
 Background: While we try not to think about it, the spectre of litigation hovers around the house of medicine. Medical malpractice books have been written, physicians have found their niche discussing and writing about it and blogs have been started covering this topic and how doctors can better protect themselves and their patients.
Background: While we try not to think about it, the spectre of litigation hovers around the house of medicine. Medical malpractice books have been written, physicians have found their niche discussing and writing about it and blogs have been started covering this topic and how doctors can better protect themselves and their patients.
A 2011 study showed that emergency physicians have a 7.5% annual risk of being involved in a malpractice claim and 1.5% annual risk of a claim being paid either through settlement or verdict (Jena 2011). Physicians who have been involved in claims may practice more defensive medicine leading to more tests which then leads to increasing health care costs.
Previous studies have focused on malpractice risk in EM but they have small sample sizes or focused on specific diseases. One larger study did look at the national dataset but the data is now over a decade old and litigation rates may have changed or increased(Brown 2010).
Clinical Question: What are the factors that are associated with malpractice claims and claim pay outs?
Article: Myers LC et al. Characteristics of Medical Malpractice Claims Involving Emergency Medicine Physicians. J Healthc Risk Manag 2020. PMID: 33078524
Population: Analyzed claims closed between 2007 and 2016, in which one of the following three physician specialties (EM, internal medicine, general surgery) was identified by nurse coders as the “primary responsible provider.” Claims involving family medicine physicians were included in the internal medicine group. Only claims for adult patients.
Outcomes: Factors associated with claim payment
Design: Retrospective cohort study of medical malpractice claims extracted from a national database.
Excluded: Pediatric cases, Non EM, IM, Surgery claims
Primary Results:
- Data from >400 hospitals and >160,000 physicians, representing >30% of all claims in the United States
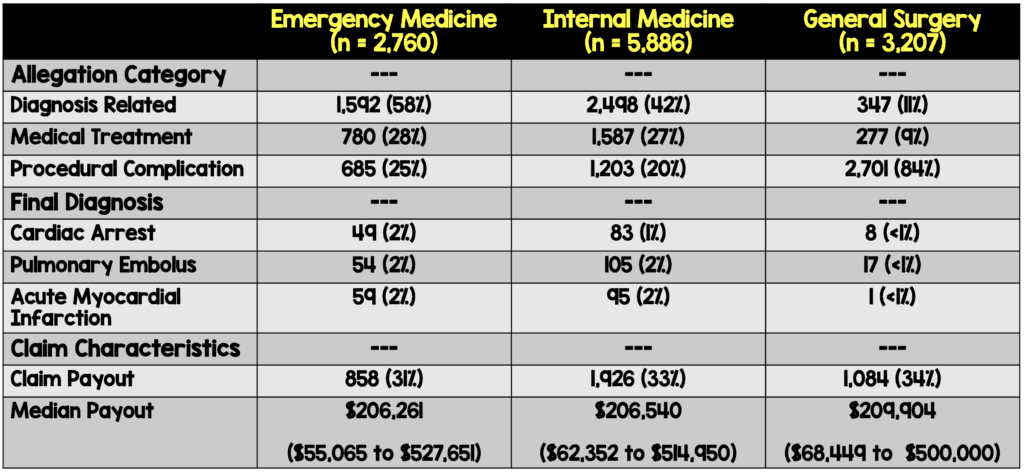
- 54,772 claims, 2,760 claims involved EM physicians, 5,886 involved internists and 3,207 involved general surgeons
Critical Findings:
Strengths:
- Large comprehensive review with over 54,000 claims
- Contextualize information by comparing to other fields
- Looked for results specific for Emergency Medicine
Limitations:
- Information can’t be generalized to overall harmful events since it only looks at malpractice claims.
- Some information in root cause analysis is qualitative, not quantitative. This is an issue because that data does not translate over to the research analysis.
- Nuances related to local standards of care culture and state malpractice that are not captured in a pooled analysis such as this.
- Though covering large dataset, there may be a northeast bias in the data set
Discussion:
- Complications associated with diagnosis are the most common cause of litigation for EM physicians. Second highest is due to complications of treating the illness. What we should ask ourselves is why are we making these mistakes. In a busy and chaotic emergency room we often anchor on a diagnosis which leads to premature closure without having all the data. Are we considering atypical presentations in patients and factoring in whatever previous racial or age bias there may be. We have to take all these things into consideration moving forward when seeing and treating our patients.
- There is a large change from previous literature on what diagnoses are most commonly seen in these cases. Myocardial infarction was previously reported as high as 7.1% of all cases and pulmonary embolism was not listed previously.
- Of procedure-related claims, the most common procedures involving EM physicians were intubation (7%), suturing (5%), and lumbar puncture (3%).
Authors Conclusions:
“In conclusion, we provide granular information related to malpractice risk in EM which we believe may be able to serve as a foundation for preventing future patient harm events related specifically to misdiagnosis and disease-specific domains, such as pulmonary embolism and procedure-related risk.”
Our Conclusions: We tentatively agree with the authors. The data presents the pathologies we are missing but not specifically why we are missing them or what we can do to avoid the misses..
Potential to Impact Current Practice: The data is illuminating in what we are potentially missing but is also lacking in terms of what we can do. While the research is good and a positive step forward, we need further research exploring why we are having these misses.
Bottom Line: Medical malpractice claims involving EM physicians have both a lower odds and rate of payout than the other specialties. The data shows us what pathologies we are missing at high rates but not what factors are leading to those misses.
Guest Post By:
Miguel Reyes, MD
Medical Education Fellow at St. Joseph’s Health
Emergency Medicine
Twitter: @Miguel_reyesMD
Read More:
- Jena AB et al. Malpractice Risk According to Physician Specialty. N Engl J Med 2011. PMID: 21848463
- Brown TW et al. An Epidemiologic Study of Closed Emergency Department Malpractice Claims in a National Database of Physician Malpractice Insurers. Acad Emerg Med. 2010. PMID: 20536812
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Characteristics of EM Malpractice Claims appeared first on REBEL EM - Emergency Medicine Blog.