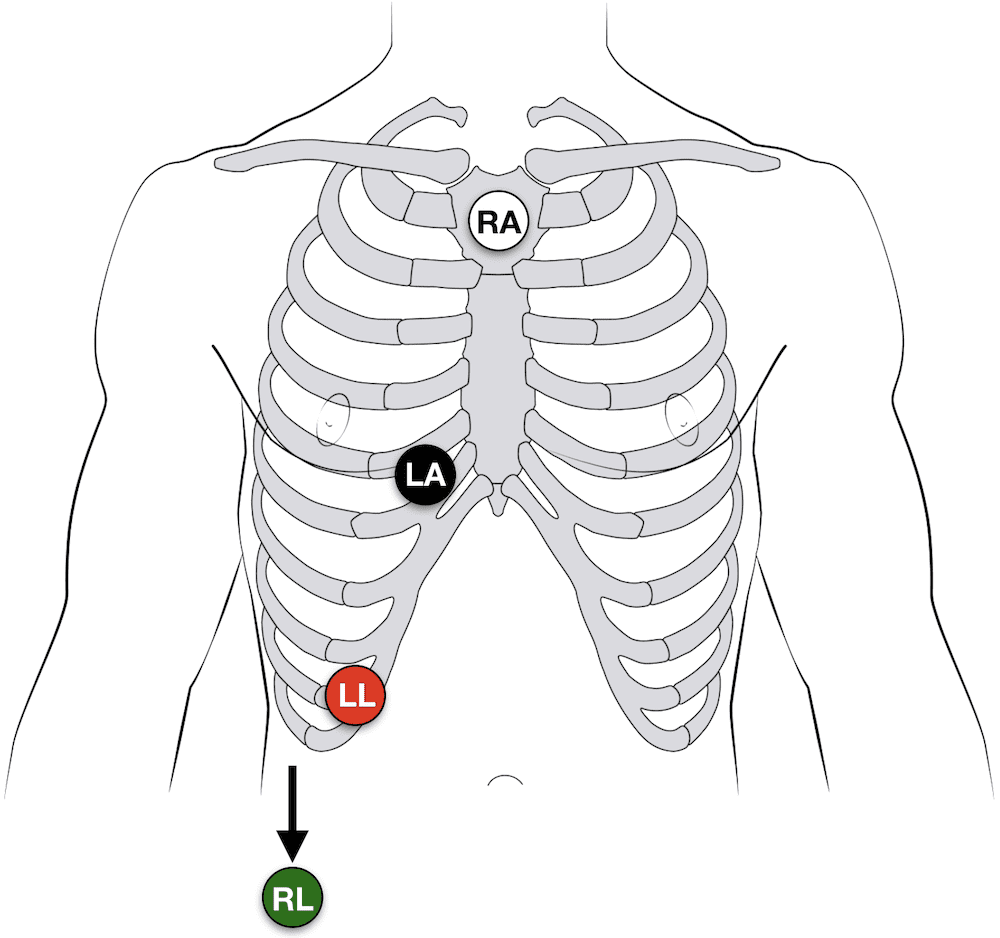
The Magical Lewis Lead to Differentiate SVT-AC vs VT via @amalmattu
- Lewis lead shows atrial activity
- RA –> Suprasternal notch
- LA –> Rt 5th ICS next to sternum
- LL –> Rt lower costal margin
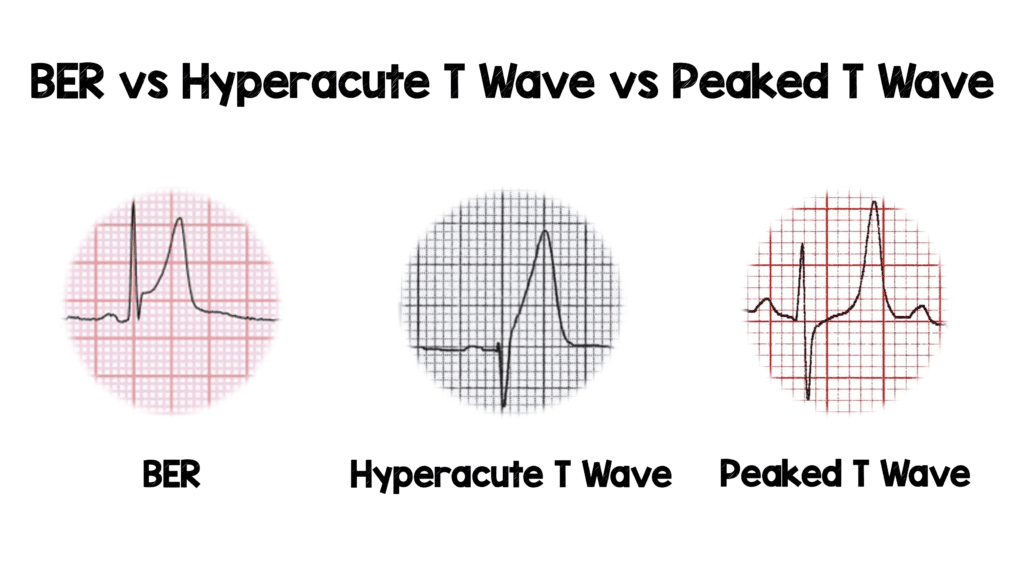
Terrible T’s of ACS via @amalmattu
- “The T wave is the underdog of ECGs”
-
Hyperacute T waves = T wave out of proportion to QRS
- Concerting for Occlusion MI
- Repeat ECGs
- New upright T wave in V1
- T wave in V1 bigger than T wave in V6
- Type of hyper acute T wave
- Get Serial ECGs
- Normal Variants = Misplaced leads, LBBB, LVH
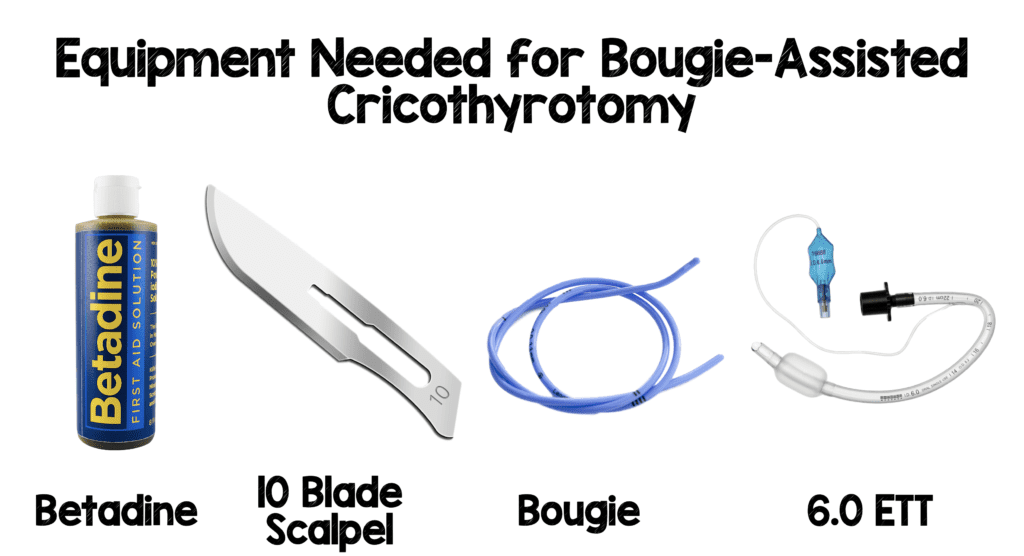
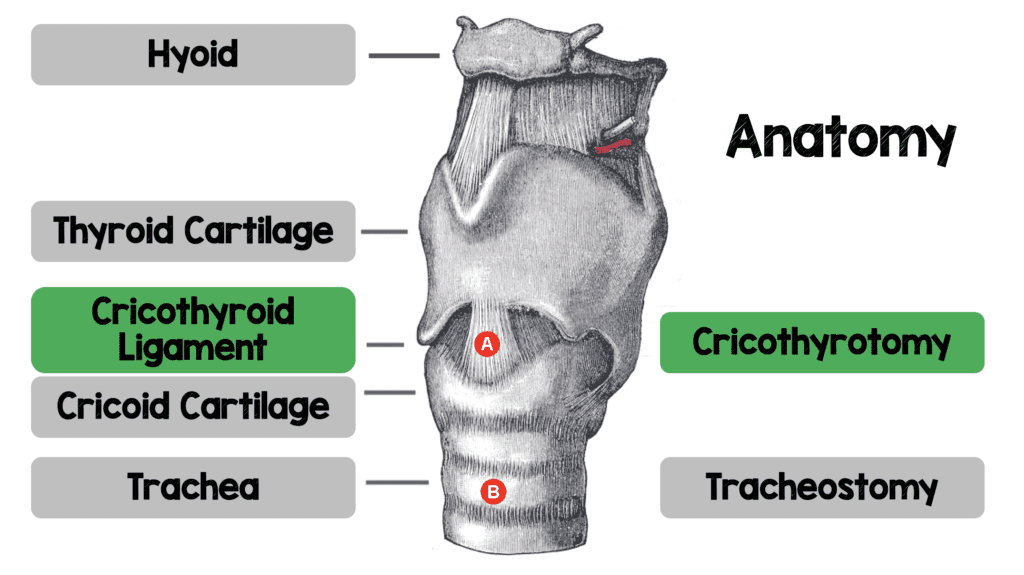
Bougie-Assisted Cricothyrotomy
- Simple and rapid
- No special equipment required
- High success and low complication rates
- Toughest part of procedure is decision to cut
- Know your anatomy
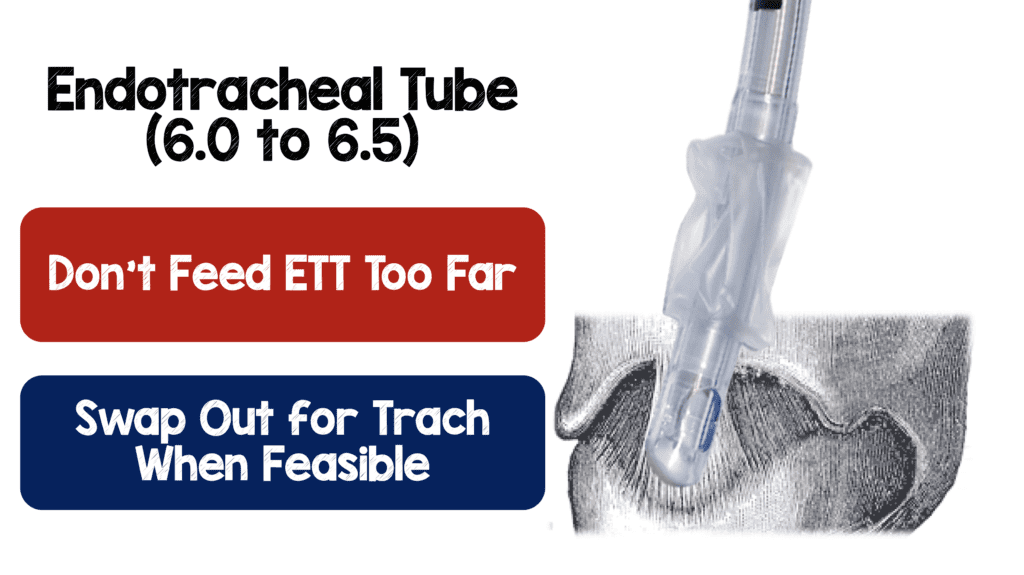
- Only need your finger, 10 blade scalpel, bougie, and a 6-0 ETT
- Betadine nice if available
- Don’t feed ETT too far (usually 1 to 2 cm after ETT ballon disappears)
- Practice, practice, practice

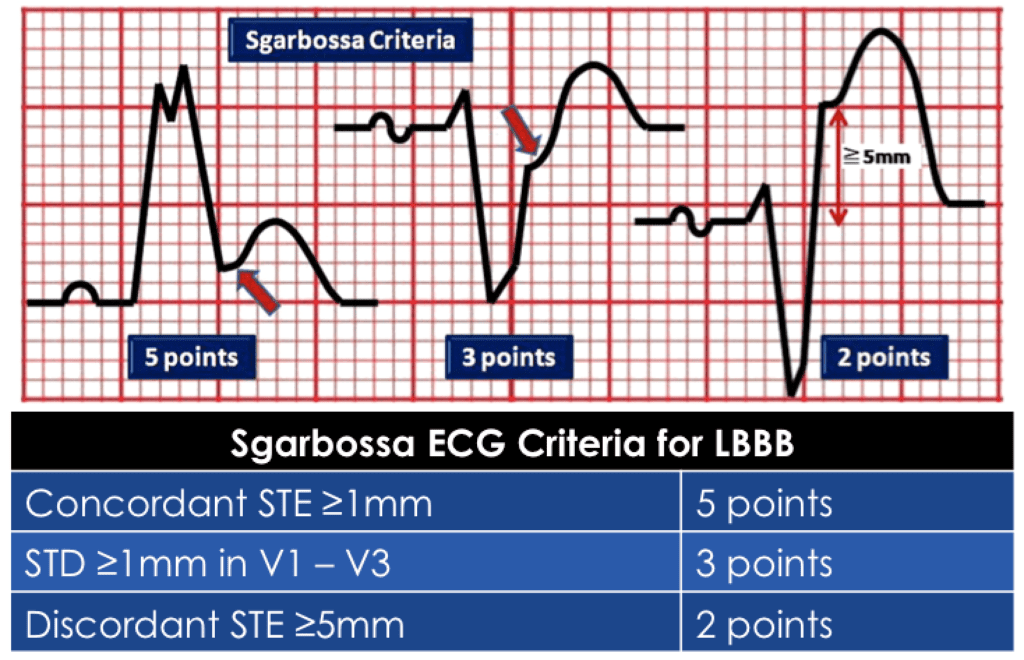
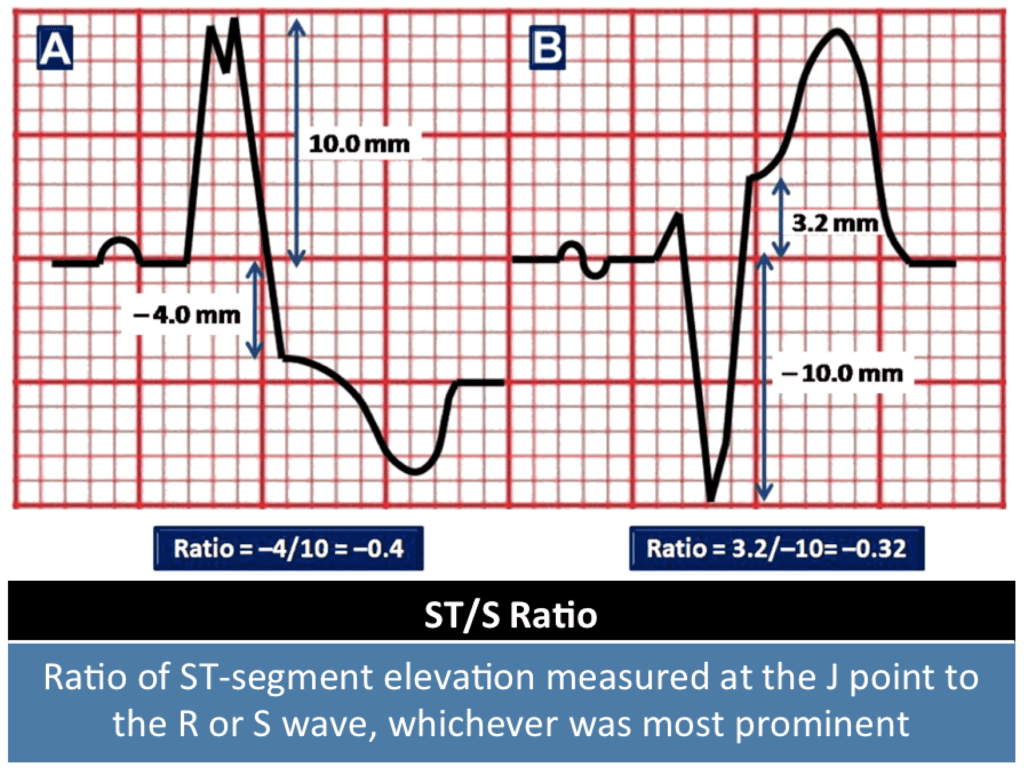
ACS in Presence of LBBB via @amalmattu
- Modified Sgarbossa Criteria (Only need in 1 lead)
- Concordant STE ≥1mm
- Concordant STD >1mm in V1 to V3
- ST/S Ratio ≤-0.25
- REBEL EM Post: Modified Sgarbossa Criteria – Ready for Primetime?
- REBEL EM Post: The Modified Sgarbossa Criteria – Part Deux
![]()
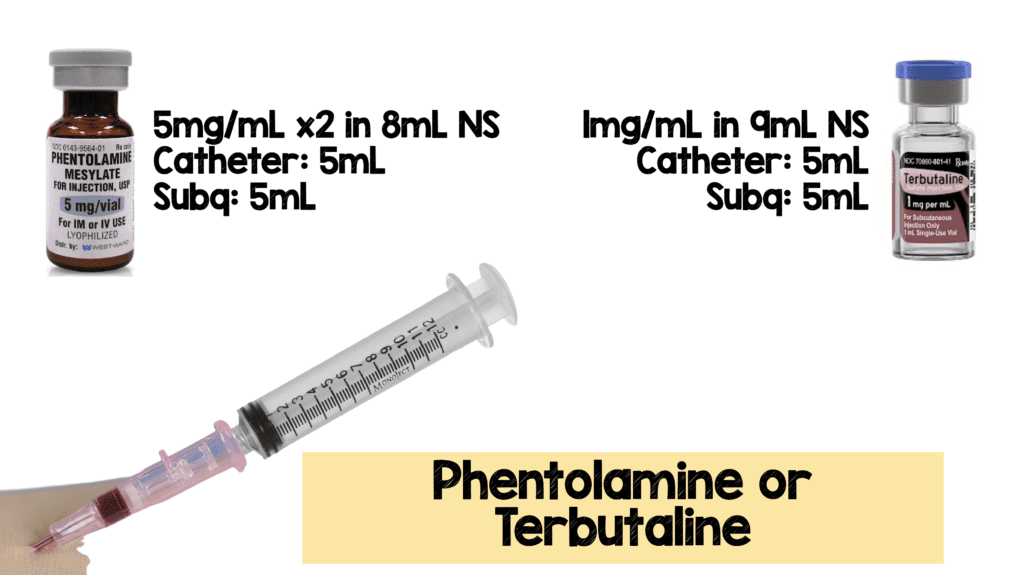
Peripheral Pressors: 6 Pearls to Not F*#k up the Arm
- Use proximal veins
- Use a longer catheter (4.78cm or 6.35cm)
- Run for only 2 to 4 hours
- Dilute + small volume (i.e. norepinephrine 4mg in 250mL NS)
- Have an observation protocol (Look at IV site every 15 to 20min)
- Have an extravasation protocol (Phentolamine, terbutaline, Nitropaste, warm compress, and elevation)
- REBEL EM Blog Post: Peripheral Pressors – 6 Pearls to Not F*#k up the Arm
VExUS Score to Quantify Systemic Congestion via @EMNerd_
- POCUS
- IVC
- Hepatic Vein
- Portal Vein
- Intra-Renal Vein
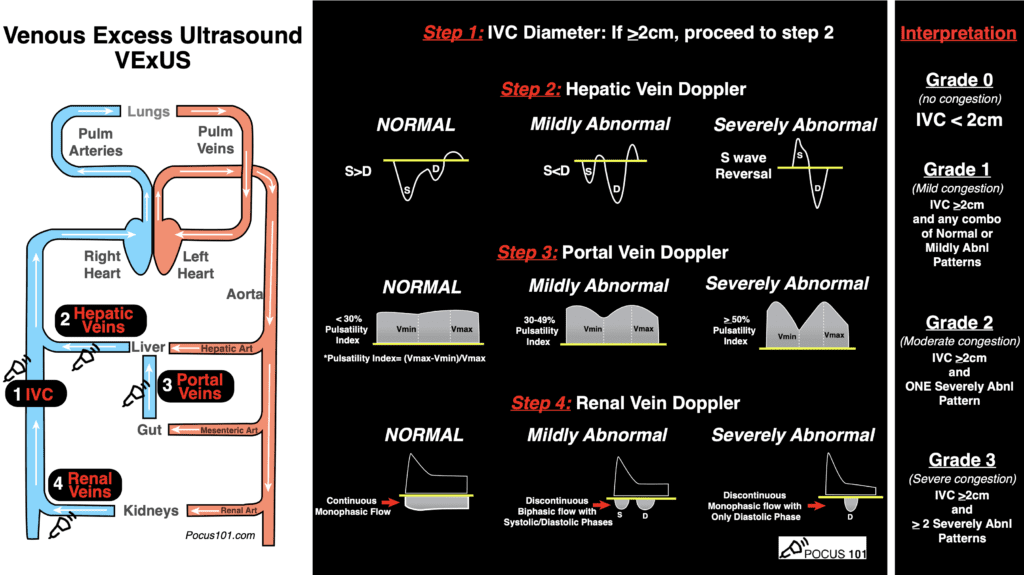
Image from POCUS101.com [Link is HERE]
The post Pearls from ResusX Rewired 2020 appeared first on REBEL EM - Emergency Medicine Blog.