
 Background: Current management of COVID-19 focuses on supportive care as there are yet to be robust, data driven treatments. To date, there has barely been a glimmer of hope based on published evidence, as most studies are either poor quality or demonstrate “negative” results. Two more trials have now been published looking at some new options as potential candidates.
Background: Current management of COVID-19 focuses on supportive care as there are yet to be robust, data driven treatments. To date, there has barely been a glimmer of hope based on published evidence, as most studies are either poor quality or demonstrate “negative” results. Two more trials have now been published looking at some new options as potential candidates.
Paper: Fan-Hgai Hung I et al. Triple Combination of Interferon Beta-1b, Lopinavir-Ritonavir, and Ribavarin in the Treatment of Patients Admitted to Hospital with COVID-19: An Open-Label, Randomised, Phase 2 Trial. Lancet 2020. [Epub Ahead of Print]
Clinical Question: Does the combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin or lopinavir-ritonavir alone help expedite a decrease in time to negative nasopharyngeal swab for SARS-CoV-2?
What They Did:
- Multicenter, prospective, open-label, randomized phase 2 trial in adults with COVID-19 admitted to 6 hospitals in Hong Kong
- Patients randomly assigned (2:1) to:
-
Combination Group: 14d combination of lopinavir/ritonavir 400mg/100mg BID + ribavirin 400mg BID + 3 doses of 8 million IU of interferon beta-1b on alternate days
- For patients recruited and treated between days 7 to 14, interferon beta-1b was omitted
- Control Group: 14 days of lopinavir/ritonavir 400mg/100mg BID
-
Combination Group: 14d combination of lopinavir/ritonavir 400mg/100mg BID + ribavirin 400mg BID + 3 doses of 8 million IU of interferon beta-1b on alternate days
Outcomes:
- Primary: Time to providing a nasopharyngeal swab negative for SARS-CoV-2
-
Secondary:
- Time to resolution of symptoms (NEWS2 of 0 maintained for 24hrs)
- Daily NEWS2 and SOFA score
- Hospital LOS
- 30d Mortality
- Time to achieve negative SARS-CoV-2 in all clinical samples (nasopharyngeal, oropharyngeal, throat, stool, and urine)
- Daily viral load changes in first 7d
- Frequencies and duration of adverse events
Inclusion:
- Age ≥18 years
- Tested positive for COVID-19
- NEWS2 score of at least 1
- Symptom duration of 14d or less upon recruitment
- Admitted to hospital
Exclusion:
- Allergy or severe reaction to study drugs
- Known prolonged QTc syndrome ventricular cardiac arrhythmias, 2nd or 3rd degree heart block, QTc interval ≥480ms
- Taking medications that would interact with lopinavir/ritonavir, ribavirin, or interferon beta-1b
- Known history of severe depression
- Pregnant or lactating women
- Received an experimental agent 1 month prior to recruitment of this study
- History of alcohol or drug abuse in the last 5 years
Results:
- 127 patients recruited
- Median number of days from symptom onset to start of study treatment = 5d
-
Median Time from Start of Study Treatment to Negative Nasopharyngeal Swab:
- Combo Group: 7d (Range 5 to 11)
- Control Group: 12d (Range 8 to 15)
- HR 4.37; 95% CI 1.86 to 10.24; p = 0.0010
- Complete Alleviation of Symptoms (NEWS2 of 0):
- Combo Group: 4d (Range 3 to 8)
- Control Group: 8d (Range 7 to 9)
- HR 3.92; 95% CI 1.66 to 9.23; p ,0.0001
- Complete Alleviation of Symptoms (SOFA score of 0):
- Combo Group: 3d (Range 1 to 8)
- Control Group: 8d (Range 6.5 to 9.0)
- HR 1.89; 95% CI 1.03 to 3.49; p = 0.041
- Median Hospital LOS:
- Combo Group: 9d (Range 7 to 13)
- Control Group: 14.5d (Range 9.3 to 16.0)
- HR 2.72; 95% CI 1.2 to 6.13; p = 0.016
- Combo treatment was associated with significantly shorter time to negative viral load in all specimens (nasopharyngeal, postural oropharyngeal, throat, and stool)
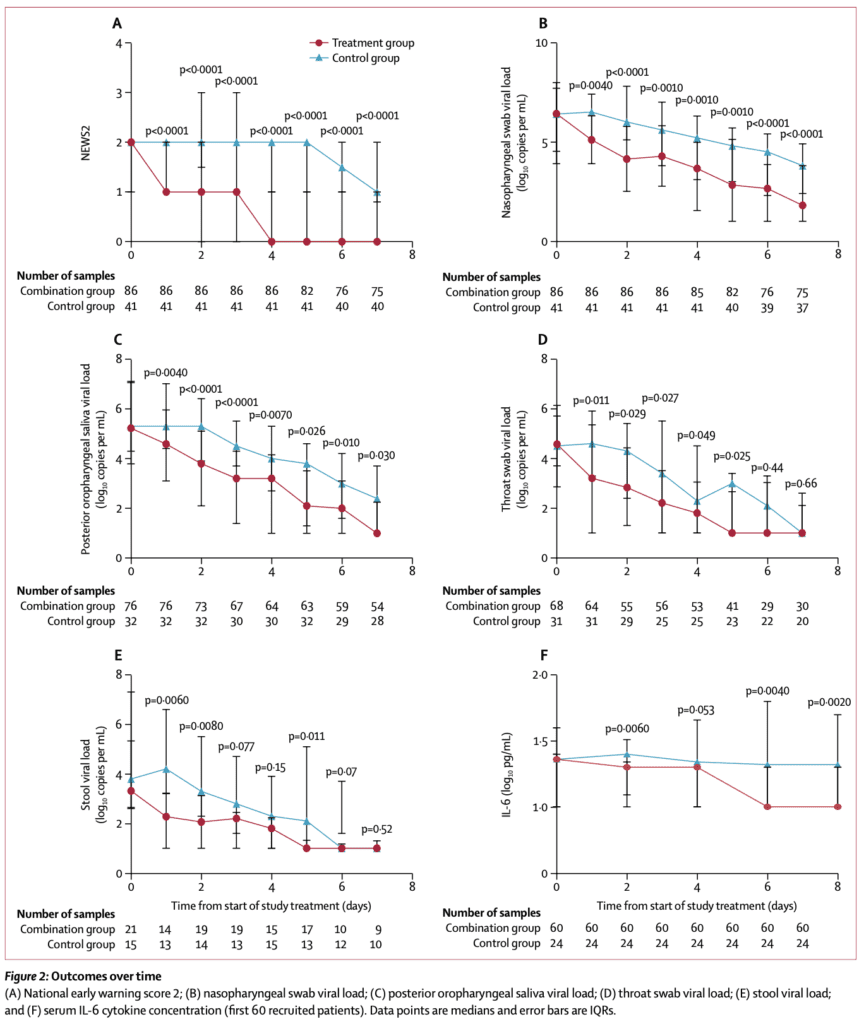
- IL-6 levels were significantly lower in the combo group compared to control group on days 2, 6, and 8
- Adverse Events:
- Combo Group: 48%
- Control Group: 49%
- Most common adverse event was: diarrhea (41%)
- Most adverse events resolved within 3d after drug initiation
- NO serious adverse events in the combo group
- 1 patient in the control group developed biochemical hepatitis from lopinavir-ritonavir
- No patients died during the study
Strengths:
- 1st RCT on triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin, compared with single-drug lopinavir-ritonavir in treatment of patients admitted to the hospital with COVID-19
- Primary outcome is objective, although it is viral clearance. Objective outcomes are preferred especially in an open-label study
- Patients well balanced between groups
- Most patients were admitted to hospital within 7 days of symptom onset, allowing for recruitment into a clinical trial during the early part of COVID-19
- Enrolled consecutive patients
Limitations:
- Based sample size calculation from lopinavir-ritonavir treatment from 2003 SARS-CoV trial, with an estimated difference of 26.4% in the 21d mortality or ARDS rate
- Primary outcome was a disease-oriented outcome (time to negative nasopharyngeal swab), not a patient oriented outcome
- Although the primary outcome is objective in nature it is important to note that RT-PCR testing is only about 75% sensitive so some patients may have had false negative results claiming the treatment as successful clearance when in fact that is not the case. Also, the method of obtaining nasal swabs is important
- Unclear consecutive enrollment of patients
- Open-label study which can bias the results, especially since many of the results are subjective
- No placebo group for comparison
- Unclear if outcome assessors were blinded to treatment allocation
- Confounding results in a subgroup of patients who omitted interferon beta-1b within the combo group
- Absence of critically ill patients, makes it difficult to extrapolate results to an ICU population
Discussion:
- Although the primary outcome was time to negative nasopharyngeal swab, this also seemed to correlate with clinical improvement as shown in the reduction of NEWS2 and duration of hospital LOS. Additionally, the side effect profile seemed generally mild and self-limiting
- IMPORTANT NOTE: This is a relatively well cohort of patients who were treated early in the course of infection with minimal symptoms. If further studies support the results of this trial, the benefit of this drug combination would be in outpatients with mild symptoms which means early capture of patients. These results should not be applied to those patients admitted to the hospital with moderate to severe illness (already in cytokine storm)
- Further studies should elucidate which medication was necessary. Will need large double-blind RCTs
- Patients did well regardless of which treatment arm they were in. This shortened duration which is a useful for two major reasons:
- Reduce transmission (but would need wide use)
- Getting patients back to work, but without testing, are they going back to work without immunity and potentially re-exposed?
- In Hong Kong standard practice is staying in the hospital until nasopharyngeal viral swabs are negative on 2 consecutive days.
- In the combo group, triple therapy was not used in patients who presented 7d or more after symptom onset due to concerns about proinflammatory side effects. Interferon beta-1b is a cytokine, used to help jump start the immune system until anti-viral therapy begins to become effective. It therefore could be potentially detrimental after 7d into illness
Author Conclusion: “Early triple antiviral therapy was safe and superior to lopinavir-ritonavir alone in alleviating symptoms and shortening the duration of viral shedding and hospital stay in patients with mild to moderate COVID-19. Future clinical study of a double antiviral therapy with interferon beta-1b as a backbone is warranted.”
Clinical Take Home Point: Triple antiviral therapy with interferon beta-1b, lopinavir-ritonavir, and ribavirin used early in illness (<7d) seemed to support improvement in the main outcome which was shortening of viral shedding and alleviation of symptoms. These findings also correlated with a faster discharge of patients with mild to moderate COVID-19.
Paper: Cavalli G et al. Interleukin-1 Blockade with High-Dose Anakinra in Patients with COVID-19, Acute Respiratory Distress Syndrome, and Hyperinflammation: A Retrospective Cohort Study. Lancet 2020. [Epub Ahead of Print]
Clinical Question: In patients with COVID-19 on non-invasive ventilation with ARDS, and hyperinflammation, does the addition of anakinra to standard treatment improve clinical outcomes at 21d compared to a historical cohort of patients not receiving anakinra?
What They Did:
- Retrospective cohort study in Italy of consecutive patients with COVID-19
- All patients also received Standard Treatment with:
- Hydroxychloroquine 200mg BID
- Lopinavir/ritonavir 400mg/100mg BID
- Additional Treatment:
- Anakinra 5mg/kg IV BID (high dose)
- Anakinra 100mg BID SQ (low dose)
- Standard Treatment Only + NIV: Mar 10 – 17 (16 patients)
- High Dose Anakinra + NIV + Standard Treatment: Mar 17 – 27 (29 patients)
- Low Dose Anakinra + NIV + Standard Treatment: Mar 10 – 17 (7 patients – terminated after 7 days due to lack of effect on serum CRP and clinical status)
Outcomes:
- Sustained clinical benefit (75% reduction in serum CRP) and sustained respiratory benefit (P/F ratio >200mg) for at least 2d, or until death, bacteremia, or side effects arose (i.e. increase in LFTs > 3x UNL)
- Survival
- Mechanical ventilation free survival
- Change in P/F ratio
- Change in serum CRP
- Clinical status using a 7-point ordinal scale recommended by WHO
Inclusion:
- Age ≥18 years
- Moderate to severe ARDS
- Hyperinflammation (Serum CRP ≥1mg/L, ferritin ≥900ng/mL, or both)
- NIV outside of the ICU
Exclusion:
- Already admitted to ICU for mechanical ventilation
- Evidence of bacterial infection
- Concomitant administration of other anti-inflammatory agents or glucocorticoids
- Enrolled concomitantly in another clinical trial
Results:
-
Before initiation of anakinra:
- Median CRP: 164mg/L
- Median ferritin 1237ng/mL
- All patients on CPAP with median P/F ratio of 77
- 25 (86%) of patients with severe ARDS (P/F ≤100mmHg)
-
7 patients received low-dose SQ anakinra (100mg BID)
- At 7d: no reductions in CRP or in clinical status
- No safety concerns
- Lack of meaningful clinical or anti-inflammatory effects led to early termination
-
29 patients received high dose IV anakinra (5mg/kg BID)
- Median duration of treatment 9d
- Respiratory Function Improvement after 21d
- High Dose anakinra: 21/29 patients (72%)
- Standard Treatment: 8/16 (50%)
- Mechanical Ventilation after 21d:
- High Dose anakinra: 5/29 patients (17%)
- Standard Treatment: 1/16 patients (6%)
- Dead at 21d
- High Dose anakinra: 3/29 (10%)
- Standard Treatment: 7/16 (44%)
- At 21d survival was 90% in high dose anakinra group and 56% in standard treatment group (p = 0.009)
- Mechanical ventilation free survival was 72% anakinra group vs 50% in standard treatment group (p = 0.15)
- Treatment with high dose anakinra was associated with prompt reductions in serum CRP and improvement in P/F ratios over 14d compared to standard care
-
High dose anakinra tolerated in most patients
- Discontinued for adverse events in 7 (24%) of patients after median treatment duration of 9d
- 4 (14%) patients had bacteremia
- 3 (10%) had elevation in LFTs
- Discontinuation of anakinra was not followed by inflammatory relapses
- IMPORTANT NOTE: bacteremia and increased LFTs also occurred in 2 (13%) of patients and 5 (31%) of patients receiving standard treatment respectively
- Discontinued for adverse events in 7 (24%) of patients after median treatment duration of 9d
Strengths:
- Evaluating a medication that targets patients with COIVD-19, hyperinflammation, and ARDS outside the ICU, to prevent death or escalation of care
- Used a sound rationale for use of medication based on pathophysiology
- Groups appear well balanced at baseline
- Reviewed previous evidence to assess effectiveness of high dose IV anakinra
- Evaluated survival and mechanical ventilation free survival (both patient oriented outcomes)
Limitations:
- Retrospective before and after trial with small sample size limit interpretation of results and make it difficult to make definitive conclusions
- There is no a priori primary outcome. This study was part of a larger study which also has no outcomes set (i.e. just descriptive)
- Outcome that is highlighted is not patient centered
- Unclear how patients were selected for participation (i.e. unclear consecutive or convenience enrollment)
- NO blinding since this is not a randomized clinical trial which introduces bias as the outcome assessors were not blinded
- In the conclusion the authors state “safety” of medication, however safety cannot be shown with this small of a study
- Before and after study may have seen improvements in care from one time period to the next as we understood more about the disease, which biases the study to look favorable to the later group
Discussion:
- Anakinra is an interleukin (IL)-1 receptor antagonist that blocks activity of proinflammatory cytokines IL-1alpha and IL-1beta. Pathophysiologically there is a subset of patients with COVID-19 that resemble cytokine storm seen after chimeric antigen receptor T (CAR-T)-cell treatment or patients with macrophage activation syndrome.
- One of the advantages of anakinra is compared to other cytokine-blocking agents it is relatively safe, has a short half-life (3hrs), which allows prompt discontinuation, which is great in critically ill patients
- This trial highlights the importance of not only reducing mortality but preventing ICU admission in a group of patients with COVID-19, on NIV in medical wards. In areas where health systems are overwhelmed, the number of patients with ARDS can exceed the maximum capacity of ICUs, therefore treating patient at an earlier time point in disease could not only decrease mortality, but also decrease need for ICU level of care
Author Conclusion: “In this retrospective cohort study of patients with COVID-19 and ARDS managed with non-invasive ventilation outside of the ICU, treatment with high-dose anakinra was safe and associated with clinical improvement in 72% of patients. Confirmation of efficacy will require controlled trials.”
Clinical Take Home Point: This small retrospective before and after trial of high dose anakinra (5mg/kg IV BID), gives us a proof of concept in the treatment of COVID-19, that should set the stage for replication in larger trials.
References:
- Fan-Hgai Hung I et al. Triple Combination of Interferon Beta-1b, Lopinavir-Ritonavir, and Ribavarin in the Treatment of Patients Admitted to Hospital with COVID-19: An Open-Label, Randomised, Phase 2 Trial. Lancet 2020. [Epub Ahead of Print]
- Cavalli G et al. Interleukin-1 Blockade with High-Dose Anakinra in Patients with COVID-19, Acute Respiratory Distress Syndrome, and Hyperinflammation: A Retrospective Cohort Study. Lancet 2020. [Epub Ahead of Print]
For More Thoughts on This Topic Checkout:
- PulmCrit: High-Dose Anakinra for COVID-19 – The Anti-Inflammatory Trials Begin
- PulmCrit: Virus Wars – Return of Lopinavir/Ritonavir (Along with Ribavirin and Interferon)
- The Bottom Line: Triple Therapy for COVID-19 – A RCT
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)


The post COVID-19: Triple Antiviral Therapy & IL-1 Inhibition appeared first on REBEL EM - Emergency Medicine Blog.