
 Typically, the initial evaluation of blunt trauma patients involves a supine anteroposterior (AP) chest x-ray (CXR) which has a poor sensitivity for the detection of pneumothorax (PTX), and has been reported as low as 20% – 48%. Following the CXR computed tomography (CT) has been the standard for the diagnosis of pneumothorax. The use of ultrasonography to diagnose pneumothorax was first described in 1986 in animal studies. Since then there have been many studies that have shown bedside ultrasound can rapidly detect pneumothorax, helping avoid serious potential consequences (i.e. tension pneumothorax), especially in patients requiring mechanical ventilation. There are several different sonographic signs that can be used to detect pneumothorax, specifically, sonographic lung sliding. But how good is ultrasound for the detection of pneumothorax?
Typically, the initial evaluation of blunt trauma patients involves a supine anteroposterior (AP) chest x-ray (CXR) which has a poor sensitivity for the detection of pneumothorax (PTX), and has been reported as low as 20% – 48%. Following the CXR computed tomography (CT) has been the standard for the diagnosis of pneumothorax. The use of ultrasonography to diagnose pneumothorax was first described in 1986 in animal studies. Since then there have been many studies that have shown bedside ultrasound can rapidly detect pneumothorax, helping avoid serious potential consequences (i.e. tension pneumothorax), especially in patients requiring mechanical ventilation. There are several different sonographic signs that can be used to detect pneumothorax, specifically, sonographic lung sliding. But how good is ultrasound for the detection of pneumothorax?
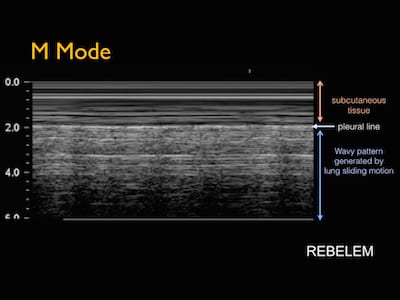
What does normal lung sliding look like?
What are the sonographic signs used to detect a PTX on ultrasound? [1]
- Lack of lung sliding: Back and forth movement of parietal and visceral pleura sliding on each other with normal respiration
- Lack of power slide: Using power doppler to detect the subtle motion of sliding pleural lines
- Absence of normal comet tail or reverberation artifacts: This artifact arising from the deeper visceral pleura should normally move with the lung during respiration and is absent when air or pneumothorax is present
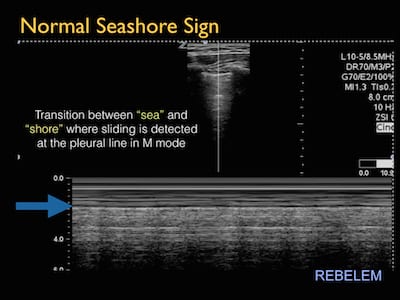
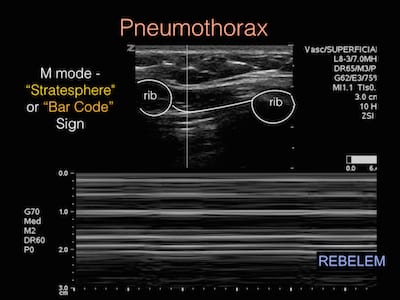
- “Stratosphere” or “Bar Code” sign: M mode detects the difference in motion between the two pleural lines. Normal lung will show a “seashore sign” with transition of lines differentiating movement at the pleural lines, whereas pneumothorax prevents detection of motion creating a single “bar code” pattern
- Presence of a “lung point” or “transition point”: Transition seen between normal sliding lung and no sliding at the pneumothorax border. Improves specificity for pneumothorax when sliding is present, however its absence does not rule it out (i.e. large pneumothoraces where lung is completely collapsed and borders not visualized)
What is the sensitivity and specificity of ultrasound for detection of PTX when performed by ED physicians after blunt trauma? [2]
What they did:
- 606 patients collectively evaluated between 1965 – 2009
- Literature review of prospective trials analyzing performance of ED physicians performing US for detection of PTX in adult, trauma patients
- Comparison of supine CXR vs US for detection of PTX
Results:

- US for detection of PTX: Sensitivity 86 – 98% and Specificity 97 – 100%
- AP CXR for detection of PTX: Sensitivity 28 – 75% and Specificity 100%
Limitations:
- Only blunt trauma patients included (i.e. No evaluation of spontaneous, iatrogenic, or penetrating PTX)
- Many studies were not randomized
- Patients with crepitus, requiring immediate surgical intervention were excluded
- No evaluation of effect on patient care (i.e. What is the effect of missing an occult PTX not detected by US or CXR found on CT). This is still a controversial topic especially in patients receiving positive pressure ventilation.
Conclusions: Ultrasound is superior to CXR at detection of pneumothorax
How does use of ultrasound for detection of pneumothorax perform in the non-trauma setting?
It has been suggested that the absence of lung sliding for the detection of pneumothorax in critically ill ICU patients (aside from trauma patients) is much less specific and can be more difficult because sliding is more difficult to appreciate in this group of patients. Recently, Lichtenstein et al. [3] stated the PPV of abolished lung sliding for PTX was only 87% in the general population [4], and as low as 56% in the critically ill [5], down to 27% in patients with respiratory failure [6].
- Lichtenstein et al (1995) [4]: 109 hemithoraces of critically ill ICU patients, 47 cases had no lung sliding, 62 had lung sliding, and 2 were inconclusive; All proven pneumothoraxes had no lung sliding but there were 6 false positives (Sensitivity 95.3%, Specificity 91.1%, NPV 100%, and PPV 87%)
- Lichtenstein et al (2000) [5]: 299 hemithoraces in ICU patients for detection of lung sliding and presence of lung point compared to CXR and the gold standard CT:
- Absent lung sliding alone = Sensitivity 100%, Specificity 78%, PPV of 57%, NPV 100%
- Conclusion: All proven pneumothoraces had no lung sliding, but there are some cases of false positives with no lung sliding in critically Ill ICU patients
How does the presence of additional artifacts (i.e. B Lines or comet tails) affect these results?
- In patients with no lung sliding, the presence of B lines or comet tails can still rule out pneumothorax, and using these signs combined improves the specificity and PPV of lung ultrasound for pneumothorax detection
- Positive Test = No lung sliding present and absence of B lines
- Negative Test = Sliding present, or no lung sliding but visible B lines
- Sensitivity 100%, Specificity 95%, PPV 85%, NPV 100%
- Conclusion: In the presence or absence of lung sliding, visible B lines or comet tails can rule out pneumothorax in critically ill ICU patients
What is the sensitivity, specificity, PPV, NPV of lung point alone?
- In all cases of absent lung sliding and absent B lines or comet tails, Lichtenstein further searched for a lung point or transition point
- Positive test = lung point present
- Negative test = no lung point present
- Sensitivity 67%, Specificity 100%, PPV 100%, NPV 91%
- Conclusion: In the absence of lung sliding, B lines, and comet tails, the presence of a lung point has 100% specificity and PPV for pneumothorax in critically ill ICU patients
What is the take home message?
- Absence of lung sliding is much less specific in respiratory distress and critically ill ICU patients compared to trauma patients
- Additional signs such as comet tails or B lines can improve the specificity and PPV in those critically ill patients, and essentially rules out pneumothorax when lung sliding is absent
- The presence of a lung point and no lung sliding improves the specificity to 100% for pneumothorax, however its absence does not rule out pneumothorax, as very large PTX may not have a detectable lung point
What can lead to false positive PTX detection?
The absence of lung sliding alone is very sensitive for PTX, but not specific in ICU patients because of a large number of false positives. Detection of sliding and artifacts requires tissue air interface at the pleural line. Things that may cause false positives, especially in non-trauma, critically ill patients:
- Dyspnea causes interference above the pleural line
- Single lung intubation, or esophageal intubation can lead to secondary atelectasis
- Lung and pleura adhering together (i.e ARDS and chronic pleuradesis, or adherences from cancer)
- Phrenic palsy
- Pulmonary fibrosis
- Cardiopulmonary arrest
- Poor operator skill or inappropriate equipment/settings
- Large infiltrates and pleural effusions (considered non aerated patterns and may also interfere with the detection of lung sliding)
- In trauma patients pulmonary contusions may also cause similar interference
- COPD and asthma may have a large number of A lines (horizontal lines) which are seen in PTX, but should still have sliding present, however this can create confusion for physicians unaware of the difference
Does using power doppler for detection of power slide, change the performance of ultrasound for detection of PTX? [7]
Cunningham et al describe a case in which a patient with a proven hemo-pneumothorax had undetectable “power slide” in addition to absent sliding and comet tail artifacts.
- They suggest the absence of a “power slide” may be sufficient to rule in a pneumothorax
- It is unclear as this has not been studied if the “power slide” would be be subject to the large number of false positives as regular lung sliding seen in grey scale
- Although, frequently taught and talked about, the relevance of a power slide is unclear, and may or may not improve specificity and PPV
Take Home Points
- The presence of lung sliding in both blunt trauma and critically ill ICU patients can rule out the presence of a pneumothorax
- Ultrasound outperforms CXR in evaluation of pneumothorax in blunt trauma patients, but there may be other traumatic injuries that are detected on CT that are not detected on CXR or US
- The absence of lung sliding alone is not specific enough to rule in a pneumothorax in critically ill ICU patients
- Presence of a lung point is 100% specific and 100% predictive of PTX when seen, but may not be seen in large pneumothoraces
- Power slide is a described use of power doppler to aid in detection of lung sliding, however its utility is not known to date
References:
- Husain LF et al. Sonographic Diagnosis of Pneumothorax. J Emerg Trauma Shock 2012. PMID: 22416161
- Wilkerson RG et al. Sensitivity of Bedside Ultrasound and Supine Anteroposterior chest Radiographs for the Identification of Pneumothorax After Blunt Trauma. Acad Emerg Med 2010. PMID: 20078434
- Lichtenstein DA. Lung Ultrasound in the Critically Ill. Ann Intensive Care 2014. PMID: 24401163
- Lichtenstein DA et al. A Bedside Ultrasound Sign Ruling Out Pneumothorax in the Critically Ill. Lung Sliding. Chest 1995. PMID: 7587439
- Lichtenstein D et al. The “Lung Point”: An Ultrasound Sign Specific to Pneumothorax. Intensive Care Med 2000. PMID: 11126253
- Lichtenstein DA et al. Relevance of Lung Ultrasound in the Diagnosis of Acute Respiratory Failure: The BLUE Protocol. Chest 2008. PMID: 18403664
- Cunningham J et al. Enhanced Recognition of “Lung Sliding” with Power Color Doppler Imaging in the Diagnosis of Pneumothorax. J Trauma 2002. PMID: 11956400
- Blaivas M et al. A Prospective Comparison of Supine Chest Radiography and Bedside Ultrasound for the Diagnosis of Traumatic Pneumothorax. Acad Emerg Med 2005. PMID: 16141018
- Soldati G et al. The Ultrasonographic Deep Sulcus Sign in Traumatic Pneumothorax. Ultrasound Med Biol 2006. PMID: 16875950
- Zhang M et al. Rapid Detection of Pneumothorax by Ultrasonography in Patients with Multiple Trauma. Crit Care 2006. PMID: 16882338
- Soldati G et al. Occult Traumatic Pneumothorax: Diagnostic Accuracy of Lung Ultrasonography in the Emergency Department. Chest 2008. PMID: 17925411
The post Ultrasound for Detection of Pneumothorax appeared first on REBEL EM - Emergency Medicine Blog.