
 Background: Pulmonary embolism is the leading cause of death in pregnancy and the puerperium – accounting for nearly 20% of maternal deaths in the United States – making rapid and accurate diagnosis critically important for emergency physicians, OB/GYNs, and all who take care of these women on a regular basis. Unfortunately, typical diagnostic pathways and approaches may not apply in pregnancy, and are made more complicated by the frequency of concerning and suggestive signs and symptoms in this population, particularly dyspnea (a common symptom in pregnancy related to an increase in progesterone levels) and tachycardia (as resting heart rate is typically expected to increase by up to 25% in normal pregnancy).
Background: Pulmonary embolism is the leading cause of death in pregnancy and the puerperium – accounting for nearly 20% of maternal deaths in the United States – making rapid and accurate diagnosis critically important for emergency physicians, OB/GYNs, and all who take care of these women on a regular basis. Unfortunately, typical diagnostic pathways and approaches may not apply in pregnancy, and are made more complicated by the frequency of concerning and suggestive signs and symptoms in this population, particularly dyspnea (a common symptom in pregnancy related to an increase in progesterone levels) and tachycardia (as resting heart rate is typically expected to increase by up to 25% in normal pregnancy).
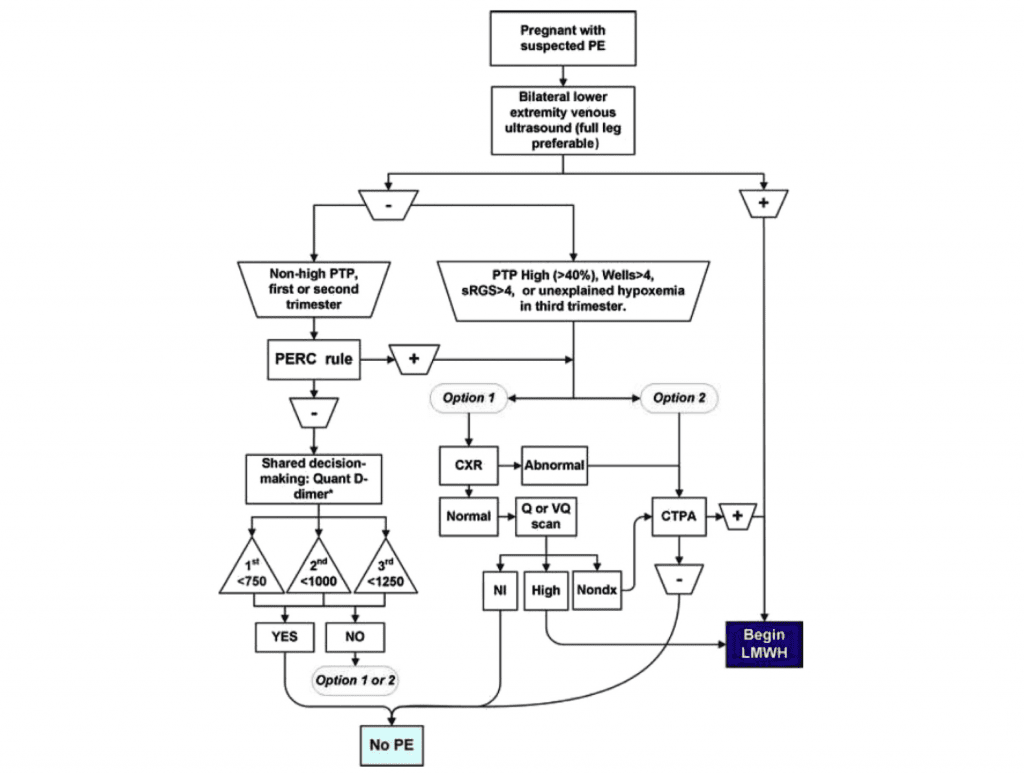
While the use of the D-dimer in conjunction with a low pre-test probability for pulmonary embolism is well established for ruling out PE in the non-pregnant population, the preponderance of evidence to date suggests significant shortcomings with such a strategy in pregnant patients. Indeed, the American Thoracic Society guidelines [1] recommend specifically against the use of D-dimer to exclude PE in pregnancy. Still, though, many emergency physicians have striven for a rational approach to diagnosis—limiting radiation exposure while ensuring safety and sensitivity. The “Kline Algorithm,” as best described in this 2013 podcast on Rob Orman’s venerable ERCast, draws on physiologic expectations and the expertise of Jeff Kline, MD, an emergency medicine physician and expert in venous thromboembolism, to propose a more sensible approach to diagnosis. Unfortunately, literature to support this approach has been sparse. The DiPEP study, published recently in the British Journal of Haematology, attempted to add to this literature base [2].
Kline’s Proposed Algorithm For Exclusion & Diagnosis of PE in Pregnancy [4]
What They Did:
- Prospective observational cohort of 310 pregnant or postpartum women with suspected pulmonary embolism recruited through emergency departments or maternity units at eleven UK hospitals.
- Study population was augmented with 18 pregnant or postpartum women with diagnosed DVT to increase disease prevalence and estimates of biomarker sensitivity.
- Multiple previous investigations have demonstrated the relationship between and consequence of PE from DVT, as well as the similar diagnostic performance of D-dimer in these populations [5].
- Multiple biomarkers including D-dimer were drawn and compared between patients diagnosed with DVT or PE and those in whom VTE was excluded.
- Attempted to answer the question as to whether the sensitivity of D-dimer for VTE was maintained in pregnancy and the puerperium.
Outcomes:
- Primary: Mean biomarker levels, AUROC, and sensitivity and specificity were determined for each biomarker among all pregnant and postpartum women with VTE confirmed by imaging.
-
Secondary:
- Recalculation excluding all women who had received anticoagulant therapy prior to blood sampling.
Inclusion:
- Pregnant and postpartum women 16 years of age and older with suspected PE or diagnosed DVT.
- Suspected PE defined as the treating clinician determining that imaging for PE would be required.
- Length of postpartum period was not defined.
Exclusion:
- Women requiring life support on arrival to hospital.
- Previous PE diagnosed during current pregnancy.
Results:
- 324 women with suspected PE recruited from 11 hospital emergency departments and maternity wards.
- 310 patients with suspected PE included in primary analysis
- Augmented with 18 patients with diagnosed DVT
- 18 patients with PE confirmed by imaging
- 1 subsegmental PE
- 5 patients with clinically diagnosed PE
-
Sensitivity of D-dimer assay for radiographically confirmed VTE at predefined threshold (Primary Outcome)
- ELISA assay ≈ 86%
- INNOVANCE POC assay ≈ 50%
- 240/328 patients received anticoagulation prior to blood sampling
-
Sensitivity of D-dimer assay excluding patients who had received anticoagulant (Secondary Outcome)
- 66 total patients included, only 4 of whom had VTE
- ELISA assay ≈ 50%
- INNOVANCE POC assay ≈ 25%
- No significant difference noted among any of an expanded list of biomarkers.
- BNP, Troponin, CRP, PT, APTT, etc.
Strengths:
- Largest study to date examining the utility of biomarkers for PE in pregnancy and puerperium.
- Though the predicted PE prevalence rate (2%) was very low, augmentation of patients with diagnosed DVT permitted mirroring of the expected rate of VTE in the study population.
- Diagnosis of PE made by independent assessors blinded to D-dimer results.
- D-dimer measured using both ELISA and POC testing to account for real-world variation in testing modalities.
Limitations:
- No information provided as to duration of postpartum period included in study.
- Observational nature prevents utilization of D-dimer based on pre-test probability of disease/risk stratification.
- Cardiac strain (and thus many of the other biomarkers investigated in this study) is likely to be much lower in DVT than PE, making cardiac biomarkers less sensitive in DVT than PE. Study augmentation of patients diagnosed with DVT may have clouded these results.
- The overwhelming majority of patients received anticoagulation prior to blood sampling, severely limiting the applicable patient population for analysis.
Discussion:
- Given the significant limitations of this study, it adds very little to the knowledge base surrounding the use of D-dimer for the evaluation of pulmonary embolism in pregnancy.
- The study highlights the paucity of relevant literature, however, and reminds physicians of guidelines recommending against the use of D-dimer.
- There are three papers highly recommended for reading on this topic:
- Kline JA. D-Dimer concentrations in Normal Pregnancy: New Diagnostic thresholds are Needed. Clinical Chemistry 2005. [3]
- Leung AN et al. An Official American Thoracic Society/Socitey of thoracic Radiology Clinical Practice guideline: Evaluation of Suspected Pulmonary Embolism in Pregnancy. Am J Respir Crit Care Med 2011. [1]
- Kline JA et al. Emergency Evaluation for Pulmonary Embolism, Part 2: Diagnostic Approach. JEM 2015. [4]
Author Conclusion:
“…D-dimer should not be recommended for use in the diagnostic work-up of PE in pregnancy.”
Clinical Take Home Point: Among pregnant women presenting with concern for pulmonary embolism in pregnancy, there remain no data supporting the use of D-dimer in any diagnostic algorithm.
References:
- Leung AN, Bull TM, Jaeschke R, Lockwood CJ, Boiselle PM. Evaluation of Suspected Pulmonary Embolism in Pregnancy. American Journal of Respiratory Critical Care Medicine 2011; 184: 1200-1208. PMID: 22086989
- Hunt, Beverley J., et al. “The DiPEP (Diagnosis of PE in Pregnancy) biomarker study: An observational cohort study augmented with additional cases to determine the diagnostic utility of biomarkers for suspected venous thromboembolism during pregnancy and puerperium.” British journal of haematology (2018). PMID: 29359796
- Kline JA. D-Dimer concentrations in Normal Pregnancy: New Diagnostic thresholds are Needed. Clinical Chemistry 2005. PMID: 15764641
- Kline JA et al. Emergency Evaluation for Pulmonary Embolism, Part 2: Diagnostic Approach. JEM 2015. PMID: 258005245
- Stein, Paul D., et al. “D-dimer for the exclusion of acute venous thrombosis and pulmonary embolism: a systematic review.” Annals of internal medicine 140.8 (2004): 589-602. PMID: 15096330
Post Peer Reviewed By: Salim R. Rezaie (Twitter: @srrezaie)
The post D-Dimer and Pregnancy: The DiPEP Study appeared first on REBEL EM - Emergency Medicine Blog.