
 Background: One of the most feared complications associated with rapid sequence intubation (RSI) is hypoxemia ultimately leading to cardiac arrest. The FELLOW Trial, a recent randomized controlled trial demonstrated no difference in hypoxemia rates between patients that received apneic oxygenation and those that did not (i.e. “usual practice”) in the ICU. What many forget about this trial is 1/3 of the patients were pre-oxygenated with a bag valve mask and another 1/3 of the patients with a BIPAP device, meaning that 2/3rds of these patients were not truly apneic during the period that induction medications were pushed up to laryngoscopy. Currently, there is a lack of high quality research on the use of apneic oxygenation in the ED setting. Many still use the intervention as it is cheap, easy to do, with no increase in patient harm, but there are still naysayers that do not feel the intervention is warranted in standard RSI practice.
Background: One of the most feared complications associated with rapid sequence intubation (RSI) is hypoxemia ultimately leading to cardiac arrest. The FELLOW Trial, a recent randomized controlled trial demonstrated no difference in hypoxemia rates between patients that received apneic oxygenation and those that did not (i.e. “usual practice”) in the ICU. What many forget about this trial is 1/3 of the patients were pre-oxygenated with a bag valve mask and another 1/3 of the patients with a BIPAP device, meaning that 2/3rds of these patients were not truly apneic during the period that induction medications were pushed up to laryngoscopy. Currently, there is a lack of high quality research on the use of apneic oxygenation in the ED setting. Many still use the intervention as it is cheap, easy to do, with no increase in patient harm, but there are still naysayers that do not feel the intervention is warranted in standard RSI practice.
What They Did:
- Randomized Controlled Trial in the ED Setting
- Single Institution
- Apneic Oxygenation vs Usual Care
Interventions/Definitions:
- Apneic Oxygenation: Oxygen via Nasal Cannula at flush flow rates ≥15LPM during laryngoscopy
- Usual Care: No supplemental oxygen during laryngoscopy
- Pre-Oxygenation: NRB, BiPAP, or BVM connected to flush flow rate with 100% oxygen
- Apnea Time: Time from first look (defined as insertion of the laryngoscope blade into the patients mouth) to confirmation of ETT placement by waveform capnography (EtCO2) or in failed intubations time to repeated assisted ventilation
Outcomes:
- Primary Outcome: Lowest Mean Oxygen Saturation during the apnea period or in the two minutes following intubation
- Secondary Outcomes: First Pass Success Rate, Time to Desaturation SpO2 <90% and <80%, Average Time to Desaturation, Mortality
Inclusion:
- All Patients > 18 Years of age, presenting to the ED, Requiring Intubation
Exclusion:
- Not Pre-Oxygenated to the Standard RSI Protocol of a Goal of 3 Minutes with 100% FiO2 y Means of BVM, BIPAP, and/or NRB
- Patients with Cardiac or Traumatic Arrest
- No Apneic Period (i.e. Awake Intubation)
Results:
- 206 patients enrolled and 200 patients randomized
- Apneic Oxygenation = 100
- Usual Care = 100
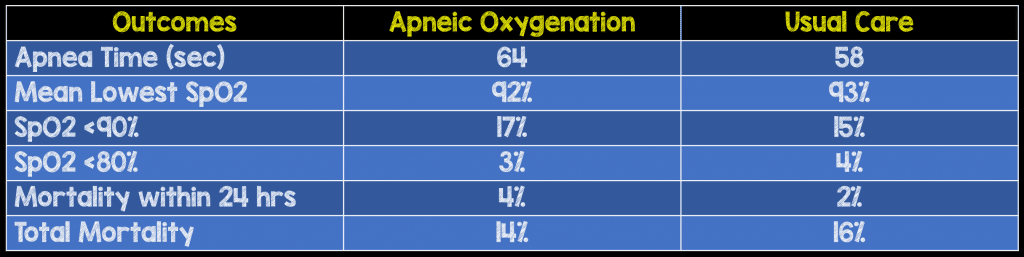
- Lowest Mean Oxygen Saturation
- Apneic Oxygenation: 92% (95% CI 91 – 93)
- Usual Care: 93% (95% CI 92 – 94)
- p = 0.11
- Critical Results:
Strengths:
- Randomized controlled trial
- Observers were blinded to study outcomes and not involved in the procedure of intubation
- Intubation checklist was used on all intubations
- Determination of accuracy of data collection was confirmed by comparing the data collected from the first 20 consecutively enrolled patients (10% of study population) with the primary investigators data
Limitations:
- Utilized a real-time data collection form which have been shown to underestimate adverse events and time to intubation
- Single center study at an academic ED with residents may make this non-generalizable to non-academic centers
Discussion:
- Over 70% of patients were successfully intubated by 60 seconds, 80% by 80 seconds, 90% by 100seconds, and 100% by 195 seconds
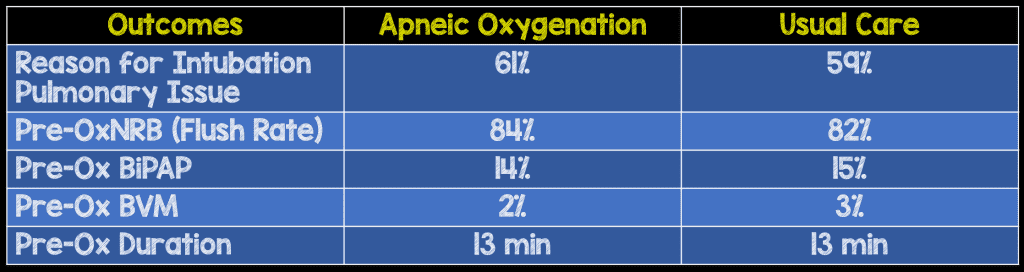
- About 60% of patients were intubated due to a pulmonary issue which was the most common indication for intubation in both cohorts
- All patients were pre-oxygenated for 3 minutes with flush 100% O2 prior to intubation and the majority of patients were successfully intubated by 60 seconds. Its no surprise that no difference was found between the two groups and does not mean apneic oxygenation does not work, especially in patients with prolonged apnea times or requiring crash intubations.
- First pass intubation success was not obtained in 22 patients of which 15 patients in this group had multiple subsequent attempts made without assisted ventilation between attempts. All 15 patients had prolonged apnea times (average 144 seconds) without desaturation, but none of them had pulmonary indications as the need for intubation.
- Some interesting stats from the paper:
Author Conclusion:
“There was no difference in lowest mean oxygen saturation between the two groups. The application of AO during RSI did not prevent desaturation of patients in this study population.”
Clinical Take Home Point:
In patients who receive proper pre-oxygenation (3min with flush 100% O2), apneic oxygenation may be a superfluous intervention, however it is important to remember that AO is not a complicated procedure, not expensive, and has not been shown to be harmful. Additionally, the absence of benefit here doesn’t mean there is no group who won’t benefit (i.e. prolonged apnea times and crash intubations) but, it is nearly impossible to make accurate prospective predictions as to which patients will benefit the most.
References:
- Caputo N et al. EmergeNcy Department use of Apneic Oxygenation Versus Usual Care During Rapid Sequence Intubation: A Randomized Controlled Trial (the ENDAO Trial). Acad Emerg Med 2017. [epub ahead of print]. PMID: 28791755
For More Thoughts on This Topic Checkout:
- Simon Carley at St. Emlyn’s Blog: JC – Apnoeic Oxygenation (Again)
- Ryan Radecki at EM Literature of Note: More Futility – Apneic Oxygenation?
- Rory Spiegel at EM Nerd (EMCrit): The Case of the Elemental Truancy
- Scott Weingart at EMCrit: Podcast 206 – ApOx, ENDAO, & PreOx Update
- 5 Minute Airway: ENDAO Trial and Interview with Nick Caputo
- Ken Milne at The SGEM: SGEM #186 – Apneic and the O, O, O2 for Rapid Sequence Intubation
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)
The post The ENDAO Trial: Is Apneic Oxygenation a Futile Intervention in ED RSI? appeared first on REBEL EM - Emergency Medicine Blog.