
 Background: Based on the Surviving Sepsis Campaign, hemodynamic resuscitation of sepsis patients is done by repeating serum lactic acid levels every 2 – 4 hours until normalization. The issue with this strategy is that there are other things that may elevate lactate levels other than sepsis and hypoperfusion. Another, potentially useful marker to guide hemodynamic resuscitation could be capillary refill time. Its easy-to-use, requires no resources, and costs nothing. To answer this question the ANDROMEDA-SHOCK randomized controlled trial tried to evaluate the use of a peripheral perfusion-targeted resuscitation strategy during septic shock in adults.
Background: Based on the Surviving Sepsis Campaign, hemodynamic resuscitation of sepsis patients is done by repeating serum lactic acid levels every 2 – 4 hours until normalization. The issue with this strategy is that there are other things that may elevate lactate levels other than sepsis and hypoperfusion. Another, potentially useful marker to guide hemodynamic resuscitation could be capillary refill time. Its easy-to-use, requires no resources, and costs nothing. To answer this question the ANDROMEDA-SHOCK randomized controlled trial tried to evaluate the use of a peripheral perfusion-targeted resuscitation strategy during septic shock in adults.
What They Did:
- Determine if peripheral perfusion-targeted resuscitation during early septic shock in adults is more effective than lactate level-targeted resuscitation for reducing mortality
- Multicenter, randomized controlled trial at 28 ICUs in 5 countries (Argentina, Chile, Colombia, Ecuador, Uruguay)
- Study intervention period was 8 hours
- Normalizing capillary refill = applying firm pressure to ventral surface of right index finger distal phalanx with a glass microscope slide. Pressure increased until skin was blanched and then maintained for 10 seconds. The time for return for normal skin color was registered with a chronometer (Time ≥3 seconds = abnormal) assessed every 30 minutes
- Normalizing or decreasing lactate >20%/2hrs
- Study Protocol:
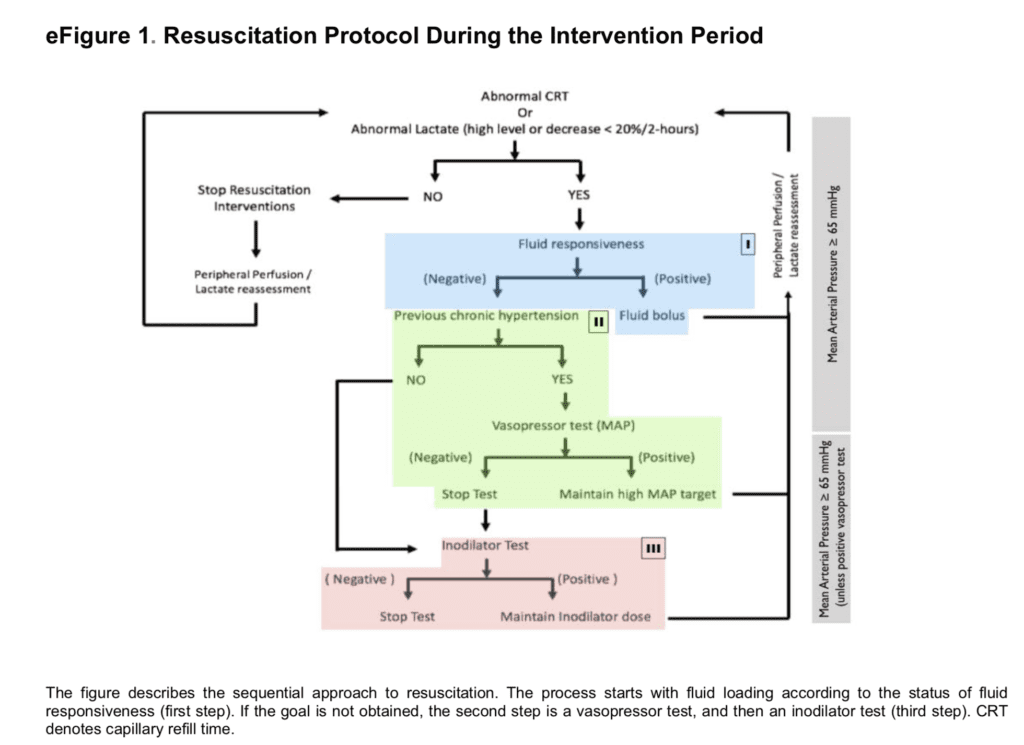
Some Thoughts on this Protocol:
- Fluid Responsiveness (Blue Box): A fluid bolus of 20cc/kg of intravenous fluid is not the standard protocol that CMS requires those of us in the USA to give, which is 30cc/kg. However, these authors did an amazing job checking fluid responsiveness first to ensure an appropriate amount of fluids were given to septic shock patients. Their protocol assessed fluid responsiveness followed by fluid challenges with 500cc of crystalloids every 30 minutes in fluid responders until the goal MAP was achieved as assessed depending on the allocated group (i.e. CRT vs lactate).
- Chronic Hypertension (Green Box): In patients with chronic hypertension, if previous interventions did not meet HD goals (MAP ≥65mmHg), a vasopressor test was conducted by steadily increasing norepinephrine dose until reaching a MAP of 80 – 85mHg, followed by reassessment depending on the allocated group (i.e. CRT vs lactate). If MAP goal was met, then this was the maintained MAP throughout the intervention period. Otherwise if MAP goal not achieved, norepinephrine was decreased to the previous dose and an inodilator test was performed. In my practice, instead of performing a vasopressor test, I instead starting norepinephrine infusion, and if hemodynamic goals are not achieved, next add vasopressin 0.04U/min).
- Inodilator Test (Red Box): This was performed with low dose milronone or dobutamine, depending on local protocols, and patients re-assessed again depending on allocated group (i.e. CRT vs lactate). If HD goals were not met or a safety issue arose, the inodilator was discontinued. In my practice, I am not performing an inodilator test, but If hemodynamic goals are not achieved by the first two steps, I am then a repeating an echo to see if the patient needs inotropic support with either epinephrine or dobutamine.
Outcomes:
- Primary: All-cause mortality at 28days
- Secondary:
- Organ dysfunction at 72hrs after randomization (assessed by SOFA score)
- Death within 90 days
- Mechanical ventilation free days
- Renal replacement therapy
- Vasopressor-free days within 28 days
- ICU and hospital LOS
Inclusion:
- Consecutive patients ≥18 years with septic shock admitted to the ICU
- Septic Shock = Suspected or confirmed infection, plus lactate ≥2.0mmol/L and vasopressor support to maintain MAP ≥65mmHg after IV fluid load of at least 20mL/kg over 60min
Exclusion:
- Hemorrhage
- Severe ARDS
- DNR status
Results:
- 424 patients randomized
- 416 patients completed trial
- All-Cause Mortality:
- Cap Refill Arm: 74 patients (34.9%)
- Lactate Clearance Arm: 92 patients (43.4%)
- HR 0.75
- 95% CI 0.55 – 1.02
- P = 0.06
- Organ Dysfunction at 72 Hours:
- Cap Refill Arm: mean SOFA 5.6
- Lactate Clearance Arm: mean SOFA 6.6
- P = 0.45
- No significant differences in the other secondary outcomes, however in the exploratory analyses there was a clinical trend toward less fluids at 8 hours (Mean: 2359cc vs 2767cc)
Strengths:
- Randomized, multicenter, clinical trial
- Fluid administration based on assessing fluid responsiveness
- Study protocol was operationalized, in a stepwise fashion, using recommended current best evidence guidelines and/or consensus/expert recommendations
- Study cohort enrolled over 1 year
- Complete follow up for primary outcome
- Well balanced cohort of patients
- Protocol adherence was good with protocol violations in 13.7% of CRT arm and 10.8% in lactate arm.Although this could alter results of the study, it does show that the protocol can be adhered to in ≈90% of cases
Limitations:
- Non-blinded study, potentially causing provider bias. Providers could make diagnostic and therapeutic decisions while knowing treatment assignment
- May have been underpowered to exclude clinically meaningful differences between groups (i.e. no previous data to perform a power calculation with CRT)
- Randomization not stratified by site, which may have caused imbalances in allocation to the treatment groups within sites
- Protocol used is quite complex
- ICU-based study, therefore does not provide information on the effectiveness of this approach in other settings
- This study does show that CRT-guided resuscitation is at least as good as lactated guided resuscitation. The results of this trial do not prove superiority of CRT vs lactated-guided resuscitation, and therefore will require an externally validated study to prove this fact.
- Significant physician resources needed for frequent capillary refill checks which may limit use in a busy emergency department or ICU
Discussion:
- Most frequent techniques used for fluid responsiveness were pulse pressure variation and passive leg raise with velocity time integral determination (144 patients in each group)
- In the supplementary info a few things worth mentioning (Peripheral Perfusion vs Lactate Group):
- Epinephrine use: 9.9% vs 16.5% (Epinephrine use will drive up lactate via beta-2 stimulation)
- Vasopressor test: 28.8% vs 40.1%
- Thoughts on Lactate from Frank Lodeserto, MD (Twitter: @FrankLodeserto)
- Popular Myth: Lactate is elevated due to anaerobic metabolism; therefore, we often try to increase oxygen delivery and perfusion to tissue, and in the process, of trying to normalize lactate, we may do more harm by over-resuscitating our patients according to this study
- Lactate is elevated in aerobic metabolism due to beta-2 stimulation and therefore a marker for stress and maybe a useful substrate for tissue energy utilization in shock. With this understanding, we may pay less attention to elevated lactate levels and more attention to important markers of tissue perfusion such as CRT and cause less harm
- In the Jones et al study [2], we saw that the placement of a central line to draw a ScvO2 was as good as lactate clearance. Ironically, in this study we are seeing that CRT may even replace lactate levels. In other words, we are moving to a less invasive resuscitation strategy that is more patient focused rather than lab based and may be less harmful to our patients.
- In the accompanying editorial to this trial, Angus [3], also states that although at the group level interventions may seem similar, at the individual level this may not be the case (i.e. some patients may have received more fluids than others depending on individual needs) but no difference at the group level. He also states this is tough to study.
Author Conclusion: “Among patients with septic shock a resuscitation strategy targeting normalization of capillary refill time, compared with a strategy targeting serum lactate levels, did not reduce all-cause 28-day mortality.”
Clinical Take Home Point: Although the authors conclusion makes it sound like a negative trial, as the gold standard in sepsis is to use lactate and not CRT, this study should be considered a positive trial, as it shows CRT is at least as good as a lactate-guided resuscitation strategy. Using a lactate-guided resuscitation strategy led to more fluid administration, more epinephrine used, and more vasopressors used without improvement in mortality (not statistically significant), compared to normalizing capillary refill time. In other words, with a lactate-guided resuscitation strategy, we are doing more things that don’t make a difference in mortality…Which begs the question…should we be drawing repeat lactates in septic shock?
References:
- Hernandez G et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients with Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA 2019. [Epub Ahead of Print]
- Jones AE et al. Lactate Clearance vs Central Venous Oxygen Saturation as Goals of Early Sepsis Therapy: A Randomized Clinical Trial. JAMA 2010. PMID: 20179283
- Angus DC. How Best to Resuscitate Patients with Septic Shock? JAMA 2019. [Epub Ahead of Print]
For More Thoughts on This Topic Checkout:
- EM Lit of Note: Lactate is Dead! Long Live Lactate?
- EMNerd (EMCrit): The Case of the Deceitful Lantern
- The Bottom Line: ANDROMEDA-SHOCK
- St. Emlyns: JC – The Beauty of Simplicity. ANDROMEDA-SHOCK
Post Peer Reviewed By:Frank Lodeserto, MD (Twitter: @FrankLodeserto) and Rick Pescatore, DO (Twitter: @Rick_Pescatore)
The post ANDROMEDA-SHOCK: Peripheral Perfusion vs Serum Lactate in Septic Shock appeared first on REBEL EM - Emergency Medicine Blog.