
 Background: The mis- and overuse of antibiotics continues to be a growing problem in medicine; the results of which are increased health-care costs, increased antibiotic resistance and, ultimately, patient harm. Unnecessary antibiotics are particularly prevalent in the treatment of lower respiratory tract infections (LRTIs) including asthma exacerbations and bronchitis. While it would be nice to simply stop using antibiotics when they’re not indicated, issues in stewardship abound. Amongst these are legitimate concerns by providers that the patient may have a bacterial infection causing their symptoms and, thus, benefit from a course of antibiotics.
Background: The mis- and overuse of antibiotics continues to be a growing problem in medicine; the results of which are increased health-care costs, increased antibiotic resistance and, ultimately, patient harm. Unnecessary antibiotics are particularly prevalent in the treatment of lower respiratory tract infections (LRTIs) including asthma exacerbations and bronchitis. While it would be nice to simply stop using antibiotics when they’re not indicated, issues in stewardship abound. Amongst these are legitimate concerns by providers that the patient may have a bacterial infection causing their symptoms and, thus, benefit from a course of antibiotics.
Procalcitonin has been touted in recent years as a lab test that can help with this conundrum. Ideally, an elevated procalcitonin level would indicate the presence of a bacterial infection and, thus, suggest benefit from use of antibiotics while a low procalcitonin level would suggest a viral or non-bacterial etiology and suggest an absence of benefit from antibiotics. A recent Cochrane review showed potential for a procalcitonin approach but, there was minimal Emergency Department based evidence.
Article: Huang DT et al. Procalcitonin-Guided use of Antibiotics for Lower Respiratory Tract Infection. NEJM 2018; 379(3): 236-249. PMID: 29781385
Clinical Question: Does a procalcitonin guided approach to antibiotic administration result in lower 30-day antibiotic use in patients presenting with lower respiratory tract infections and an unclear need for antibiotics?
Population: Adult patients (> 18 years old) presenting to the ED with a diagnosis of a LRTI in whom the provider was undecided on whether antibiotics would be given or not.
Outcomes:
- Primary: Total antibiotic exposure (defined as total number of antibiotic-days) within 30 days of study enrollment. Adverse outcomes attributable to withholding antibiotics in LRTI
- Secondary: Prescriptions for antibiotics in the ED, antibiotic receipt by 30 days, antibiotic-days during hospitalization, admission to the ICU, subsequent ED visits within 30 days and quality of life
Intervention: Measuring and reporting procalcitonin assays to the treating clinicians and providing a procalcitonin guideline. Procalcitonin was measured on presentation, 6-24 hours later and on days 3, 5 and 7 if the patient was still in the hospital
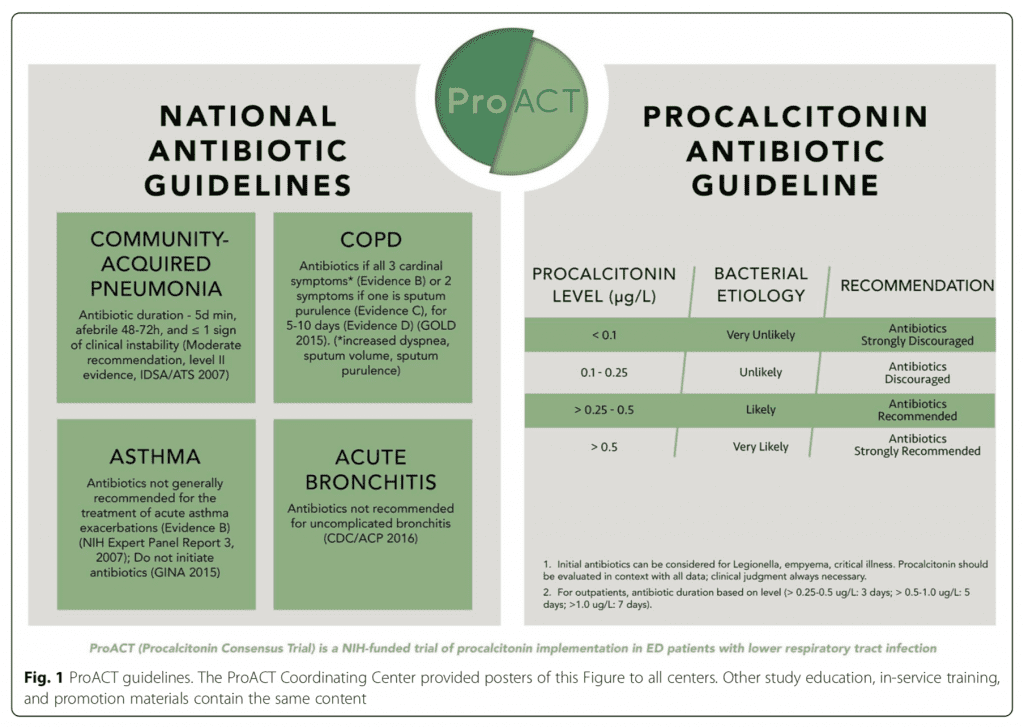
Control: Standard practice (guided by national antibiotic guidelines)
Design: Multicenter, randomized trial in 14 US hospitals
Excluded: Physicians unlikely to withhold antibiotics (prior antibiotic use, vasopressor use, mechanical ventilation, known severe immunosuppression, accompanying non-respiratory infection, known lung abscess/empyema), patient with state where procalcitonin may be elevated in absence of infection (chronic dialysis, metastatic cancer, recent surgery) or follow-up unlikely (i.e. prisoners, homeless)
Primary Results:
- Enrolled patients over 2.5 years
-
8360 patients presented with acute LRTI
- 3540 met exclusion criteria
- 1034 not studied as clinician not willing to consider procalcitonin in decision making
- 2122 excluded for other reasons (logistical issues, patient declined)
-
1664 patients underwent randomization
- Procalcitonin group = 830 (826 analyzed in study)
- Usual care group = 834 (830 analyzed in study)
- Hospitalization: 782 (47.2%)
- Follow up: 1345 patients completed 30-day follow up (81.2%)
- Antibiotics within 30 days: 984 (59.4%)
-
Final diagnoses
- Asthma exacerbation: 39.3%
- COPD exacerbation: 31.9%
- Acute bronchitis: 24.2%
- Community acquired pneumonia: 19.9%
Critical Findings:
-
Antibiotic exposure in 30 days (primary outcome)
- Intention-to-treat analysis
- Procalcitonin 4.2 vs usual care 4.3 mean antibiotic days
- Difference – 0.05 (95% CI -0.7 to 0.6)
- No statistically significant difference
-
Adverse outcome attributable to antibiotic withholding
- Procalcitonin 11.7% vs. usual care 13.1%
- Absolute difference 1.4% (95% CI -4.6 to 1.7)
- Secondary outcomes: no significant difference for any secondary outcome
-
Acute bronchitis antibiotic prescription (subgroup analysis
- Procalcitonin 17.3% vs. usual care 32.1%
- Risk difference – 14.8% (95% CI: – 28.5 to -1.1)
Strengths:
- Study asked an important clinical question
- Multiple European trials have studied procalcitonin-guided care and showed a reduction in antibiotic use in LRTI, with no apparent harms. This is the first multicenter study in the US to evaluate the utility of procalcitonin in the ED
- Randomized, parallel group, 14 center US trial
- At study launch , no center was routinely using procalcitonin, and only 2 centers had procalcitonin clinically available, and no LRTI guidelines recommended, which shows feasibility in centers wanting to start using a procalcitonin guided approach to antibiotic stewardship
- Initial study assumed a 10% loss to follow-up, but at the second interim analysis, the loss to follow-up was 18% so enrollment was increased to 1664 patients to maintain statistical relevance
- bioMerieux (Procalcitonin assay company) provided assay and lab training but played no other role in the trial
- Randomization was appropriately performed (not detailed in study but clear in publication outlining trial design and rationale
- Outcome assessors blinded to study arm
- Baseline characteristics well balanced between groups
- Only recruited patients in whom there was clinical uncertainty in management
- Authors performed both intention to treat and per-protocol analyses and results between the two were similar
Limitations:
- Exclusion criteria limits generalizability: 42% of patients presenting with LRTI were not randomized as they met exclusion criteria
- Nearly 20% of patients were lost to follow up
- Follow up was by chart review and phone calls at days 15 and 30. There is no guarantee that if antibiotics were prescribed, that they were filled or taken
- Due to the nature of the intervention, neither the treating clinician nor the study staff could be blinded to allocation
- Study does not address critical question – is it safe to withhold antibiotics based on a low procalcitonin level?
Discussion:
- Study included multiple sites that did not use procalcitonin in decision making prior to study. If providers were previously using procalcitonin for decision making, taking it away for half the patients may have biased study in favor of procalcitonin group
- The primary outcome was antibiotic use within 30 days. This seems like an odd endpoint for an ED study and, it’s hard for me to imagine how a procalcitonin level on index visit would affect patient care within 30 days. It makes more sense in my mind to look at the difference in antibiotic prescriptions at the index visit.
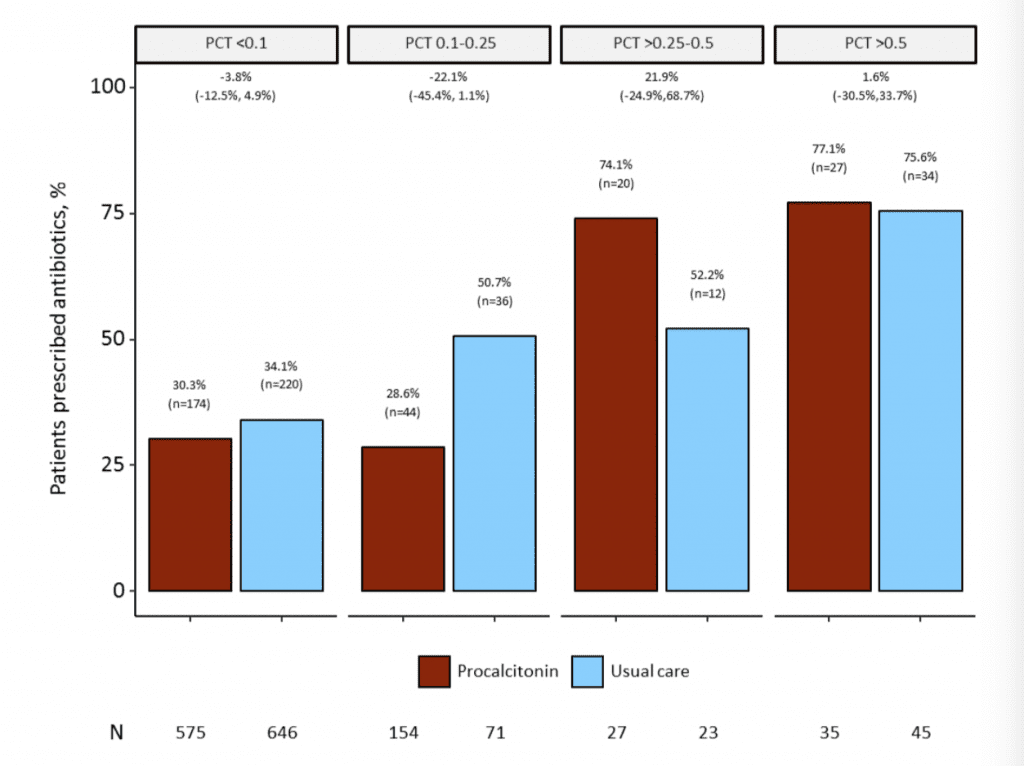
- The authors did report ED antibiotic prescriptions and found a 4.6% non-statistically significant difference between groups. If a larger study found this number to be a true difference, it would represent a substantial antibiotic savings
- There was a significant difference in the prescription of antibiotics in the ED for bronchitis favoring procalcitonin. This subgroup analysis should prompt further investigation
- The authors rolled out their study with a significant investment in education. This represents “a best-case scenario for deployment of a new intervention,” but may not be replicated in non-research settings.
- The centers in this study were all high-performers on national standards. It would be interesting to see if procalcitonin had a larger effect on antibiotic prescribing in hospitals with lower adherence to standards (i.e. Institutions already following best practices may already be paying attention to antibiotic overuse, antibiotic stewardship, and shorter courses of antibiotic treatment).
- Although not statistically significant, if you look at the procalcitonin levels of <0.1 and 0.1 – 0.25 we can see that less antibiotics are prescribed (Almost 50% reduction in the 0.1 – 0.25 tier).
Authors Conclusions:“The provision of procalcitonin assay results, along with instructions on their interpretation, to emergency department and hospital-based clinicians did not result in less use of antibiotics than did usual care among patients with suspected lower respiratory tract infection.”
Our Conclusions: Procalcitonin does not reduce the use of antibiotics in patients presenting to the ED with LRTI in whom it is unclear if antibiotics are indicated. Future studies should investigate shorter term outcomes.
Potential to Impact Current Practice: There is no role for procalcitnonin in ED management of LRTI. Clinicians should continue to base antibiotic treatment on established guidelines and clinical gestalt keeping in mind concepts of antibiotic stewardship.
Bottom Line: Procalcitonin continues to be a test looking for an indication. There is no evidence that procalcitonin is helpful in antibiotic stewardship or in treating patients with LRTI. Thus, it’s use only serves to increase resource utilization without offering improvements in care.
For More on this Topic Checkout:
- REBEL EM: Procalcitonin: Useful Test or Useless Pest to Improve Antibiotic Stewardship with Acute Respiratory Infections in the ED?
- Taming the SRU: Pro’s and Con’s of Procalcitonin
References:
- Schuetz P et al. Procalcitonin to initiate or discontinue antibiotics in acute respiratory tract infections. Cochrane Database Syst Rev 2017. PMID: 29025194
- Huang DT et al. Design and rationale of the Procalcitonin Antibiotic Consensus Trial (ProACT), a multi center randomized trial of procalcitonin antibiotic guidance in lower respiratory tract infection. BMC Emerg Med 2017; 17: 25. PMID: 28851296
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post (Dis)Utility of Procalcitonin in Lower Respiratory Tract Infections (ProACT Trial) appeared first on REBEL EM - Emergency Medicine Blog.