
 The 1stannual Rebellion in EM Clinical Conference took place in San Antonio, TX on May 11th– 13th, 2018. If you missed out in 2018, the Rebellion is coming back June 28th – 30th, 2019. Stay up to date as we plan the conference for this upcoming year at www.rebellioninem.com.
The 1stannual Rebellion in EM Clinical Conference took place in San Antonio, TX on May 11th– 13th, 2018. If you missed out in 2018, the Rebellion is coming back June 28th – 30th, 2019. Stay up to date as we plan the conference for this upcoming year at www.rebellioninem.com.
The Missions of Rebellion in EM:
- Decrease Knowledge Translation: With 100s of journals and thousands of publications every year, it takes time for research to disseminate to clinical practice. Discussion of current literature and its application to practice is the key to facilitating safe best practices.
- Create a Community of Practice: It requires many to take care of the few. Patient care is a team sport that starts pre-hospital, continues through the ED, and finally into the hospital.
- Improve Patient Care: Decrease suffering and improve patient oriented outcomes
“Learning is always rebellion…every bit of new truth discovered is revolutionary to what was believed before.” -Margaret lee Runbeck-
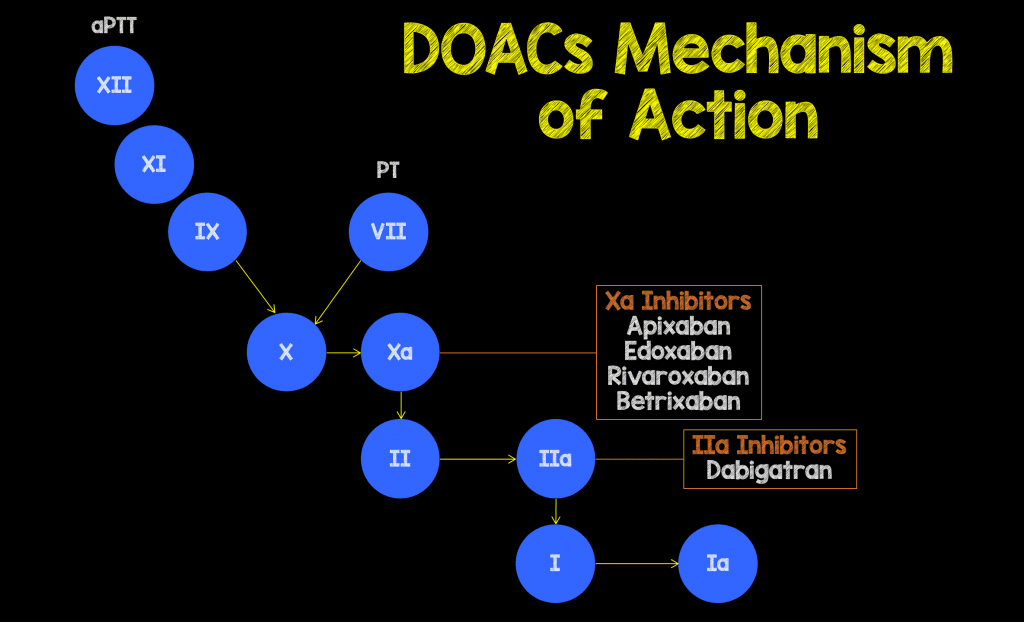
This talk was recorded live on the first day of Rebellion in EM 2018 in San Antonio, TX. The title of the talk, “Are you Going to do Something or Just Stand There and Bleed,” by Scott Wieters, MD (@EMedCoach). In this talk Scott discusses direct oral anticoagulant agents (DOAC), how to measure their activity, and how to reverse them in a bleeding patient.
[embedyt] http://www.youtube.com/watch?v=9i7LDk0YKv0[/embedyt]
 Scott Wieters, MD
Scott Wieters, MD
Director of Undergraduate Medical Education
Texas A&M College of Medicine
Baylor Scott & White EM Residency Faculty
Belton, TX
Twitter: @EMedCoach

3 Questions to ask when Dealing with a Patient Bleeding from DOACs:
- When was the last time medication was taken?
- What is the half-life of the medication?
- What is the renal function? – Chronic kidney disease or acute kidney injury may make DOACs more potent
DOAC Activity is Hard to Measure:
-
PT/PTT/INR:
- If PT elevated, means you are at the 75thpercentile of active drug level; If PT normal, does not mean patient does not have active drug level, you could still be at 55thor 65thpercentile of active drug level
- If PTT elevated, means you are at the 75thpercentile of active drug level; If PTT normal, again, does not mean patient does not have active drug level, you could also still be at 55thor 65thpercentile of active drug level
- Ecarin Clotting Time – Not used routinely used; Gold standard for Dabigatran activity
- Anti-Xa Level – Must be calibrated for agent the patient is on (i.e. different for Apixaban, Edoxaban, Rivaroxaban, Betrixaban)
- Thromboelastogram (TEG) – In Vino Veritas –> In Wine is Truth –> TEG for Dummies
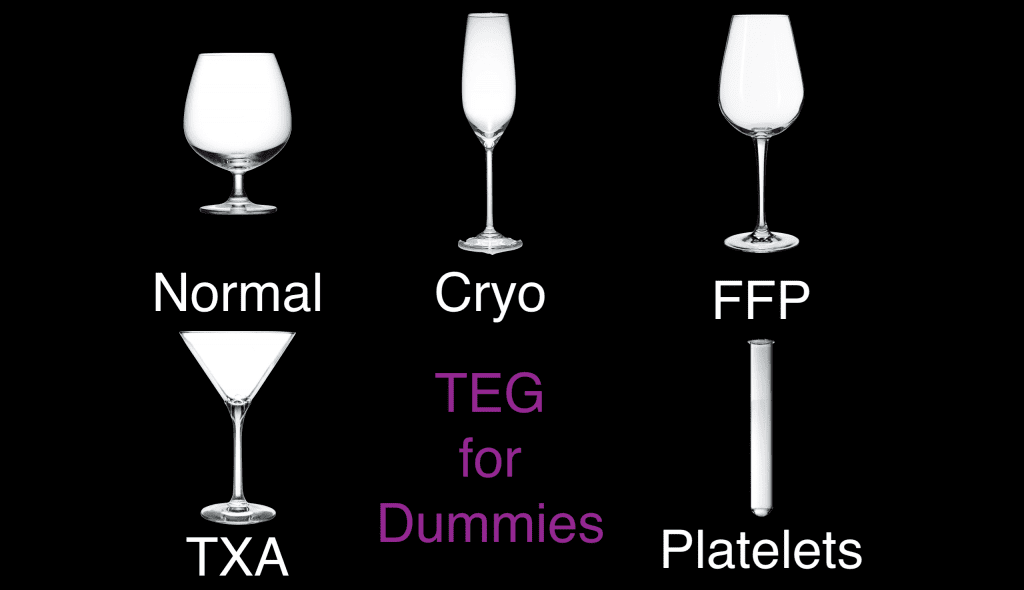
Shape of the TEG + Alcohol Glass = What is Needed:
- Brandy Tumbler = Normal (Do Nothing)
- Champagne Flute = Give Cryo
- Red Wine Glass = Give FFP
- Martini Glass = Give TXA
- Test Tube = Give Platelets
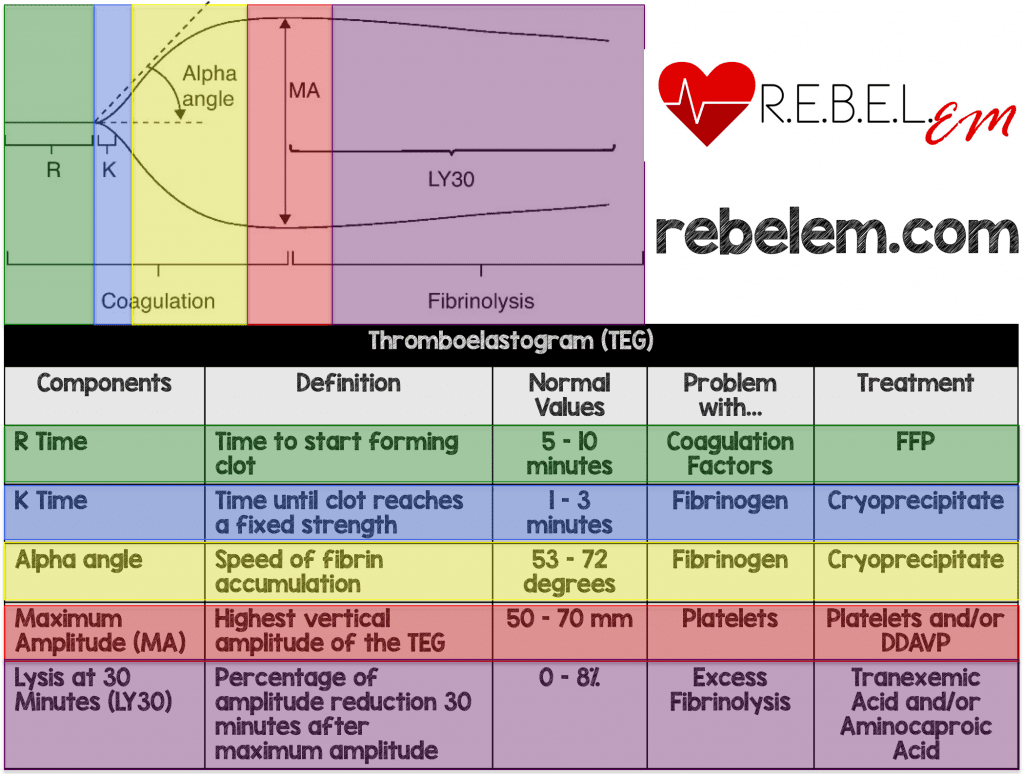
We have also created an infographic on REBEL EM to help simplify TEG Interpretation:
What Reversal Agents Were Discussed:
- Charcoal – Not giving this to patients who are actively bleeding
- Fresh Frozen Plasma (FFP) – It takes ≈30cc/kg to get to an INR of FFP (1.5 – 1.7); Can also cause transfusion reactions such as Transfusion Associated Circulatory Overload (TACO) or Transfusion Related Acute Lung Injury (TRALI)
- Dialysis – Requires large dialysis catheter and takes time to coordinate, so not helpful in acute setting of bleed
- Tranexamic Acid (TXA) – Plasminogen dissolves clot, but TXA inhibits plasminogen; Recommended by experts. Dose is 1g IV over 10 minutes + 1g IV over 8 hours
- Prothrombin Complex Concentrates (PCC) – 4 Factor (KCentra, Octaplex, Beriplex) contains factors II, VII, IX, X (Inactive factors); Also contain some protein C & S as well as heparin. Dose is typically 50U/kg up to 2,000U [1]
- Factor Eight Inhibitor Bypass Activity (FEIBA) – Contains factors IIa, VIIa, IXa, Xa (Active factors) therefore very pro-coagulant. Dose is typically 50U/kg IV x1 [2]
- Idarucizumab (Praxbind) – Humanized monoclonal antibody fragment that specifically and potently inhibits dabigatran. FDA approved October 2015. Evidence is poor including small studies, studies funded by same company that makes Dabigatran, and questionable patient oriented outcomes (reverses bleeding parameters). For now, this is the best we have. Dose is 5g IV x1 [5] [6]
- Andexanet Alpha – Derived from Chinese hamster ovary, is a decoy antigen that competitively binds to Xa inhibitors. Just approved by FDA in May 2018. [3] [4]
- Ciraparantag – Modified recombinant molecule that directly inhibits Xa and IIa; Not FDA approved at this time, but human studies are underway
Take Home Messages for DOAC Reversal:
- Xa Reversal Summary: 4 Factor PCC 50U/kg + TXA 1g IV –> Consider Andexanet Alpha when available –> In the Future Ciraparantag
- IIa Reversal Summary: Idarucizumab 5g IV + TXA 1g –> If no Idarucizumab available, consider FEIBA 50U/kg –> In the Future Ciraparantag
Also Be Sure to Checkout our YouTube Channel

References:
- Majeed A et al. Management of Rivaroxaban- or Apixaban-Associated Major Bleeding with Prothrombin Complex concentrates: A Cohort Study. Blood 2017. PMID: 28835439
- Mao G et al. Factor Eight Inhibitor Bypassing agent (FEIBA) for Reversal of Target-Specific Oral Anticoagulants in Life-threatening Intracranial Bleeding. J Emerg Med 2017. PMID: 28007364
- Siegal DM et al. Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. NEJM 2015. PMID: 26559317
- Connolly SJ et al. Andexanet Alfa for Acute Major Bleeding Associated with Factor Xa Inhibitors. NEJM 2016. PMID: 27573206
- Glund S et al. Safety, Tolerability, and Efficacy of Idarucizumab for the Reversal of the Anticoagulant Effect of Dabigatran in Healthy Male Volunteers: A Randomised, Placebo-Controlled, Double-Blind Phase 1 Trial. Lancet 2015. PMID: 26088268
- Pollack CV Jr et al. Idarucizumab for Dabigatran Reversal – Full Cohort Analysis. NEJM 2017. PMID: 28693366
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami) and Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Rebellion in EM 2018 – DOAC Reversal by Scott Wieters, MD appeared first on REBEL EM - Emergency Medicine Blog.