
 BACKGROUND: intracerebral hemorrhage (ICH) makes up 10-15% of all strokes and significantly contributes to overall stroke-related morbidity and mortality (Hostettler 2019). Levetiracetam is frequently used to prevent seizures in patients with conditions such as ICH, traumatic brain injury (TBI), supratentorial neurosurgery, and subarachnoid hemorrhage (SAH). However, guidelines offer no strong recommendations for its use, specifically in spontaneous ICH (Fang 2021). Ongoing debates persist regarding the drug’s effectiveness, optimal dosage, and potential side effects.
BACKGROUND: intracerebral hemorrhage (ICH) makes up 10-15% of all strokes and significantly contributes to overall stroke-related morbidity and mortality (Hostettler 2019). Levetiracetam is frequently used to prevent seizures in patients with conditions such as ICH, traumatic brain injury (TBI), supratentorial neurosurgery, and subarachnoid hemorrhage (SAH). However, guidelines offer no strong recommendations for its use, specifically in spontaneous ICH (Fang 2021). Ongoing debates persist regarding the drug’s effectiveness, optimal dosage, and potential side effects.
About 30% of patients experience early seizures within seven days following the onset of a stroke (Peter-Derex 2022). While clinical seizures are readily identifiable, subclinical seizures—which comprise most seizures after a hemorrhage—are hard to detect. The long-term impact of these subclinical seizures is still unclear. More research is needed to inform preventive treatment strategies for seizures in patients with spontaneous intracerebral hemorrhage (ICH).
Article: Peter-Derex et al. Safety and efficacy of prophylactic levetiracetam for prevention of epileptic seizures in the acute phase of intracerebral hemorrhage (PEACH): a randomized, double-blind, placebo-controlled, phase 3 trial. Lancet Neurology 2022; 21:781-91. PMID: 35963261. ClinicalTrials.gov: NCT02631759
Clinical Question: In adult patients aged 18 years or older presenting within 24 hours of a spontaneous ICH, does the administration of levetiracetam, compared to placebo, reduce the occurrence of clinical seizures?
WHAT THEY DID
- Investigators performed a double-blinded, randomized, placebo-controlled parallel-group trial at three-stroke centers in France.
- They selected adult patients with spontaneous intracerebral hemorrhage on CT imaging within 24 hours of symptom onset.
- Patients were randomly assigned (1:1) to receive levetiracetam or a matching placebo.
- Continuous EEG was performed for a total of 48 hours. Thereafter, clinical seizures were objectively reported.
- Study subjects were stratified by the institution and by NIHSS score (≤15 or >15). Neurologic deficits were assessed at 72 hours, 1 month, and 3 months after randomization.
POPULATION
Inclusions:
- Age ≥ 18 years of age
- Radiographically confirmed spontaneous supratentorial intracerebral hemorrhage
- Symptom onset within 24 hours of presentation
Exclusions:
- National Institute of Health Stroke Scale (NIHSS) > 25
- ICH that is known or suspected to be secondary to tumor, vascular malformation, hemorrhagic conversion of ischemic stroke, or trauma.
- Current use of anti-seizure medications or history of epilepsy
- Pregnancy or breastfeeding
- History of severe depression or psychotic disorder
- Known terminal illness
- Allergy or hypersensitivity to levetiracetam
- Occurrence of an epileptic seizure between inclusion and initiation of treatment
INTERVENTION
- Levetiracetam 500mg intravenous infusion every 12 hours for 48 hours followed by 30 days at the same oral dose and then a 2-week taper.
CONTROL
- A matching placebo was administered intravenously and orally following the same dosing schedule as the levetiracetam group.
OUTCOMES
Primary:
- Occurrence of at least one clinical or electrographic seizure recorded on continuous EEG within 72 hours after inclusion.
Secondary:
- Number of seizures recorded on continuous EEG.
- The total duration of seizures was recorded on continuous EEG.
- The number of clinical seizures within 72 hours and early (day 0 to day 30) and late (day 30 to 12 months) clinical seizures.
- Change in NIHSS scores between inclusion and 72 hours, 1 month, and 3 months.
- Change in modified Rankin Scale (mRS) scores between inclusion and 3 months, 6 months, and 12 months.
- The Stroke Impact Scale was used to assess quality of life at 3 months, 6 months, and 12 months.
- Change in intracerebral hemorrhage volume and mass effect defined as midline shift at 72 hours.
Secondary Safety Outcomes:
- The frequency of side effects related to treatment, anxiety, and depression was evaluated with the Hospital Anxiety and Depression Scale at 1 month and 3 months
- All-cause mortality
RESULTS
-
50 patients were enrolled in the trial
- Trial enrollment was discontinued due to the COVID-19 pandemic and the cessation of funding.
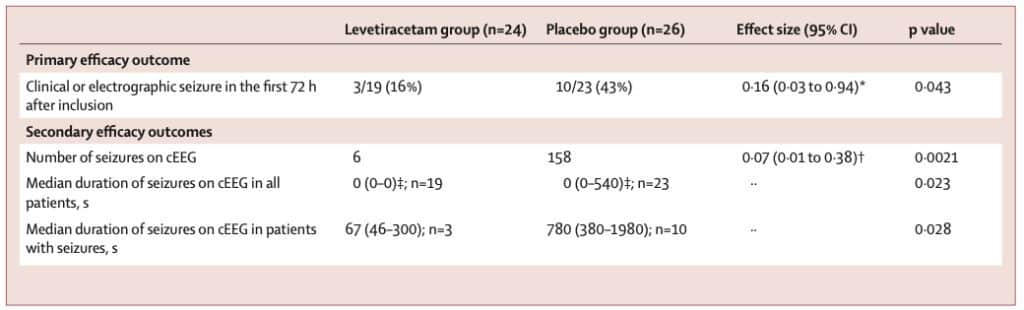
- 16% of the levetiracetam group and 43% of the placebo group were found to have seizures, which was statistically significant. (OR 0.16, 95% CI 0.03-0.94, p=0.043)
- 158 seizures were seen on cEEG in the placebo group compared to 6 in the levetiracetam group. (OR 0.07, 95% CI 0.01-0.38, p=0.0021)
- No statistically significant results were reported in the other clinical outcomes studied.
STRENGTHS
- Investigators asked a clinically relevant research question.
- The primary outcome was patient-oriented.
- The trial was randomized and double-blind, minimizing bias.
- The patients, all members of the clinical team, and outcome assessors were masked to the treatment allocation.
- All participants received the standard treatment protocol, which helped minimize the confounding variables’ potential influence.
- The intervention and therapy were both masked in appearance and had identical packing.
- Randomization protocol utilized a centralized web-based platform less prone to manipulation and unblinding (i.e., sealed envelopes).
- Investigators performed an intention-to-treat analysis.
- Patients were followed for up to 12 months, a sufficient period to capture the occurrence of seizures or other relevant outcomes.
- The trail was registered, which increases transparency and potential for reproducibility.
LIMITATIONS
- The study was conducted in a single country. Patients from a single country may not be reflective of all patients with ICH and seizures.
- It is unclear how many patients were eligible for enrollment but not enrolled. It is unclear whether patients who were potentially eligible but not enrolled represent the studied population, creating a selection bias.
- The study was stopped early due to a loss of funding attributed to the COVID-19 pandemic. Trials that are stopped early are at risk of over or underestimating the results.
- The study ran for 34 months at 3 hospitals, but investigators recruited less than 1 patient per month, indicating the presence of selection bias.
- The study is markedly underpowered. Investigators determined 104 patients were required for adequate power but only recruited 50.
- The average GCS in both groups was 15. The results would not apply to patients with severe intracerebral hemorrhage.
- Baseline characteristics differed in the two groups; NIHSS was higher in placebo, and hematoma volume was twice the size.
- It’s unclear if treatment outside of the investigated drugs was the same in both groups.
DISCUSSION
- No clinical seizures were observed in either treatment group during the first 72 hours, calling into question the efficacy of levetiracetam in preventing acute-phase seizures. Additionally, the long-term impact of preventing subclinical seizures remains uncertain, as it’s unclear whether such seizures lead to worse outcomes.
- The investigators found a statistically significant decrease in subclinical seizures seen only on EEG. They mention that continuous EEG is not routinely used in the setting of intracerebral hemorrhage. The sensitivity and specificity of continuous EEG to detect non-convulsive seizures range from 65-83% and 65-92%, respectively. [Sansevere 2019] This challenges the validity of the results—researchers are basing statistical significance on a diagnostic modality that is not routinely used and is perhaps only adequate at detecting seizures.
- The study did not clearly define the standard of care, introducing the potential for co-intervention bias. It’s unclear what additional treatments may have been administered that could have influenced the outcomes.
- The findings in this underpowered study, which was stopped early and has a limited sample size, may be due to chance alone, and a larger study could potentially yield different results.
- The paper has a fragility index of 0, meaning a different outcome in one patient in either group could alter the study’s statistical significance.
- Although the study concluded that levetiracetam reduced seizure incidence in ICH patients compared to a placebo, the placebo group had worse baseline NIHSS scores and larger initial hematomas. This suggests that the placebo group may have been inherently more susceptible to seizures, which could solely explain the statistically significant difference observed.
Author’s Conclusion: “Levetiracetam might be effective in preventing acute seizures in intracerebral hemorrhage. Larger studies are needed to determine whether seizure prophylaxis improves functional outcomes in patients with intracerebral haemorrhage.”
Bottom Line:
We agree with the author’s conclusion. The paper presents interesting data. However, the differences in demographics suggest that the studied populations were unequal, and patients in the placebo arm may have had a higher baseline predilection for seizure. Furthermore, the small sample size makes the study markedly underpowered. Larger multicenter RCTs are still required to inform decisions on seizure prophylaxis in patients with ICH.
For More on This Topic:
https://www.emra.org/emresident/article/cca-peach-trial
https://first10em.com/the-peach-trial-of-seizure-prophylaxis-for-head-bleeds-not-such-a-peach
References:
- Hostettler IC, Seiffge DJ, Werring DJ. Intracerebral hemorrhage: an update on diagnosis and treatment. Expert Rev Neurother. 2019 Jul;19(7):679-694. doi: 10.1080/14737175.2019.1623671. Epub 2019 Jun 12. PMID: 31188036.
- Fang T, Valdes E, Frontera JA. Levetiracetam for Seizure Prophylaxis in Neurocritical Care: A Systematic Review and Meta-analysis. Neurocrit Care. 2022 Feb;36(1):248-258. doi: 10.1007/s12028-021-01296-z. Epub 2021 Jul 20. PMID: 34286461.
- Peter-Derex et al. Safety and efficacy of prophylactic levetiracetam for prevention of epileptic seizures in the acute phase of intracerebral hemorrhage (PEACH): a randomized, double-blind, placebo-controlled, phase 3 trial. Lancet Neurology 2022; 21:781-91. PMID: 35963261
- Sansevere AJ, Hahn CD, Abend NS. Conventional and quantitative EEG in status epilepticus. Seizure. 2019 May;68:38-45. doi: 10.1016/j.seizure.2018.09.011. Epub 2018 Oct 6. PMID: 30528098
Guest Post By:

Carlton C.L. Watson, MD, MSc
PGY-1 , Emergency Medicine Resident
Nuvance Health, Poughkeepsie, New York
Twitter: @justcarlton

Marco Propersi, DO, FAAEM
Vice-Chair, Emergency Medicine
Vassar Brothers Hospital, Poughkeepsie, New York
Twitter: @marco_propersi
Post-Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami) and Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Unpacking the PEACH Trial: What is Levetiracetam’s Role in Spontaneous Intracerebral Hemorrhage? appeared first on REBEL EM - Emergency Medicine Blog.