
This past  week, one hundred clinicians went back to work inspired. They were reinvigorated, motivated and full of knowledge. They were the delegates, faculty and volunteers of #resusTO. This inaugural event (hopefully) laid the groundwork for many more to come as it was a success by any measure.
week, one hundred clinicians went back to work inspired. They were reinvigorated, motivated and full of knowledge. They were the delegates, faculty and volunteers of #resusTO. This inaugural event (hopefully) laid the groundwork for many more to come as it was a success by any measure.
ResusTO, the brain child of human factors guru and EM doc Chris Hicks, who along with the organizing committee of Andrew Petrosoniak, Jesse Spurr and Kari White, and a plethora of volunteers, orchestrated a human performance, education and simulation extravaganza! The conference held in Toronto, Canada sept 13th– 14th, 2018, was a special conference for so many reasons and you could feel it the moment you stepped up to the registration desk and received your name tag that noted, “Awesome human delegate.”

ResusTO: A Simulation/Resuscitation Conference Like No Other
#resusTO | Sept 13th– 14th, 2018
See. Do. Discuss. Master. was the theme of ResusTO, setting the stage for a fast paced and interactive two days. Smashing hierarchies and modeling the benefits of team based education and training wasn’t a stated goal, but rather an undertone, felt loudly by delegates from a variety of different disciplines; EM, Crit Care, Anesthesia, OB-GYN, docs, nurses, paramedics, respiratory therapists and medical students. The multidisciplinary approach was just the beginning, there were so many key lessons and messages that came up from this conference that in no way would a single blog post do them all justice but we will do our best.

Day One Morning Panel Discussion with (from left): Scott Weingart, Vic Brazil, Jesse Spurr, Patricia Trbovich, Andrew Petrosoniak and Chris Nickson
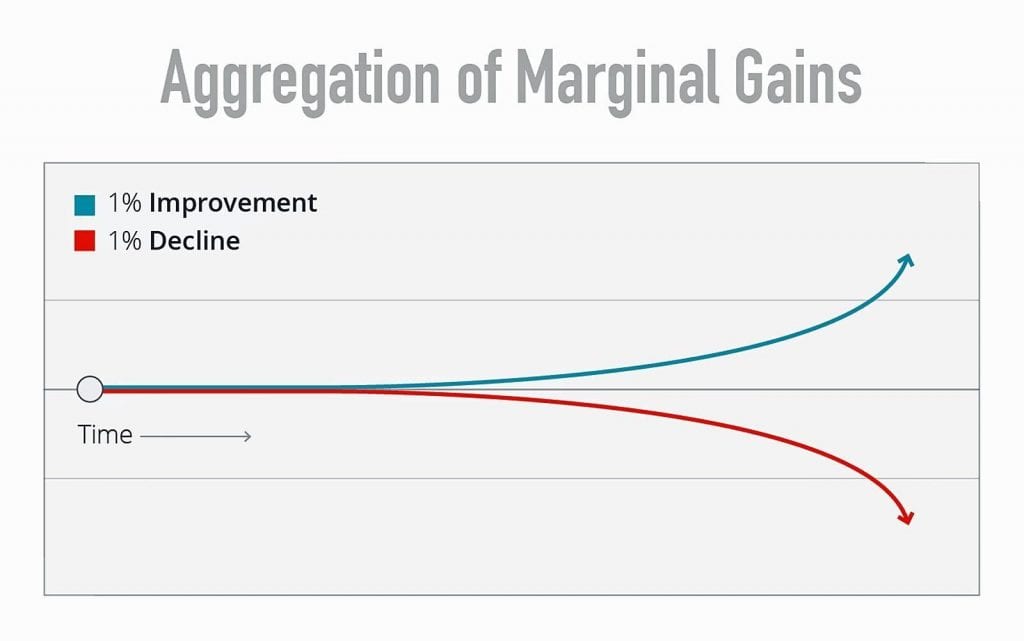
Aggregation of Marginal Gains by Vic Brazil and Jess Spurr
The sounds of ventilator alarms bounced annoyingly in the air against our not yet caffeinated brains and Vic posed the question: “what is right and what is wrong with your resuscitation teams?” A big question to begin the morning but culminated in a discussion surrounding leadership, followership and societal structures. The focus of which was the best interest of the patient and how we can become the team that patient needs.
Small incremental improvements or deteriorations in any process can add up over time to a significant improvement or decline when they are all added together. Having a commitment to improve the team, even if just 1% at a time can have a significant impact.
“Good team behaviors lead to good patient outcomes”- Vic Brazil
Resuscitative Hysterotomy by Sara Gray
This procedure should no longer be called perimortem c-section, as it is potentially lifesaving for mom. A better term would be resuscitative hysterotomy. The way this procedure helps mother is by relieving caval compression, improving pulmonary mechanics, and reducing oxygen demand (i.e. by removing baby/placenta). Based on case reports and series maternal survival benefit is about 32% and fetus survival is about 50%. Sara points out that the 4 minute rule for performing this procedure has no data to support it! There have been good survival outcomes for mom out to 15 minutes and for baby out to 30 minutes. These can be considered the outer limits for survival, based on best available evidence. The only things required for this procedure include: 10 blade scalpel, scissors, and two forcep clamps. Finally, the procedure itself is not as difficult as making the decision to do the procedure so start early and mentally prepare your team.
Resuscitation Economics by Andrew Petrosoniak & Patricia Trbovich
This was an interesting topic that I had not ever considered. Economics is defined as the study of how societies use scarce resources to produce valuable commodities and distribute them among different people. Resuscitation economics is the study of how teams use scarce resources to produce valuable patient care. One key concept that was discussed here was that we often try to change people’s behavior, however changing the system may be more beneficial (i.e. nudging behavior). Nudging behavior involves changing something in the system making people choose the easy thing to do without having to nudge them too much. Therefore, by changing the system, the best decision can be made the easiest to make. Two other concepts that came up during this session included the particular costs of running a resuscitation:
- Opportunity Cost: The idea that once you spend your time on something then you can’t spend it on something else
- Friction Cost: Small barriers that can prevent us from doing something
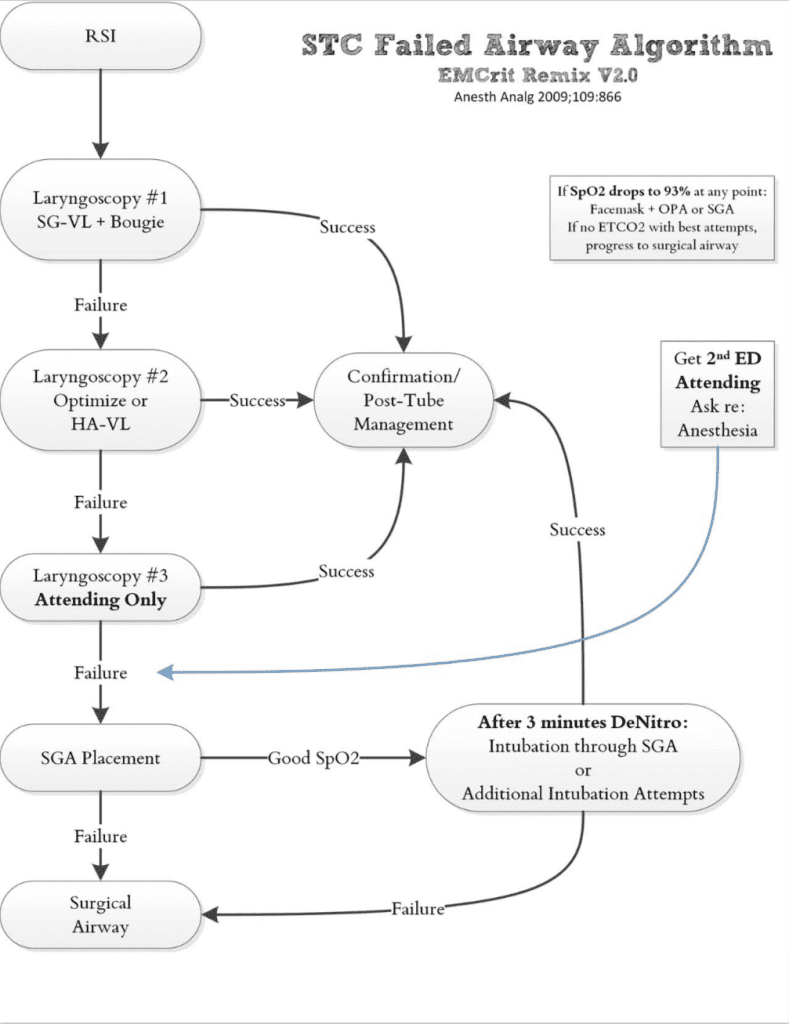
Critical Airway Mindset and Management (CRAMM) by Scott Weingart
In only the way that Scott Weingart can, he told us that “we suck at airway, but it’s not our fault”. This was an amazing session on the current paradigm in airway management. Most of our skills were learned from techniques of anesthesiology, however our environment and patients are different than anesthesiology. A key example is the concept of first pass success, as we know that a second, third, or fourth attempt has higher mortality rates associated with it. The current optimal airway model looks like the following:
- 1stAttempt: Standard Geometry Video Laryngoscopy + Bougie
- 2ndAttempt: Hyperangulated Geometery Video Laryngoscopy + Stylet
- 3rdAttempt: Most experienced person in the room
- 4thAttempt: Supraglottic Airway Device
- 5thAttempt: Surgical Airway
Other key things to consider in airway management:
- If you are going to use rocuronium for your paralytic, it lasts almost 50 minutes, so don’t forget to start sedation
- Preoxygenation should start with non-rebreather _ nasal cannula as this only uses one set of hands, but if saturation not ≥95%, change the non-rebreather to a bag valve mask with a PEEP valve to overcome potential physiologic respiratory shunt.
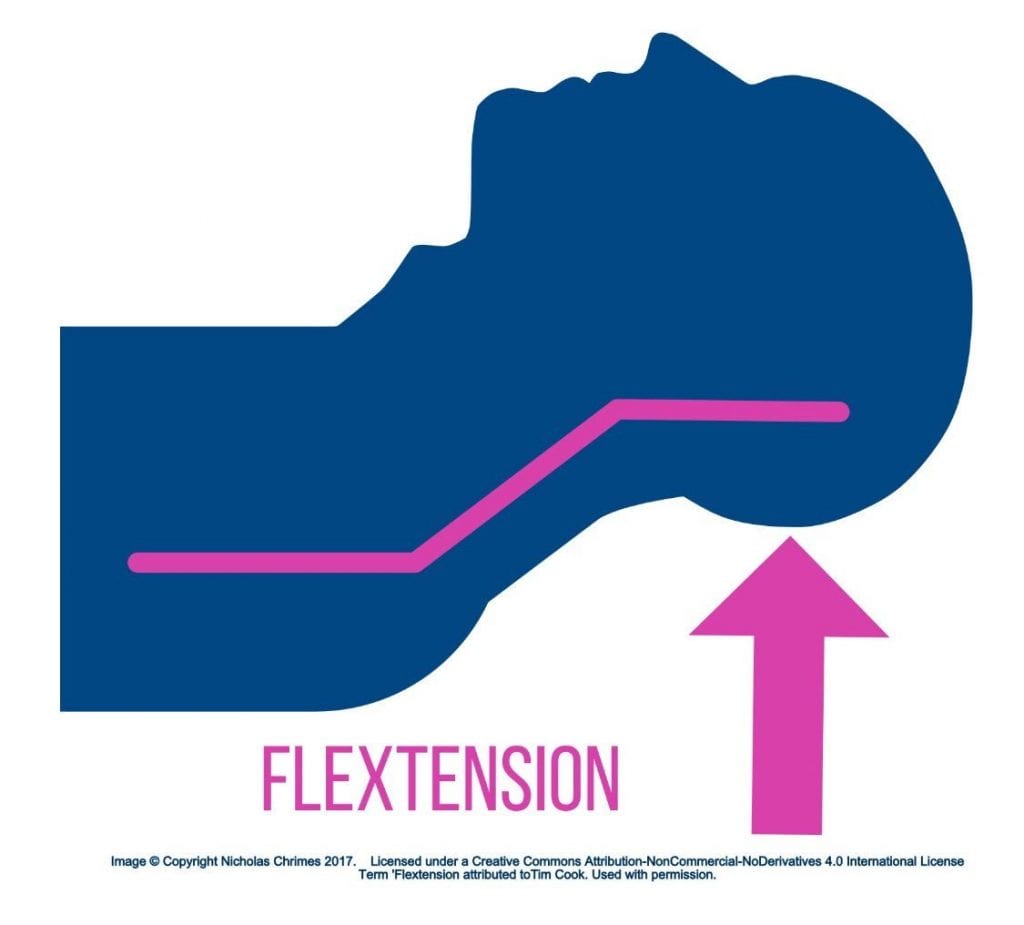
- The optimal position of the patient is “flextension,” which essentially means we want the ears above the level of the xiphoid
Also Checkout Scott’s Podcast HERE: EMCrit 233 – EMCrit Failed Airway Algorithm 2018 from resusTO
Simulation for Elite Performers by Chris Nickson
Developing expertise is a complicated matter and not as simple as many may think. It requires highly motivated learners that have focused repetitive practice with monitoring and feedback (i.e. deliberate practice). The mark of an expert is the layers of failure they have had to overcome (i.e. mental models to overcome failure). As people gain more experience and expertise, simulation also needs to be modified to increase the level of difficulty. It is important to remember that teams that come together all the time are very different than the teams that come together in the ED. Therefore strategies used for elite performance teams are hard to reproduce in our environment. This can be done in several ways:
- Signal to noise ratio – more noise for more experienced learners/teams
- Cognitive load – Fill up bandwidth with extrinsic load (i.e. environmental factors, background noise interpersonal stress)
- Changeperformance requirements – have the patient decompensate faster
- Use a confederate – individual other than the patient who is scripted in a simulation to provide realism, additional challenges, or additional information for the learner
After the Arrest by Sara Gray
Burnout and depression are on the rise in health care and above national averages. We need to plan for psychological well-being. One method of accomplishing this is the 3 D’s of debriefing: Deactivation (stressed to calm), Deconstruction (Analyzing the case), and Dissemination (Sharing and educating). Another method is finding someone in your life that you can talk to (i.e. failure friend). Self-care is another important modality which is an activity that brings you peace or joy. This can be exercise, reading, being outdoors, and/or meditation. We need to schedule time for this. Finally finding meaning in tough cases helps bring us to acceptance and with growth mindset can increase happiness and resilience.
Rapid Cycle Deliberate Practice by Alice Gray & Alia Dharamsi
This session started off by discussing how ACLS is broken. What a great way to grab everyone’s attention. Taking a two day course every 2 years does not make us a better resuscitationists. Looking upon learning theory and mastery of learning, repetition with deliberate practice is a better way to ensure we do not have a decay in our skills. With this method of learning a person would start with something simple like identifying pulselessness, then there would be a pause in the activity, followed by a debrief on this. After debrief, the cycle would start over with identifying pulselessness and then adding high quality CPR and so on. Each activity would serve as a prebrief for the next cycle and resuscitation skills can now be built block by block. Essentially this is taking a complex process and breaking into microskills (i.e. task chunking). This process can help overcome the “amygdala hijack,” aka “holy shit paralysis,” that can occur during a true resuscitation.
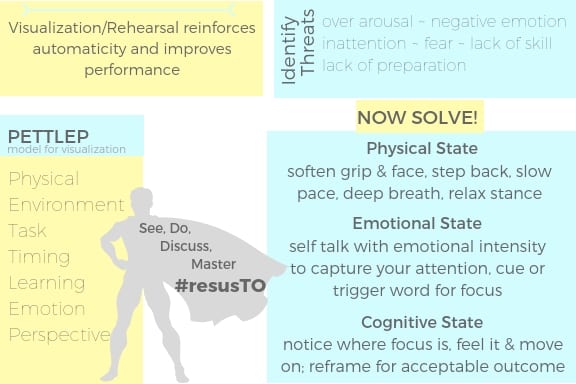
Resuscitate Like a Badass by Ashley Liebig
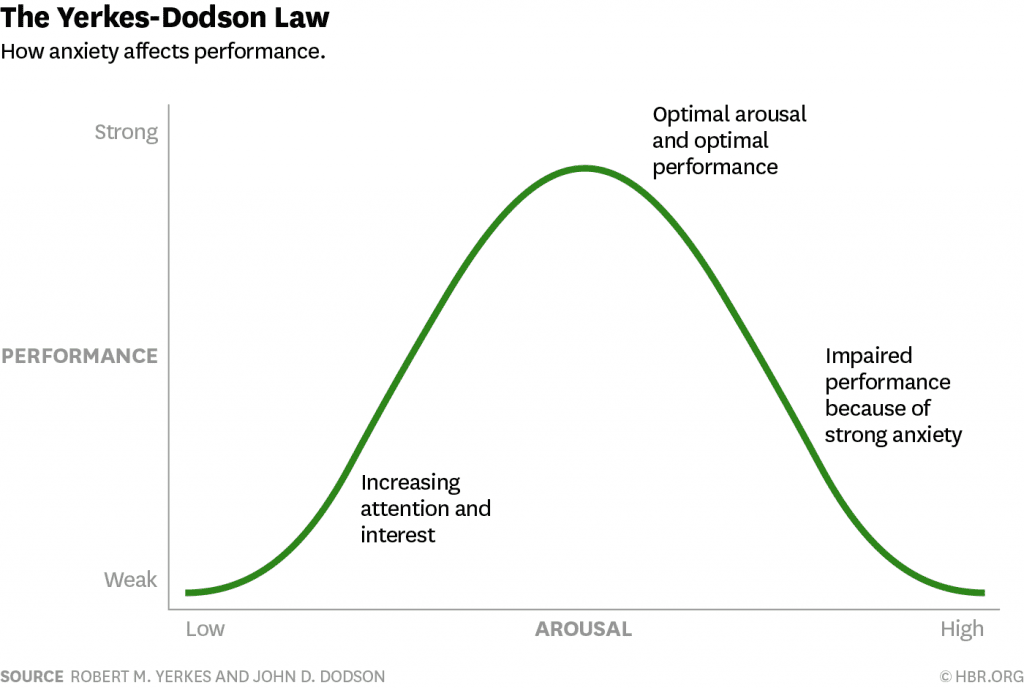
This session discussed ways to achieve an optimum performance state. Your environmental threat assessment can be adapted in a few ways so that stress or fear can be managed. Ashley suggests simply “we trick it, train in and love it.” Tricking the internal narrative involves cognitive reframing (reframe the situation where opportunities in tough situations can be found) and self-talk. “The narrative we continue to reinforce, influences how we perceive a threat or stress.” Training is just that, preparation leads to confidence, mental rehearsal leads to automaticity and focused attention. We also can’t forget that we love what we do, that it has meaning and purpose and with these ideas in tact we find an optimal performance state or “flow” that occurs when we accomplish something that is both challenging and meaningful.
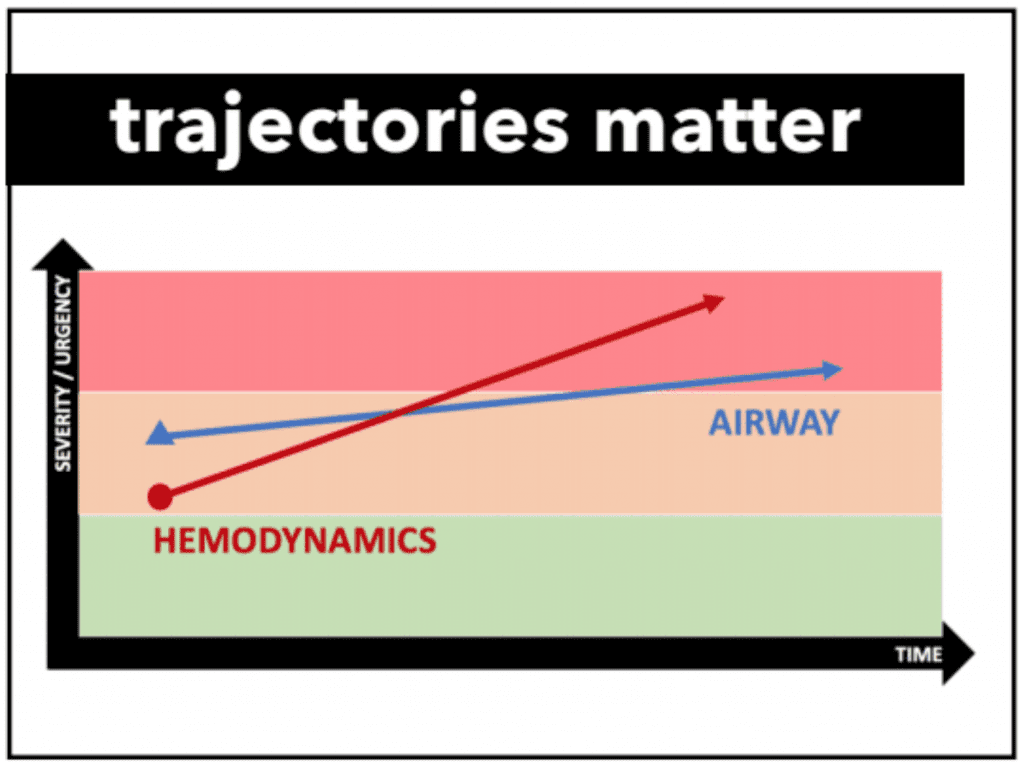
Trauma Resuscitation Resequenced by Andrew Petrosoniak & Chris Nickson
ATLS is a great training tool because it is structured and gives people a paradigm to follow. Unfortunately, patients are not all the same, therefore ABCs need to be dealt with in parallel not in sequential order. A better way would be to focus on physiologic threats instead of ABCs. Identify the greatest life threat and customize the resuscitation. One size does not fit all, and trajectories of physiology should be considered in deciding what to deal with first. In the image below, hemodynamics are on a faster trajectory than airway for increasing severity, therefore hemodynamics should be dealt with first before airway.
REBOA by Chris Hicks
The purpose of REBOA is to stop bleeding below the site of tamponade and increase perfusion above the site of tamponade (Essentially ED Thoracotomy 2.0). There are essentially 3 zones which include zone 1 for intra-abdominal hemorrhage, zone 2 which is a no fly zone for tamponade, and zone 3 which is used for pelvic hemorrhage. In this workshop we learned the steps to placing a REBOA catheter with a great mnemonic ME-FIIS:
- M = Measure – Zone 1 (insertion point to sternal notch); Zone 3 (insertion point to xiphoid)
- E = Empty – Empty the balloon
- F = Flush the catheter
- I = Insert the orange sheath to the introducer
- I = Inflate the balloon (2 – 8cc)
- S = Secure the line
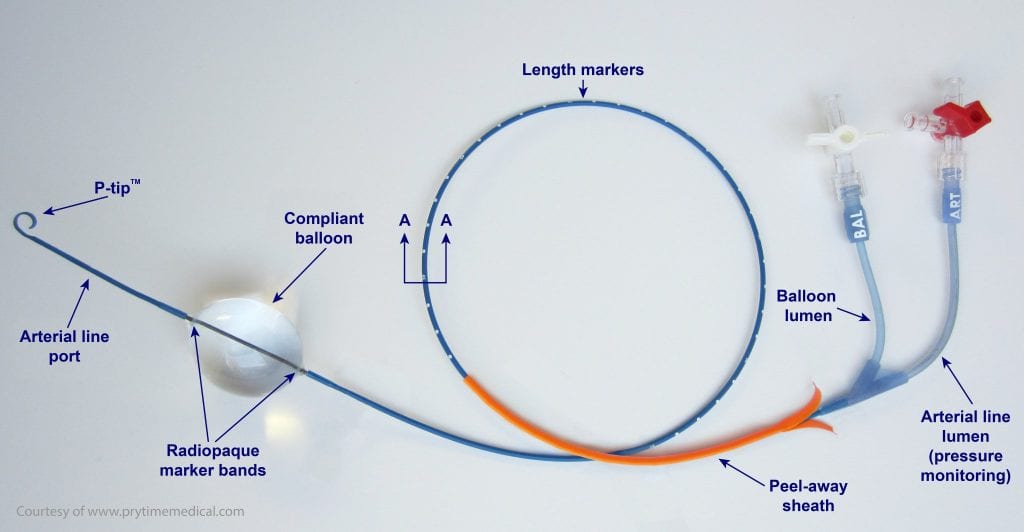
The maximum balloon time is not exactly known but in this workshop a time of 30 minutes was used as a conservative maximum. It is important to remember that this is just a temporizing measure.
And that’s a wrap! Two days of fast paced lectures, panel discussions and hands-on break-out workshop sessions. We obviously couldn’t be in all of them, though the word on the street is that all of the sessions were pretty epic! We would like to say Congratulations to the #resusTO team for their success. More than that, we would like to thank them for their innovation, leadership and commitment to patient care. This week, one hundred people looked after patients as a better version of themselves. Be proud of that!
Post Co-Written By: Ashley Liebig & Salim Rezaie
and
Co-Posted on St. Emlyn’s Blog
The post ResusTO: A Simulation/Resuscitation Conference Like No Other appeared first on REBEL EM - Emergency Medicine Blog.