for all orders over $99.99 within the CONTINENTAL USA.
TOURNIQUET LAST INFORMATION / CAT COMBAT APPLICATION TOURNIQUET tm
EMS Solutions International |
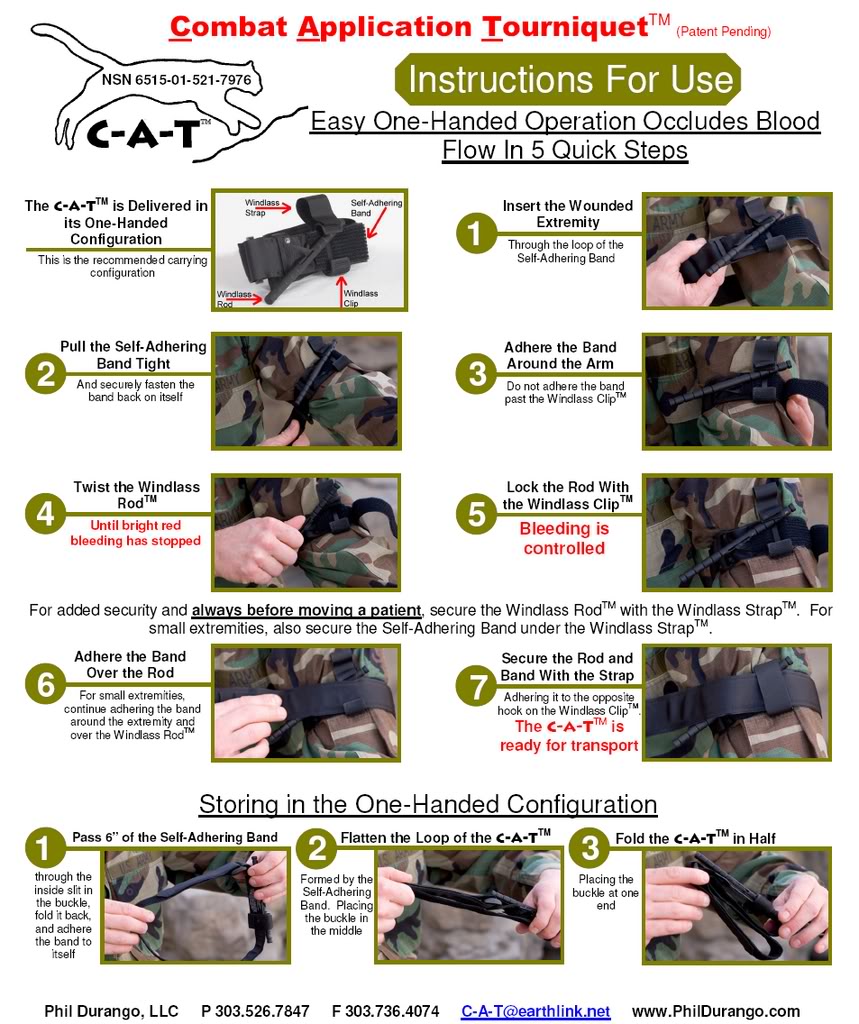
CAT COMBAT APPLICATION TOURNIQUET tm
•Un sangrado importante de una extremidad es la causa más frecuente de muertes prevenibles por una lesión
El Torniquete Es un dispositivo que detiene el flujo de sangre.
Si se aplica correctamente, el torniquete detiene el flujo arterial a la extremidad y a la herida.
Limitar la pérdida de sangre puede prevenir que el paciente entre en shock y posteriormente la muerte.
El retorno del torniquete. Lo que aprendimos de la guerra llevó a vidas salvadas en Boston
Una década después de la invasión de Irak, parece bastante claro que las aventuras militares que siguieron allí y en Afganistán han hecho más daño que bien. Miles de millones de dólares se gastaron miles de vidas perdidas, y dos regiones son ahora más estable que cuando llegamos.Pero la tragedia de ayer en Boston nos ha dado una razón para estar agradecido: el torniquete.Después de dos bombas de cocina estresantes enviados metralla a través de la multitud en la línea de muy acabado maratón como los IED que se han cobrado tantas vidas de los soldados-se habló mucho de las extremidades perdidas.Un día después de los ataques, sin embargo, sólo unos cuantos habían en realidad sido amputada: cuatro en el Hospital General de Massachusetts, cinco en el Boston Medical Center, y uno en el Hospital Brigham y de la Mujer. El recuento total de víctimas fue aún menor, a sólo tres muertes hasta el momento. Los que sobrevivieron podría tener torniquetes de agradecimiento: Los informes indican que los socorristas utilizaron cinturones, cuerdas de seguridad, arrancaron la ropa y la ropa incluso estrenar para unir las heridas de las víctimas de explosiones.Hace sólo unas semanas, un grupo de funcionarios de la FBI, Colegio Americano de Cirujanos, y la policía y las organizaciones de bomberos publicó el "Consenso de Hartford" en la forma de responder a los incidentes con víctimas masivas, como el tiroteo en Newtown, Connecticut. Su conclusión principal: La primera causa de muerte prevenible en estas situaciones es la pérdida de sangre, y la mejor manera de detener la pérdida de sangre es aplicar correctamente un torniquete.Usted no pensaría ese hecho tendría reiteración. Pero torniquetes pasó de moda hace mucho tiempo, y sólo recientemente han hecho una reaparición. De acuerdo con la American Journal of Surgery, fueron prohibidas en la práctica después de la Segunda Guerra Mundial, cuando chapuza aplicaciones bandas atadas con demasiada fuerza o demasiado sueltas llevado a más muertes y extremidades perdidas, no menos. Los torniquetes fueron utilizadas sólo ocasionalmente en las guerras de Corea y Vietnam; Estudios posteriores demostraron que podían haber evitado entre siete y 19 por ciento de las muertes en Vietnam.El ejército comenzó a entrar en razón sobre torniquetes en la década de 1990, cuando las fuerzas especiales en Somalia encontró que los utilicen correctamente salvó varias vidas. Por último, en 2003, los nuevos diseños de torniquete fueron probados para operaciones de combate en Irak y recomendados para una cuestión común a los soldados. Un estudio de 2008 de un hospital de Bagdad encontró que la tasa de supervivencia con el uso del torniquete fue del 87 por ciento.Ahora, torniquetes están haciendo poco a poco su camino de regreso a la medicina de emergencia civil también. Director médico de la Clínica Mayo Trauma Center Donald Jenkins, quien se retiró de una carrera de 24 años en la Fuerza Aérea en 2008 y ahora dirige el Instituto Nacional de Trauma, estima que un poco más de la mitad de las ambulancias llevan ahora torniquetes y debidamente capacitar al personal para utilizarlos."Después de décadas de predicando que torniquetes son malos, se podía ver cómo iba a tomar tiempo para que algo como esto a hundirse", dice Jenkins. "Los torniquetes salvaron vidas en este bombardeo de Boston, y va a aumentar el uso de ellos en otros lugares."Como suele suceder, los investigadores del Centro Médico de Boston ya habían tomado nota de la marea girando hacia torniquete en el campo de batalla, y llevó a cabo un estudio sobre las víctimas del tiroteo de civiles entre 1999 y 2006 que llegaron a una conclusión similar: Cuando se utiliza correctamente, torniquetes de trabajo, y más socorristas deberían utilizarlos. El autor del estudio, Jeffrey Kalish, dice que muchas ambulancias locales al menos llevan un tubo de goma para ese propósito.
Ni Boston Medical Center en Boston, ni servicios médicos de emergencia han respondido a las preguntas sobre cómo se utilizaron los torniquetes después de los atentados de maratón, así que todavía no pueden confirmar su eficacia. No sería la primera vez, sin embargo, que el asesinato en el extranjero ha salvado vidas en casa: los avances médicos en tiempos de guerra se han traducido siempre en la vida civil (centros de trauma completo de especialistas comenzaron a establecerse en las ciudades, por ejemplo, después de que habían trabajado a gran efecto en Vietnam). Últimos conflictos de Estados Unidos también se han mejorado las técnicas para reparar los tejidos y nervios que han impedido que las amputaciones en los quirófanos de todo el país.Ese tipo de financiación de la investigación tiende a secarse cuando los soldados regresan a casa. Sin embargo, cientos de miles de personas mueren a causa de las lesiones traumáticas cada año, y Jenkins dice que enormes brechas aún permanecen en nuestro conocimiento de cómo tratarlos. El Instituto Nacional de Trauma ha estado haciendo campaña para obtener más dinero a la investigación del trauma, que no telar tan grande en la conciencia pública como muchas enfermedades hacen."Hemos gastado millones sobre el VIH / SIDA y el cáncer de mama, y estamos viendo las tasas de supervivencia no se puede creer. La gente está sobreviviendo a mucho mayores extensiones de hoy porque tenemos centros de accidente cerebrovascular y coronaria que han demostrado a través de estudios clínicos aleatorizados lo que funciona" Jenkins dice. "Eso es todo lo que espera para suceder en el trauma. Usted puede resolver el problema, y podemos aprender mucho, sólo tenemos que aplicar los recursos para hacerlo. Simplemente no podemos conseguir la atención de cualquiera que este es un problema enorme."Quizás Boston creará ese tipo de atención. Actos internos de violencia masiva parecen ser la amenaza de esta década, después de todo, y que no deberían tener una guerra para detener la hemorragia.
FAKE TOURNIQUET Torniquete Táctico C.A.T. (Combat Application Tourniquet). Torniquete oficial de la armada de E.U. 100% efectivo para ocluir sangrado tanto en extremidades superiores como inferiores. Incluye un área para registrar por escrito la hora de colocacion.
CAT COMBAT APPLICATION TOURNIQUET
Tourniquets
A. Prehospital tourniquet use shown to have significant beneficial effect on blood loss, shock, and mortality without increased risk for amputation or conversion to higher amputation levels1
B. Application of tourniquets taught as part of echelon I (self-aid, buddy care) course to all military personnel
C. Combat Application Tourniquet System (CATS) tourniquet (see figure 12, figure 13) is most frequently used military field tourniquet and is supplied in individual first aid kits (IFAKs)
D. Tourniquets should be applied to upper thigh or upper arm for extremity injuries
E. Tourniquets best removed in operating room and may be replaced with standard pneumatic tourniquets
F. Coordination of tourniquet removal with resuscitating anesthesiologist or traumatologist is imperative, as systemic response to blood redistributing in limb and reperfusion of blood-starved tissues releasing cellular damage by-products is expected
USE of CAT COMBAT APPLICATION TOURNIQUET tm
USE of CAT COMBAT APPLICATION TOURNIQUET tm
Prehospital Tourniquet Use – A review of the current
literature
PHTLS
Lance E. Stuke, M.D. MPH
Background:
The use of extremity tourniquets for exsanguinating limb trauma has
remained controversial throughout history. The ancient Romans were likely the
first to use battlefield tourniquets and
their basic use has evolved little over the years, although many commercially
available brands are replacing the folded cravats used previously. Tourniquets
were issued in Civil War surgical sets and it was during this conflict that
enthusiasm over their use diminished, likely due to the ischemic complications
associated with prolonged delays from their application to definitive care.1
The use of tourniquets has been slowly increasing in military campaigns since the
Vietnam War but it wasn’t until the recent experience in the Iraq and
Afghanistan conflicts that widespread tourniquet use has been accepted as
standard of care in the military.
A review of civilian extremity trauma from 1994-99 noted that 86% of
patients who died from an isolated exsanguinating penetrating limb injury had
signs of life at the scene but had no discernible pulse or blood pressure upon
arrival to the hospital.2 No patient in their study had a
prehospital tourniquet placed by EMS personnel. Several factors account for the
reluctance of EMS personnel to use tourniquets. These factors include the
perceived complications of nerve injury and deep vein clot formation and the
notion that limb ischemia could increase the risk of future amputation. Since
the publication of these initial reports, civilian use of tourniquets is becoming
accepted as standard of care, primarily due to the data derived from the recent
military experience in Iraq and Afghanistan.
The 6th Edition of the PHTLS
textbook endorses the use of tourniquets if external bleeding cannot be
controlled by direct pressure. It also notes that elevation of an extremity and
compression on a pressure point proximal to the injured site are not proven
methods of hemorrhage control and are not endorsed by PHTLS. The 6th
edition endorsement of tourniquet use is based on several small published
studies demonstrating benefit as well as early evidence arising at the time
from the Iraq conflict. Since the publishing of the 6th edition,
significant additional data has appeared in the trauma surgical literature to
support the use of tourniquets. We will review these new studies in an effort
to keep PHTLS providers abreast of the latest literature on this subject.
CAT COMBAT APPLICATION TOURNIQUET tm
Literature Review:
The first large study to
retrospectively review tourniquet use by the U.S. military in Iraq was
published in the Journal of Trauma by Beekley, et al.3 The authors
reviewed their experience during 2004 in Iraq. This was relatively early in the
conflict and widespread tourniquet use among military personnel was still in
its infancy. The authors reviewed 67 patients who had prehospital tourniquets
placed and another 98 patients with severe extremity trauma who did not have
tourniquet placement. The average tourniquet time was 70 minutes (range 5-210
minutes). While a survival benefit to tourniquet use was not demonstrated in
this initial study, the authors found that among the most severely injured
patients (Injury Severity Score > 15) prehospital tourniquet use significantly
improved hemorrhage control. No early adverse outcomes from tourniquet use were
noted among the survivors. The authors discuss the challenges faced by
providers in the combat environment and recognize that documentation of successful
hemorrhage control, tourniquet application time, and vital signs was often
inadequate. Furthermore, a comprehensive military trauma database was still
under development so hospital records were often suboptimal. This study is
significant in that it demonstrated that battlefield tourniquets can safely be
applied by prehospital personnel with no significant side-effects. Critics
point out the retrospective nature of the study as well as the author’s
admitted difficulty in data collection early in the war. As data gathering methods
improved over the next several years, future research would expand on this
early study
The next two articles are from the
prospectively gathered trauma database by the U.S. military in Iraq.4,5
The articles represent the work from a single combat hospital in Baghdad and
cover a span of seven months, March to October 2006. During this time, 2,838
patients were admitted with major limb trauma of which 8% (232 patients) had
428 tourniquets placed on 309 limbs. Some patients had multiple limbs injured, while
others had an additional tourniquet placed on the same limb if the initial
placement did not adequately control hemorrhage. The average tourniquet time was 1.3 hours.
The first article from this
prospective database was published in the Journal of Trauma and evaluated
complications associated with tourniquet use.4 Four patients had nerve palsies diagnosed at
the level of the tourniquet, three of which improved within a day. Only one
patient had mild persistence of his nerve palsy at 6 days. Seven patients had
skin pinching, blisters, abrasions, or bruises in the area directly under the
tourniquet. Ten blood clots were noted although the surgeons attributed these
to be secondary to the injury itself and not to tourniquet use. No patient
developed a pulmonary embolus. There was no apparent association between
tourniquet time and the development of clots, nerve palsies, pain, or
myonecrosis. Nine fasciotomies were done, but all were prophylactic to prevent
compartment syndrome and no cases of compartment syndrome were noted from
tourniquet use. Nearly all tourniquets were properly positioned (97%). The low
rate of complications noted in this study compares favorably with other prior
studies from as far back as World War II which all demonstrate little or no
morbidity associated with tourniquet placement.
The next article, published in
Annals of Surgery, represents the first prospectively gathered data to
demonstrate the survival benefit of tourniquet use.5 The authors
first note five patients who met eligibility criteria for prehospital
tourniquet placement who did not receive a tourniquet for various reasons. All
five patients were alive in the field, bled to death in the presence of fellow
soldiers, and arrived at the hospital 10-15 minutes later without vital
signs. The authors conclude those deaths
could have been prevented with early tourniquet placement. They also note that
timing is critical to tourniquet placement. The patient must have a tourniquet in place
before the onset of shock. Patients with a tourniquet placed in the absence of
shock had a 90% survival rate versus a 10% survival rate in those whose
tourniquet was placed after development of shock. The median time to placement
after injury was 10 minutes and placement should be done prior to extrication
from the vehicle and transport to the hospital.
The final study to review is a
continuation of the previous two papers from the same combat support hospital
in Iraq.6 The authors conducted this study to see if their initial
data supporting the use of tourniquets held up as more patients were enrolled
in the study over time. The study population included 499 total patients, with
862 tourniquets applied on 651 limbs. A survival advantage was noted in
patients who had a tourniquet applied early, before the onset of shock (96%
before vs 4% after). Furthermore, a survival benefit was noted in patients with
prehospital application of a tourniquet versus hospital application (89% vs 78%
hospital). Complications associated with tourniquet placement, such as nerve
palsies, remained extremely low in this study as well (< 1.5%). The authors
conclude that early tourniquet application, before the onset of shock, saves
lives with little to no associated complications.
Summary:
-Prehospital
tourniquets are indicated if direct pressure or a pressure dressing fails to
control hemorrhage.
-The
tourniquet should be placed prior to extrication and prior to transport. There
is a clear survival advantage if placement is done prior to the onset of shock.
-The
tourniquet is tightened until hemorrhage ceases. An additional tourniquet can
be placed next to the first tourniquet if bleeding control is inadequate
following placement of the first tourniquet.
-The
patient should be transported to a hospital with immediate surgical
capabilities whenever possible.
-The
time of tourniquet application should be documented and relayed to the trauma
team upon arrival at the hospital.
-There
are few, if any, significant complications attributed to tourniquet use. It is
a safe procedure, should be performed by all EMS personnel, and saves lives.
PHTLS
Recommendation:
PHTLS recommends the placement of
tourniquets by EMS personnel if direct pressure fails to control extremity
hemorrhage.
Bibliography:
Doyle GS and Taillac PP. Tourniquets: A review of
current use with proposals for expanded prehospital use. Prehospital Emergency Care. 2008;
12: 241-256.
Dorlac WC, DeBakey ME, Holcomb JB, et al.
Mortality from isolated civilian penetrating extremity injury. Journal of Trauma. 2005;59: 217-222.
Beekley AC, Sebesta JA, Blackbourne LH, et al.
Prehospital tourniquet use in Operation Iraqi Freedom: Effect on
hemorrhage control and outcomes. Journal
of Trauma. 2008; 64: S28-S37.
Kragh JF, Walters TJ, Baer DG, et al. Practical
use of emergency tourniquets to stop bleeding in major limb trauma. Journal of Trauma. 2008;64: S38-S50.
Kragh JF, Walters TJ, Baer DG, et al. Survival
with emergency tourniquet use to stop bleeding in major limb trauma. Annals of Surgery. 2009;249: 1-7.
Kragh JF, Littrel ML, Jones JA, et al. Battle
casualty survival with emergency tourniquet use to stop limb bleeding. Journal of Emergency Medicine. 2009.
Article in press.
TOURNIQUET LAST INFORMATION / CAT COMBAT APPLICATION TOURNIQUET tm
Tourniquet Slack: Pulling tight is more important than the windlass
You keep twisting the windlass on your tourniquet, 5,6,7…11 times and you’re still bleeding… What is going on during the worst day of your life?!
A portion of literature on tourniquets has recognized failure with slack. This means operators are twisting the windlass before pulling as much slack as they can through the friction adapter/buckle, which causes the TQ to not be as tight as possible.
How do I address and prevent this?
I incorporate a “Slack Drill” into my TCCC classes before standard tourniquet drills. Before I let my students touch the windlass, I tell them “make it as tight as possible by just pulling the slack out, every centimeter, as if windlass doesn’t exist and that is all you have to stop the bleed.”
I then walk around the room and get at least a few centimeters, if not inches, out of some students slack to show them the standard.
THEN I tell them to turn the windlass and they can strongly get a feel for themselves that when a tourniquet is tight enough, the “patient” your student is practicing on grimaces halfway through the first turn and does NOT want to experience twisting until total arterial occlusion. That is a huge difference from not being aggressive when pulling slack and ending up rotating that windlass all day frivolously and causing blood loss and/or compartment syndrome.
In addition, teach your students how to “reset” a training tourniquet by grabbing the ends and pulling to lengthen out the internal band when doing drills. A tourniquet still “tight” from the last training application won’t go on as realistically and will therefore cause possible training scars and windlass emphasis.
*Training tourniquets should never be used on real casualties.
Consider addressing this in your class by emphasizing getting the slack out so we can lower operator induced tourniquet failure.
Here’s just a couple studies I easily grabbed off google, there are more:
* Confidence-Competence Mismatch and Reasons for Failure of Non-Medical Tourniquet Users. Baruch EN, et al. Prehosp Emerg Care. 2017 Jan-Feb.
* No Slackers in TQ Use to stop bleeding: https://www.jsomonline.org/SharedScience/2013212Polston.pdf Thanks to , Journal of Special Operations Medicine
Official Spanish Army Kit
MILITARES ESPAÑOLES USAN EL TORNIQUETE COMO PIEZA ELEMENTAL DE SU EQUIPO DE PROTECCIÓN. "Nadie debe morir por un sangrado descontrolado" Consenso Hartford Curso B-Con-PHTLS El Torniquete es un dispositivo que detiene el flujo de sangre. Si se aplica correctamente, el torniquete detiene el flujo arterial a la extremidad y a la herida. Limitar la pérdida de sangre puede prevenir que el paciente entre en shock y posteriormente la muerte TORNQUETES FALSOS "FAKE"
#Fake#TQ#Torniquete vs #TQoriginales#TorniquetesOriginales
#SAMXT#TIE#SICH#CAT
CAT torniquete mas falsificado del mercado
School District Issues Counterfeit Tourniquets. Although initially imported as toys for the airsoft community, they’re now making their way into legitimate medical kits and systems.
The counterfeit tourniquets have failed operationally in the United States. See more on today's blog
No puedes inventar con estas cosas: publicidad real de un fabricante de tq falsos 🤬
Si no tuviera el potencial de costarle a alguien el miembro o su vida, sería muy divertido: esto es LARPING en un nuevo nivel de peligro. Si valoras tu vida, ¡no caigas en la tentación de ahorrar un par de US$ dólares/ € por adquirir imitaciones! ¿Has leído la publicación de @nardoctor desglosando un nuevo estudio sobre solo una variedad de falsificaciones? ¡En ese, el 20% de ellos fallaron versus el 100% de éxito de los CAT genuinos! Pero si te gusta jugar con tu vida y la vida de los tuyos, tus compañeros o una persona inocente, ahí esta... posted by Dr. Ramon Reyes, MD ∞🧩
Dr Ramon REYES, MD, Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..


{kind=link}
{kind=link}














