
 58 y/o female with colorectal cancer recently started on continuous 5-FU chemotherapy presents to the ED with chest pain, shortness of breath, and diaphoresis. The symptoms wax and wane with no specific exacerbating factors. She has no other past medical history, had a port placed recently for her chemotherapy and not a smoker. Initial vital signs are shown below…
58 y/o female with colorectal cancer recently started on continuous 5-FU chemotherapy presents to the ED with chest pain, shortness of breath, and diaphoresis. The symptoms wax and wane with no specific exacerbating factors. She has no other past medical history, had a port placed recently for her chemotherapy and not a smoker. Initial vital signs are shown below…
BP: 146/64 HR: 113 RR: 15 Temp: 98.1 O2 Sat on RA: 100%
Her initial ECG is shown below
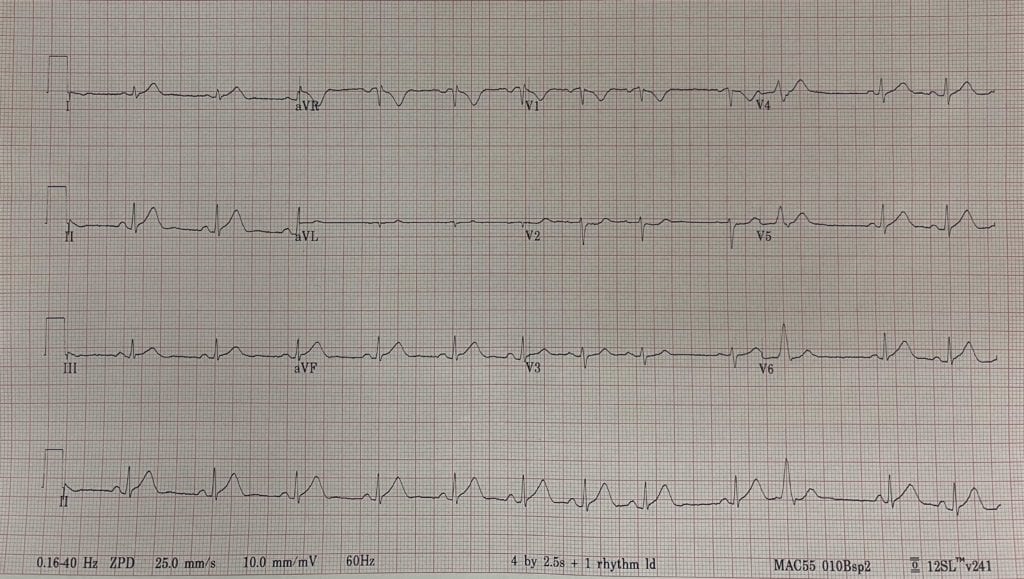
ECG Shows: NSR, hyperacute t waves in the inferior-lateral leads and ST depression in V2
Cardiology was consulted, and recommended medical management with ASA, NTG, and heparin. After receiving SL NTG patients symptoms resolved with the following VS and ECG…
BP: 111/77 HR: 102 RR: 16 Temp: 97.7 O2 Sat on RA: 96%
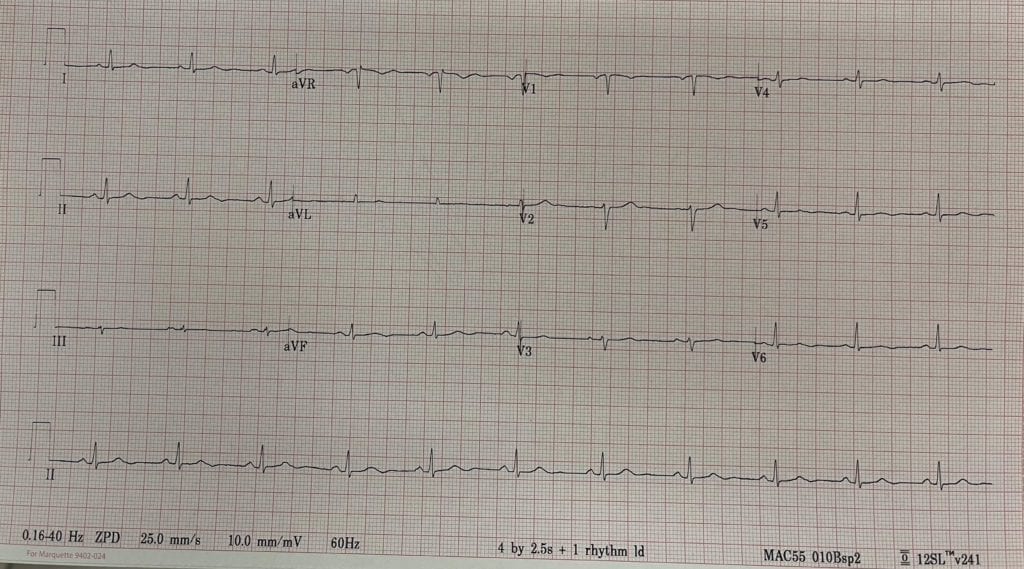
ECG Shows: NSR with resolution of hyperacute T waves and ST depression in V2. Initial conventional troponin I <0.02ng/mL. Due to cancer diagnosis and recent surgery, we performed a CTPA which showed no evidence of PE or other acute abnormalities. After returning from CT patient began having chest pain, shortness of breath, and diaphoresis again with the following vital signs and ECG…
BP: 95/61 HR: 107 RR: 18 Temp: 98.1 O2 Sat on RA: 96%
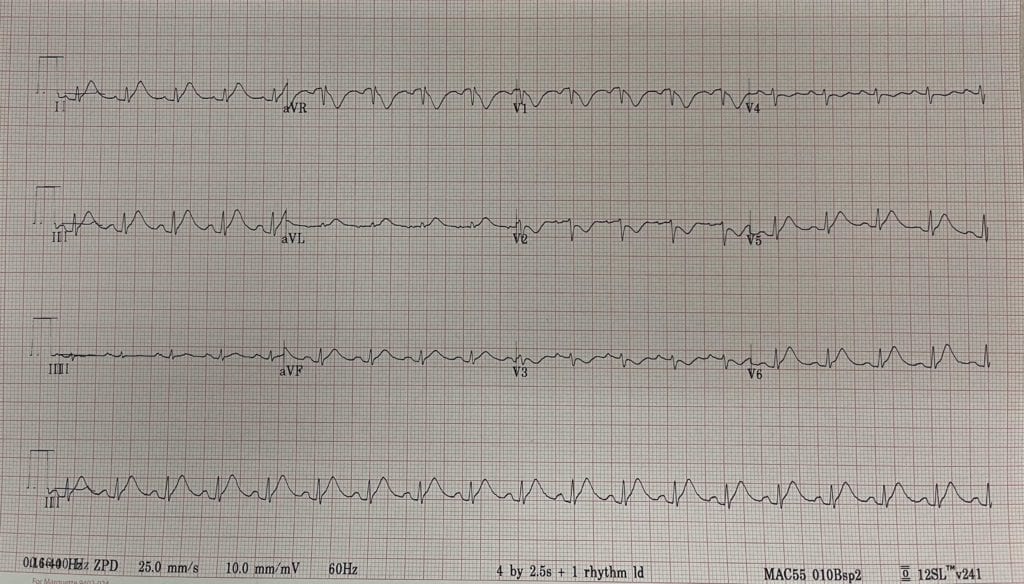
ECG Shows: NSR, with recurrence of hyperacute T waves in inferior-lateral leads and ST depression in V2 – V4. Cardiology contacted again and patient this time taken to the cath lab.
Cath: Angiographically normal epicardial coronaries with no coronary artery disease, right dominant anatomy and normal left ventricular ejection fraction.
So no PE and no OMI. 2nd conventional troponin I also <0.02ng/mL. I started doing some reading and it turns out 5-FU can cause a host of cardiac issues including coronary vasospasm, which is most likely what this patient was suffering from.
5-FU Induced Cardiotoxicity
- Colorectal cancer is the 3rd most common malignancy in both men and women [1]
- 5-FU is an essential component of systemic treatment of colorectal cancer
- 5-FU is the 3rd most commonly used chemotherapeutic agent in the treatment of solid malignancies [2]
- 5-FU is the 2nd most common drug associated with cardiotoxicity after anthracyclines [2]
- Common side effects of 5-FU include:
- Nausea/vomiting
- Stomatitis
- Alopecia
- Myelosuppression
- Diarrhea
- Hand-foot syndrome
- 5-FU can also lead to cardiotoxicity that presents with angina, elevated cardiac enzymes, and ECG changes
- Incidence of 5-FU cardiotoxicity is 1.6 to 19.0% [1, 2]
- Cardiotoxicity tends to occur most commonly during the first cycle of administration [2]
- Time of initiation of symptoms = 12hr – 2d
- Cardiotoxicity can include:
- Chest pain
- ACS
- Arrhythmias
- Myocarditis/pericarditis
- Heart failure
- Coronary vasospasm secondary to 5-FU is rare and thought to be caused by endothelial dysfunction caused by 5-FU
- No definitive test can establish a causal link between 5-FU and cardiotoxicity and thus requires clinical judgement
-
Treatment:
- Stop the 5-FU infusion immediately
- Parenteral nitrates and parenteral or oral calcium channel blockers are used for the treatment of coronary vasospasm
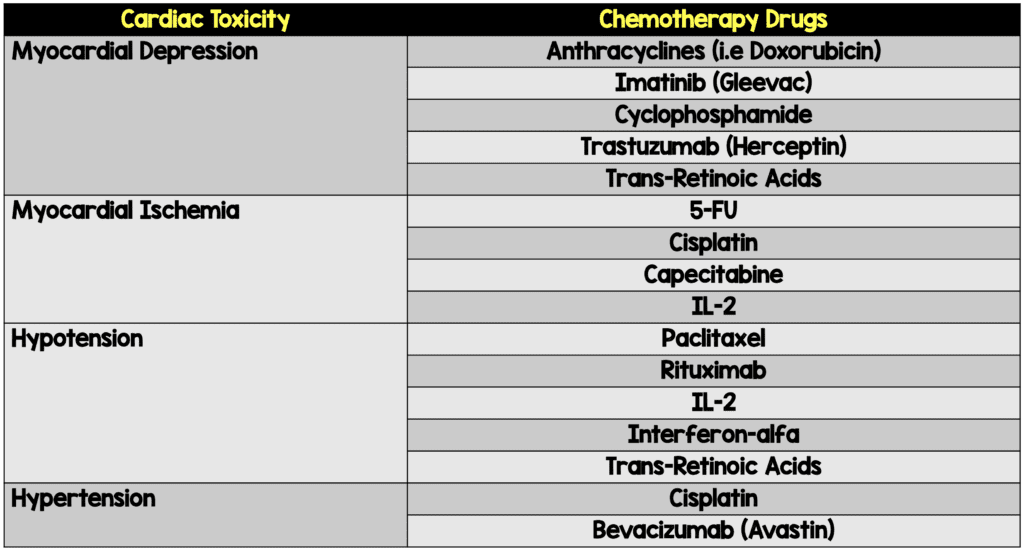
Other Common Chemotherapeutic Agents and Cardiotoxicity (Modified from [3])
References:
- Yildirim M et al. Coronary Vasospasm Secondary to 5-Fluorouracil and Its Management: Case Report. EAJM 2011. PMID: 25610161
- Sara JD et al. 5-Fluorouracila and Cardiotoxicity: A Review. Ther Adv Med Oncol 2018. PMID: 29977352
- Ben-Yakov M et al. Prinzmetal Angina (Coronary Vasospasm) Associated with 5-Fluorouracil Chemotherapy. AJEM 2017. PMID: 28283339
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post Chest Pain and Chemotherapy: 5-FU Induced Coronary Vasospasm appeared first on REBEL EM - Emergency Medicine Blog.