
 There are lots of mixed messages flying around social media about COVID-19 lung injury. Although social media is a very powerful way to get information across, it can also amplify messages that are incorrect or not based in quality research and data. Two pervasive messages have been that COVID19 lung injury is the same as high altitude pulmonary edema (HAPE) and that COVID19 pneumonia is simply typical acute respiratory distress syndrome (ARDS).
There are lots of mixed messages flying around social media about COVID-19 lung injury. Although social media is a very powerful way to get information across, it can also amplify messages that are incorrect or not based in quality research and data. Two pervasive messages have been that COVID19 lung injury is the same as high altitude pulmonary edema (HAPE) and that COVID19 pneumonia is simply typical acute respiratory distress syndrome (ARDS).
MESSAGE #1: COVID19 Lung Injury is NOT HAPE [1]
HAPE
- Excessive and uneven hypoxic pulmonary vasoconstriction
- Increased pulmonary artery pressure in certain regions of the lung
- Increased pulmonary capillary hydrostatic pressure
- Leakage of fluid out of vascular space into alveolar space
-
Treatment: Supplemental O2 alone OR descent to lower elevation (Resolves alveolar and interstitial edema within hours to days)
- Supplemental O2 helps reverse pulmonary vasoconstriction
- Medications such as nifedipine and vasodilators can also help with HAPE (NOT for COVID-19)
COVID-19 Lung Injury
- Viral mediated inflammation
- Alveolar epithelial inflammation/dysfunction
- Impaired surfactant function/alveolar fluid clearance
- Alveolar collapse and/or filling (V/Q mismatch)
- Increased pulmonary artery pressure is a consequence, NOT the cause, of alveolar edema
-
Treatment: Supplemental O2 (Improves hypoxemia but does not resolve underlying inflammation or lung injury)
- In addition positive pressure (CPAP) and awake proning are treatment options as well
MESSAGE #2: COVID19 Pneumonia is ARDS…just not “typical” ARDS [2]
-
Same Virus, Two Phenotypes
- Despite sharing a single etiology (SARS-CoV-2), COVID-19 pneumonia has two distinct presentations:
- This is most likely a time-related spectrum of disease:
-
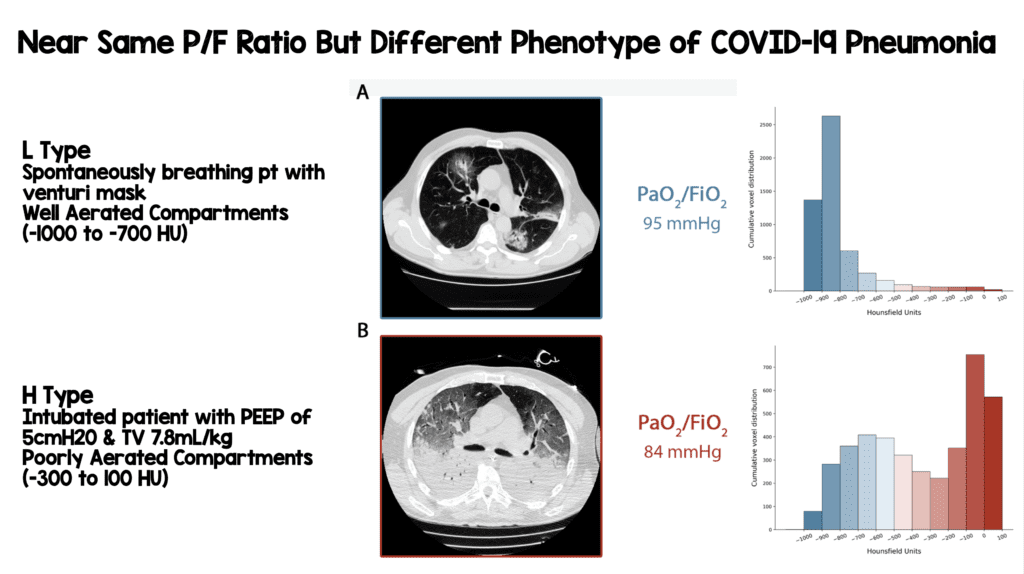
L Type
- Low elastance (i.e. high compliance)
- Low ventilation/perfusion ratio
- Low lung weight
- Low recruitability
- CT scan: well aerated lungs (-1000 to -700 HU)
-
H Type
- High elastance (i.e. low compliance)
- High right-to-left shunt
- High lung weight
- High recruitability
- CT scan: non-aerated lungs (-300 to 100 HU)
-
L Type
- If using the Berlin criteria to define ARDS, COVID-19 lung injury meets the definition. The key difference is lung compliance can often be normal/high (L type) but can progress to low compliance (H type)
- Berlin Criteria:
- Timing: Within 7 days
- Imaging: Bilateral infiltrates
- Origin: Not explained by cardiac failure/fluid overload
- Oxygenation:
- Mild: P/F <200mmHg (≤300 with PEEP/CPAP ≥5cmH20)
- Mod: P/F <100mmHg (≤200 with PEEP/CPAP ≥5cmH20)
- Severe: P/F ≤100mmHg with PEEP ≥5cmH20
- In the image below we see two CT scans of patients with two differing phenotypes however both have a P/F ratio <100mmHg
- Patients with L Type ARDS (High Compliance) need a high FiO2/Lower PEEP strategy
- Patients with H Type ARDS (Low Compliance) should follow the traditional ARDSnet protocol
Take Home Messages:
- COVID-19 lung injury is not HAPE
- COVID-19 pneumonia is ARDS, it’s just not “typical” ARDS
References:
- Luks AM et al. COVID-19 Lung Injury is Not High Altitude Pulmonary Edema. High Altitude Medicine & Biology 2020. PMID: 32281877
- Gattinoni L et al. COVID-19 Pneumonia: Different Respiratory Treatment for Different Phenotypes. Intensive Care Med 2020. [Epub Ahead of Print]
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)

The post COVID-19: Two Important Messages that Need to be Shared Widely appeared first on REBEL EM - Emergency Medicine Blog.