
 Background: The American Heart Association/American College of Cardiology (AHA/ACC) give a Class I recommendation for activation of the cardiac catheterization lab in patients with out-of-hospital cardiac arrest (OHCA) whom ST-segment elevation myocardial infarction (STEMI) is present. The evidence for early cardiac catheterization in patients after cardiac arrest, with ROSC and no STEMI is a bit more controversial. The most recent 2015 AHA/ACC guidelines recommend, “it may be reasonable,” to perform an emergent cardiac catheterization in select patients without STEMI.
Background: The American Heart Association/American College of Cardiology (AHA/ACC) give a Class I recommendation for activation of the cardiac catheterization lab in patients with out-of-hospital cardiac arrest (OHCA) whom ST-segment elevation myocardial infarction (STEMI) is present. The evidence for early cardiac catheterization in patients after cardiac arrest, with ROSC and no STEMI is a bit more controversial. The most recent 2015 AHA/ACC guidelines recommend, “it may be reasonable,” to perform an emergent cardiac catheterization in select patients without STEMI.
What They Did:
- Systematic review and meta-analysis of post-cardiac arrest patients without STEMI taken to cardiac catheterization lab
Outcomes:
- What percentage of patients with OHCA, ROSC, and No STEMI on ECG would benefit from emergent cardiac catheterization?
- Acute Myocardial Infarction
- Survival
- Good Neurological Outcome Based on Cerebral Performance Category ≤2 or modified Rankin Score of 0 – 2
Results:
- 1067 Articles Reviewed
- 11 Articles Identified for Analysis
- Sample Sizes of Studies: 84 – 754 Patients
- Odds of Post-Arrest Patients Without STEMI vs STEMI going to Catheterization Lab:
- 4 Trials Reported Results
- No STEMI: 41.5%
- STEMI: 92.5%
- Diagnosis of Acute MI:
- 10 Trials Reported Results
- 1 patient without STEMI diagnosed with AMI for every 10 STEMI patients diagnosed with AMI
- 32.2% (373/1159) of patients without STEMI were diagnosed with a “culprit vessel”
- 71.9% (665/925) of patients with STEMI were diagnosed with a “culprit vessel”
- OR of culprit lesion without STEMI vs STEMI = 0.15 (95% CI 0.06 – 0.34)
- Odds of Having PCI with Placement of Stent in a Culprit Lesion
- 6 Trials Reported Results
- 37.7% of patients without STEMI
- 84.44% of patients with STEMI
- OR 0.14 (95% CI 0.06 – 0.30)
- Survival with Heart Catheterization
- 3 Trials Reported Results
- Combined Data of STEMI + NSTEMI = 3.7 (95% CI 1.31 – 10.70) Higher Odds of Survival
- Patients without STEMI have 30% lower odds of survival compared to those presenting with STEMI (OR 0.65, 95% CI 0.65 – 1.43)
- Survival with Good Neurologic Outcomes
- 2 Trials Reported Results
- No difference in survival with good neurological outcomes between groups (OR 0.65, 95% CI 0.65 – 1.43)
- 2 Trials Reported Results
- 3 Trials Reported Results
- 6 Trials Reported Results
- 10 Trials Reported Results
- 4 Trials Reported Results
Strengths:
- Followed the PRIMSA guidelines for systematic review and meta-analysis
- Comparison of patients with OHCA, ROSC and STEMI vs Non-STEMI
- Manuscripts selected for review were assessed for biases using the Cochrane Review Bias Assessment Tool
Limitations:
- This study looked at both disease-oriented outcomes (i.e. stentable lesions) and patient-oriented outcomes (i.e. mortality). Using placement of a stent as an outcome may not be clinically relevant to morbidity and mortality. It is difficult to establish a link between a “culprit lesion” and a resultant cardiac arrest
- There was a large variance in the methods used to determine which patients would benefit from an emergent cardiac catheterization, and the definition of acute myocardial infarction (i.e. large heterogeneity of trials)
- No prospective randomized trials of PCI in post-cardiac arrest patients without STEMI in this review
- Culprit lesion on angiography was defined as an acute reduction of >50% luminal diameter of a coronary vessel. Some may not consider this a “culprit lesion.”
- Referral bias in many of the studies with patients preferentially brought to centers capable of PCI (i.e. lower threshold to take patients to the catheterization lab post ROSC)
Discussion:
- 1/3 of post OHCA patients without STEMI were found to have a “culprit lesion” causing an acute MI that could potentially benefit from PCI
- The authors were unable to differentiate which patients without STEMI that may benefit from cardiac catheterization vs those who will not based on this review. The authors state: “One should be cautioned to not conclude from this review that all post-arrest patients without STEMI should be taken to emergent cardiac catheterization, but rather conclude that the absence of ST elevation on ECG does not indicated a lack of underlying coronary disease in cardiac arrest patients.”
- In July 2015 the ACC/AHA proposed and published an algorithm to help stratify cardiac arrest patients who are comatose on presentation for emergent cath lab activation for coronary angiography and possible PCI.
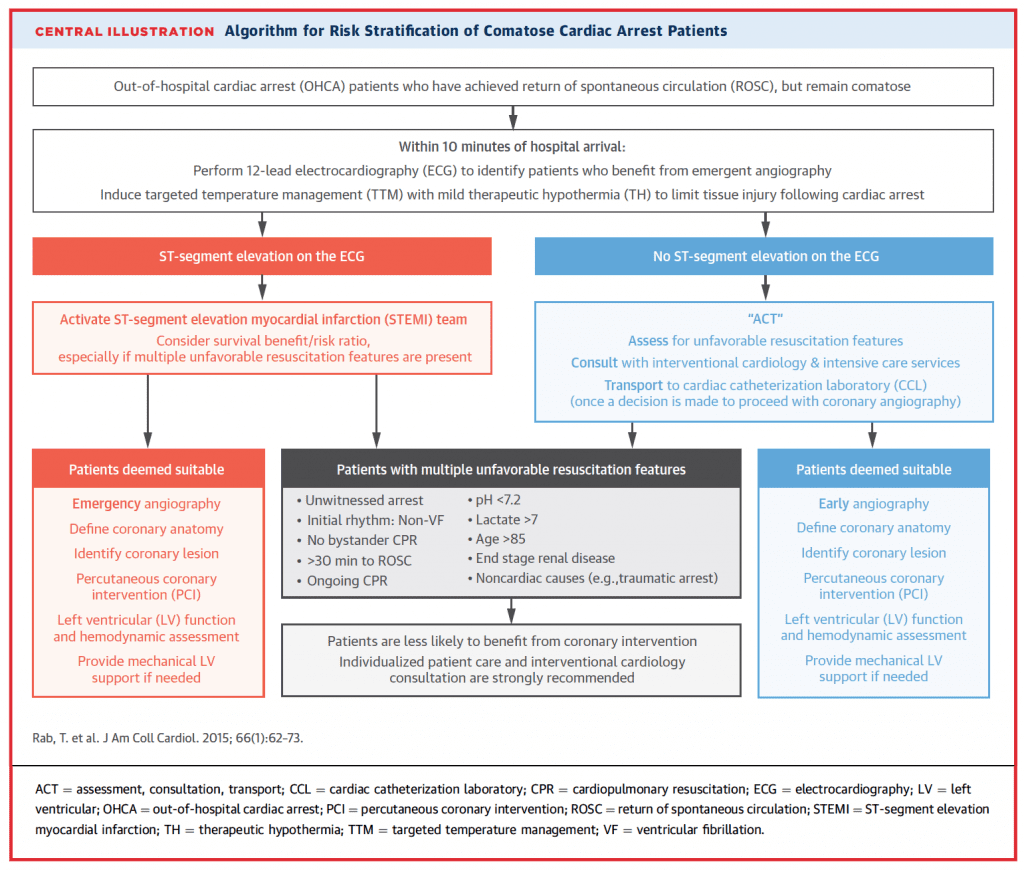
Image from HERE
Author Conclusion: “The results of this systematic review demonstrate that nearly one third of patients who have been successfully resuscitated from cardiopulmonary arrest without ST elevation on ECG have an acute lesion that would benefit from emergent percutaneous coronary intervention.”
Clinical Take Home Point: 1/3 of post OHCA patients without STEMI were found to have a “culprit lesion” causing an acute MI that could potentially benefit from PCI. This study should help start communication with cardiology at your institution to start setting up system wide guidelines of which patients with OHCA, ROSC, and no STEMI on ECG would benefit from emergent cardiac catheterization. Not all patients may benefit from emergent cardiac catheterization, but lack of STEMI on ECG post ROSC does not mean your patient doesn’t have a culprit lesion causing their cardiac arrest
References:
- Millin MG et al. Patients Without ST Elevation After Return of Spontaneous Circulation May Benefit From Emergent Percutaneous Intervention: A Systematic Review and Meta-Analysis. Resuscitation 2016; 108: 54 – 60. PMID: 27640933
For More Thoughts on This Checkout:
- Scott Wieters on REBEL EM: Beyond ACLS: From CPR to Cath – The New ACC/AHA Cardiac Arrest Algorithm
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami) and Scott Wieters (Twitter: @EMedCoach)
The post Cardiac Arrest, Return of Spontaneous Circulation (ROSC) With No ST-Segment Elevation on ECG. Now What? appeared first on REBEL EM - Emergency Medicine Blog.