
 Hacks are all the rage! There is even a current television show dedicated to “life hacks”. While the following may not be as cool as cutting cake with dental floss or cooking a pizza on your dash board (these were actually on that show) what I have learned from my training and experience in Pediatric Emergency Medicine (and my own 5 children) is that there are some hacks that can make things much easier for you, the kid, and the parents. The hacks presented here range from treatment for common (and often benign) conditions to serious situations.
Hacks are all the rage! There is even a current television show dedicated to “life hacks”. While the following may not be as cool as cutting cake with dental floss or cooking a pizza on your dash board (these were actually on that show) what I have learned from my training and experience in Pediatric Emergency Medicine (and my own 5 children) is that there are some hacks that can make things much easier for you, the kid, and the parents. The hacks presented here range from treatment for common (and often benign) conditions to serious situations.
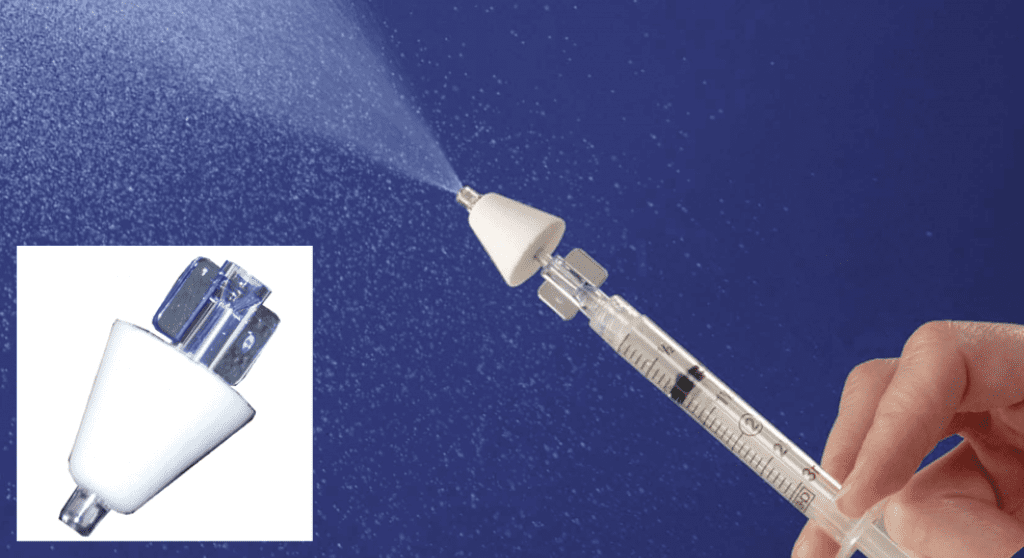
1. Intranasal (IN) Atomizers: I’m not really sure how we practiced without these before. While I think they are becoming more and more common in EDs across the country, there are still many departments slow to join the club on this one. It is amazing how useful it is in the child showing up with a long bone fracture to gain control of the pain. Get those x-rays BEFORE starting an IV [1]. IN Fentanyl can start that entire encounter off in a much more positive fashion. Avoid the child screaming about the IV stick, WHILE in pain from an acute fracture.
In case you didn’t know, there is also usefulness for IN route Midazolam in minor procedures that require “anxiolysis” (don’t call it sedation) along with local anesthesia (see next Hack) [2]. Think of it as a Pediatric “Margarita” (or 2). Many situations look better and friendlier with a Margarita…right (disclaimer…I am not an alcoholic…)?
It is also nice for seizure “lysis” when you don’t have IV access and may not want to do IM route [3].
2. LET (Lidocaine Epinephrine Tetracaine) gel: We already know that this decreases the pain for subsequent local infiltration [4]. My experience is that it is even more effective than that! In many anxious kiddos with a simple facial laceration, I apply the following sequence: LET applied, 15 minutes elapses, then IN Midazolam dose, then another 15 minutes elapses to achieve maximal “anxiolysis” [5] combined with the now full 30 minutes of LET in the wound. Anecdotally, if you add a screen playing Frozen (or better yet a Child Life Specialist) or even an Ipad (with a protective cover being held by the parents), the “rodeo” factor (screaming, hollering, bucking, snorting, slobbering, etc.) of these repairs is significantly lessened. We often do not even have to locally infiltrate the wound if the LET has been allowed the full 30 minutes for the suture repair with the Midazolam on board. No sedation paperwork required…LET it go…LET it go…
3. Rapidly absorbing sutures for facial lacerations: If you have ever had to wrangle a 3-6 year old to take out barely visible 6.0 sutures from a well healed facial lac repair…you are going to want to change to absorbable (especially on the face). The face in children has amazing vascular and healing properties. The lac only needs to be “held together” for a short period of time. The parents also LOVE not having to return to the ED for suture removal [6].
4. Docusate sodium (Colace) for the constipated…EAR: So the non-toxic 4 year old has a fever and the parents want to know what the eardrums look like because 5 months ago with these same symptoms the child was diagnosed with a “Triple Ear Infection”!!! You look and…uhhh, this kid is a grade A earwax farmer. You also aren’t thrilled about the idea of holding this grumpy, febrile kid down trying to scrape the wax out with whatever ear spoon/loop you have available. For me, this usually ends with screaming, a bloody ear canal, and judgmental looks from parents. So how about while giving an appropriate dose of ibuprofen and allowing the child to defervesce, you put 1 ml (or what the canal can tolerate) of Colace (right out of the soft-gel) and cotton to keep it in; and then 15-20 minutes later have your excellent nurses irrigate with room temp water [7]. Occasionally my nurses will catch the chunks of ear wax in an emesis basin and show off their cerumen bounty. Then take a look in the ears! So much easier than another ear loop “rodeo”.
5. Popsicles: Okay don’t laugh…these really are the “fuel” of the Pediatric ED patient. We already know that oral rehydration is the way to go the vast majority of the time [8][9]. My hack here is that in many instances, a Popsicle goes over better (in the ED) than “drink this entire bottle of Pedialyte”. I like it because it slows them down from chugging right after the anti-emetic kicks in. Their stomach is in a bit of a fragile state, so pounding 6 ounces of anything is often tolerated poorly. But with a Popsicle, it’s colorful, sweet, cold, and you can’t chug it. It essentially forces the child to start out with “sip volumes” as we enter back on the road to oral rehydration.

6. Pediatric appropriate NIV (aka Hi-Flow NC or Peds Bi-pap/C-pap set up): Admittedly this category requires more EM research in the pediatric realm [10]. The reason I think it is so critical to share with you is the number of times I have used, seen, and heard this as a wonderful tool to prevent the dreaded intubation in the moderate to severe asthmatic or bronchiolytic. Research suggests that Pediatric EDs are using non-invasive ventilation as an asthma “intubation prevention” more than community EDs[11]. It also suggest that community EDs intubate asthmatics more commonly[12]. I realize this is due to a variety of factors including equipment availability, transport considerations, and respiratory therapy expertise. I would urge you to know what your ED’s capabilities are for non-invasive ventilation in children. If they are low or non-existent, consider investing in training and development for this modality in the pediatric population. It can be a wonderful bridge from significant presentation to recovery without having to face the dreaded intubation in the asthmatic (or bronchiolytic). Hi-Flow nasal cannula use also seems to be expanding its territory into the adult realm [13], so if you or your RT department don’t regularly use it, consider getting ahead of the curve, you will be thankful you did.
7. The Right Attitude: Really busy EM shifts can be a grind at times. Seeing multiple pediatric patients with the same “viral” something during the middle of winter amidst many “over-concerned” parents can be even more so (especially if it isn’t your “thing”). This, like many things in life, requires a paradigm shift in order not to grind yourself into burn-out. Whether it fits into what we think of as a classic “Emergency Physician” or not, a huge part of what we do is reassurance and education. It’s not quite as glamorous as that great intubation in the difficult airway, or that chest tube in the hemothorax, but it will always be a cornerstone of what we are as Emergency physicians. Before you go into yet another room of worried parents of the non-toxic, febrile child with a runny nose and cough I would ask you to pause. Remember, kids are the best patients! They rarely fake anything, and rarely try to “tough it out” at home until it’s too late. They are the most honest and sincere patients you will have during your shift. They have a paucity of vices (no smokers, drinkers, or drug seekers). Also think about the fact that these parents are very worried about the most important thing to them in their entire life. They are here for you and your team to evaluate and care for their child. That in and of itself is extremely cool. I will argue that if you keep these things and mind, your shift will be more joyful, fulfilling, and less exhausting. Oh yeah, and don’t forget to catch the actual sick ones.

Hopefully you are already using some of these “hacks” or techniques in your department. Hopefully you learned something as well. Until next time, enjoy those kids!
References:
- Schacherer NM et al Expedited Delivery of Pain Medication for Long-Bone Fractures Using an Intranasal Fentanyl Clinical Pathway Pediatric Emergency Care 2015 Apr 14. [Epub ahead of print] PMID:25875994
- Lane RD et al Atomized intranasal midazolam use for minor procedures in the pediatric emergency department. Pediatr Emerg Care. 2008 May;24(5):300-3. PMID:18496113
- Thakker A et al A randomized controlled trial of intranasal-midazolam versus intravenous-diazepam for acute childhood seizures. J Neurol. 2013 Feb;260(2):470-4. PMID:22983456
- Singer AJ et al Pretreatment of lacerations with lidocaine, epinephrine, and tetracaine at triage: a randomized double-blind trial. Acad Emerg Med. 2000 Jul;7(7):751-6. PMID:10917323
- Klein EJ et al A randomized clinical trial comparing oral, aerosolized intranasal, and aerosolized buccal midazolam. Ann Emerg Med. 2011 Oct;58(4):323-9. PMID:21689865
- Luck R et al Comparison of cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations. Pediatr Emerg Care. 2013 Jun;29(6):691-5., PMID: 23714755
- Singer AJ et al. Ceruminolytic effects of docusate sodium: a randomized, controlled trial Ann Emerg Med. 2000 Sep;36(3):228-32. PMID:10969225
- Fonseca BK et al Enteral vs intravenous rehydration therapy for children with gastroenteritis: a meta-analysis of randomized controlled trials. Arch Pediatr Adolesc Med. 2004;158(5):483. PMID 15123483
- Spandorfer PR et al Oral versus intravenous rehydration of moderately dehydrated children: a randomized, controlled trial. Pediatrics. 2005;115(2):295. PMID: 15687435
- Mayfield S et al High-flow nasal cannula therapy for respiratory support in children. Cochrane Database Syst Rev. 2014 Mar 7 PMID: 24604698
- Bratton SL et al Critical care for pediatric asthma: wide care variability and challenges for study. Pediatr Crit Care Med. 2012 Jul;13(4):407-14 PMID: 22067984
- Shibata S et al Patient origin is associated with duration of endotracheal intubation and PICU length of stay for children with status asthmaticus. J Intensive Care Med. 2014 May-Jun;29(3):154-9 Epub 2013 Feb PMID: 23753230
- Frat JP et al Sequential application of oxygen therapy via high-flow nasal cannula and noninvasive ventilation in acute respiratory failure: an observational pilot study. Respir Care. 2015 Feb;60(2):170-8. doi: 10.4187/respcare.03075. Epub Oct 7 PMID: 25294935
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post 7 Pediatric Hacks for Your ED appeared first on REBEL EM - Emergency Medicine Blog.