
El uso del torniquete en niños TQ Pediatrico/ Do commercially available tourniquets work on kids? UPDATED May 20 2019
Existe suficiente científica que habla de la eficiencia del torniquete TQ en adultos, pero encontramos pocos datos sobre su uso en niños.
Version 1
En un artículo del Boston Children's Hospital, el director del centro de trauma, David Mooney, MD, habló sobre los dos niños a quienes se aplicaron torniquetes después de los atentados de la maratón de Boston. Los torniquetes demostro ser la diferencia entre salvar vidas o perderlas ese día, y dos niños que sí tenían torniquetes aplicados hoy continuan vivos.
Version 2
Lecciones aprendidas de la transferencia del TCCC Tactical Combat Casualty Care:
Después de los tiroteos de la Escuela Primaria Sandy Hook en 2012, el Colegio Cirujanos de los EUA (ACS) reunió al Comité Conjunto para crear una Política Nacional para mejorar la supervivencia de eventos de Heridos en Masa, que se reunieron en Hartford, Connecticut. Las deliberaciones del comité se conocen como Consensos de Hartford, que esencialmente establecen que;
El sangrado incontrolado en extremidades es la causa prevenible más importante de muerte en el ambiente prehospitalario pudiendo alcanzar un 63%.
Esta formacion esta dirigida a todos los actores que responden profesionales y no profesionales tales como; civiles y fuerzas del orden, para que tengan la educación y el equipo necesario para el control de la hemorragia.
Hartford Consensus apoya firmemente a civiles para que actuen como "respondedores inmediatos".
El Comite Tactical Emergency Tactical Care (C-TECC) fue convocado para acelerar la transición de las lecciones médicas militares aprendidas del campo de batalla a la respuesta civil para reducir las causas prevenibles de muerte tanto por los servicios de emergencias como por la población civil.
TCCC vs TECC
Tactical Emergency Casualty Care (TECC) con un conjunto de pautas de atención de trauma basadas en evidencia para entornos prehospitalarios de alta amenaza para civiles. Las directrices se hicieron a partir de las pautas del TCCC (Tactical Combat Casualty Care).
En resumen, el (TECC) es la evolución civil y la aplicación de las pautas militares de Cuidado de víctimas de combate táctico (TCCC) y el TCCC como sistema, tiene una aplicación limitada en el ámbito civil.
Los niños no se tienen en cuenta en las pautas de TCCC ya que no están en la población militar desplegada. Como tal, el C-TECC examinó específicamente la investigación y los datos específicos de la población pediátrica y creó un conjunto específico de recomendaciones para niños.
Cuidado pediátrico de urgencias tácticas.
Los puntos clave para el paciente pediátrico incluyen;
El proveedor no debe tardar en aplicar torniquetes a víctimas pediátricas
Aplicar el torniquete TQ sobre la ropa lo más proximal como sea posible en la extremidad.
Apriete hasta que cese el sangrado (Desaparezca el pulso distal en la extremidad que hemos aplicado el TQ)
.
En cualquier amputación traumática total o parcial, se debe aplicar el torniquete independientemente del sangrado.
Cuando el tiempo y la situación lo permitan, se debe realizar una prueba de pulso distal en cualquier extremidad donde se aplica torniquete. Si todavía hay pulso distal, considere aprietar mas el torniquete o un segundo torniquete, uno al lado del otro y proximal al primero, para eliminar el pulso distal.
Bibliografía
http://www.c-tecc.org/images/content/FINAL_V.1.0_Pediatric_Guidelines.pdf
Adaptado Dr. Ramon REYES, MD
VP Operacional Comite Iberoamericano de Medicina Tactica y Operacional
Faculty y Medical Director TECC, TCCC
VP Operacional Comite Iberoamericano de Medicina Tactica y Operacional
Faculty y Medical Director TECC, TCCC
Miembro Grupo Internacional Comite TECC
Torniquetes Pediatricos en el Mercado:
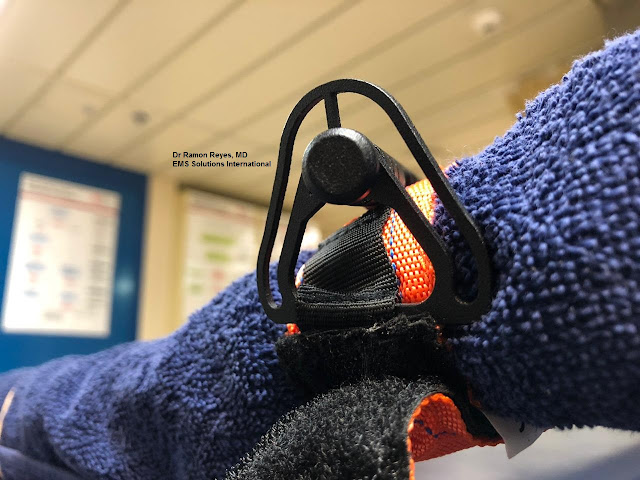
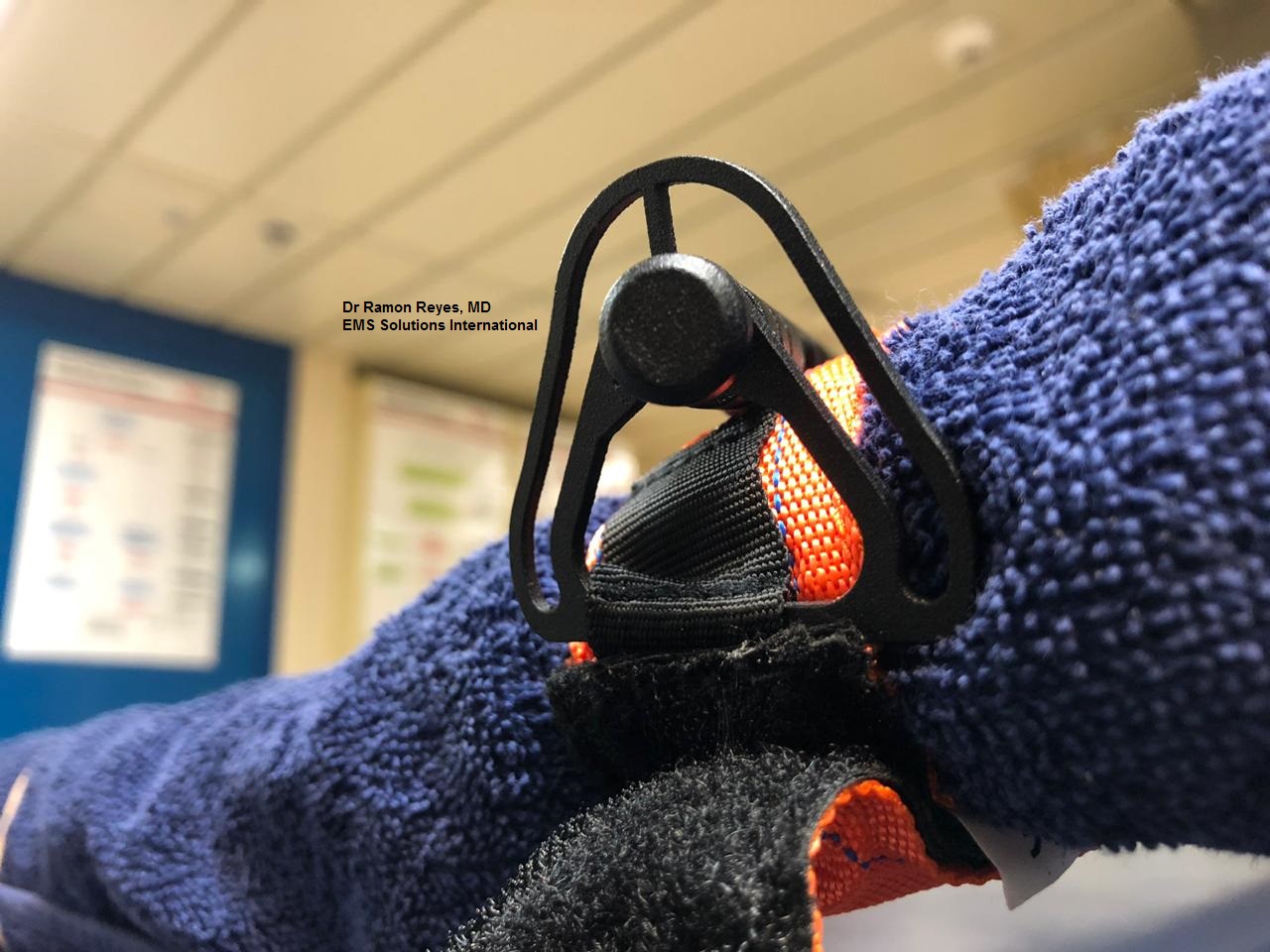
S.T.A.T.® Tourniquet
Pero antes ver estos malos resultados hechos por un profesional de mucho prestigio ante el Comite TECC
Torniquete pediátrico para extremidades pequeñas tanto como unos 20 mm. De fácil aplicación en solo unos 5 segundos.
m2 CHILD Ratcheting Medical Tourniquet EMS World 2015 Top Innovation Award Winner
http://emssolutionsint.blogspot.com/2017/12/m2-ratcheting-medical-tourniquet-rmt.html
Tambien pudiera ser utilizado el Torniquete SOFT
 Do commercially available tourniquets work on kids? UPDATED May 20 2019 by Crisis Medicine
Do commercially available tourniquets work on kids? UPDATED May 20 2019 by Crisis Medicine
Jacob Hall, 6 years old, died of a femoral artery laceration after being shot by a 14-year-old while he was at recess at his school. Another student and a teacher were wounded.








Representamos en exclusiva los Torniquetes 100% Europeos SICH
STRENGTHENED INDIVIDUAL COMBAT HYBRID TOURNIQUET
https://emssolutionsint.blogspot.com/2019/01/tq-tourniquet-sich-strengthened.html
Torniquetes Pediatricos en el Mercado:
S.T.A.T.® Tourniquet
Pero antes ver estos malos resultados hechos por un profesional de mucho prestigio ante el Comite TECC
STAT Tourniquet 21 of 24 applications FAIL by Mike Shertz CRISIS MEDICINE
https://emssolutionsint.blogspot.com/2018/11/stat-tourniquet-21-of-24-applications.html
m2 CHILD Ratcheting Medical Tourniquet EMS World 2015 Top Innovation Award Winner
http://emssolutionsint.blogspot.com/2017/12/m2-ratcheting-medical-tourniquet-rmt.html
Tambien pudiera ser utilizado el Torniquete SOFT

Jacob Hall, 6 years old, died of a femoral artery laceration after being shot by a 14-year-old while he was at recess at his school. Another student and a teacher were wounded.
“’The first-grader lost 75 percent of his blood from a bullet, which pierced his femoral artery in his thigh,’ officials said. He was rushed to Greenville Health System Children’s Hospital, where he had multiple surgeries after going into cardiac arrest.” NBC News, October 2016.
Tragically, Jacob ultimately succumbed to his wounds. No commercially available tourniquets were available at his school, leaving the school nurse with few good hemorrhage control options.
Despite over 10,000 applications and 2,000 lives saved by tourniquet placement during the Global War on Terror, the commercially available tourniquets being used by the Department of Defense were never designed for pediatric use.
Conceptually the two most common of the DOD issued tourniquets, the CAT and SOFT-Wide should work on kids as long as they can adequately circumferentially constrict the limb they are placed on. However, those devices are specified for adult service member limbs, not smaller sized child limbs.
The question becomes will commercially available tourniquets work on kids?
With the recent publication of Dr. Harcke’s study1 using 7th Generation CAT tourniquets on 60 children aged 6 to 16, we have even more data that commercially available tourniquets work just fine on children.
In the study, 7th generation CATs were placed on both the upper arm and thigh of 60 children. The tourniquets were tightened until distal Doppler pulse ceased or the windlass had been twisted 3 full turns (1080 degrees). This limit was chosen to decrease the pain of the tourniquet placement for the study. They acknowledged in actual application pain is irrelevant.
The CATS occluded 100% of the upper extremities and 93% of the thighs. One subject quit during thigh application secondary to pain, and another three could not be occluded despite three twists of the windlass. The three tourniquet applications that failed to occlude were in the oldest (14 to 16 years) age group and were obese.
This is the largest tourniquet study using Doppler ultrasound to verify artery occlusion we are aware of in either adults or children. It is a nice compliment to the previous study by Dr. John Kragh.
Previously, Dr. John Kragh, an orthopedic surgeon and military researcher on tourniquet use, studied 88 children seen in US Military Hospitals in Iraq and Afghanistan on whom US DOD tourniquets were placed. Children ranged in age from 4 to 17 years old. 64% were injured by explosions and 30% gunshot wounds. 7 of the 88 died. They identified no pediatric-specific problems in applying the tourniquets on kids despite the tourniquets being designed for adult casualties. The tourniquets seemed to work on kids just fine.
That is not surprising. Commercial tourniquets are more prone to failure on larger circumference limbs where they cannot fully occlude arterial flow. Placing adult spec’d devices on kids limbs, which are generally much smaller, might actually increase their likelihood of effectiveness. Additionally, kids are generally squishier than adults who may have co-morbidities like calcified and incompressible arteries. All of which should make it easier to occlude a child’s arterial flow.
Once again, the medical literature supports that commercial tourniquets work just fine on children. Now we have one study showing successful application of commercially available tourniquets on kids in a lab setting and another showing similar efficacy in real-world, combat applications.
How young of a kid might the tourniquet work on?
According to the World Health Organization and US CDC, 50% of boys and girls have arm circumferences at least 16.5 to 17.7 cm. There is no specific data on thigh circumference, but the average 6 to 12-month-old American baby is felt to have a thigh circumference of 8 inches / 20 cm. The SOFT Wide circumference is 6.75 inches / 17 cm. The CAT 6th and 7th generation are both about 7.75 inches / 19.5 cm.
What does all this mean?
Dr. Kragh’s study is the only prehospital review on commercial tourniquet use on kids. However, the CAT and SOF-T Wide would be expected to work as tourniquets on thighs as young as 6 to 12 months and arms beginning at about the 5-year-old range.
Just recently, the first case report of a commercially available tourniquet being placed on a child was published. A 7-year-old sustained a femoral artery laceration when a piece of metal flew out of a running lawnmower. Although in shock by the time prehospital providers arrived, he survived after a commercial tourniquet was placed, before transport to the hospital.
What do you do for massive hemorrhage on a kid’s arm too small for a tourniquet? Good clamshell direct pressure. It’s strong enough to occlude arterial flow in an adult male’s arm; it should work easily on a kid.
For an improvised tourniquet using the kid’s own clothing, check out a video using the child’s pants as a tourniquet with a windlass. Works on adults too.
1Harcke HT, Lawrence BA, Gripp HK, et all. Adult Tourniquet Use in School-Age Emergencies. Pediatrics. 2019,143(6)








Representamos en exclusiva los Torniquetes 100% Europeos SICH
STRENGTHENED INDIVIDUAL COMBAT HYBRID TOURNIQUET
https://emssolutionsint.blogspot.com/2019/01/tq-tourniquet-sich-strengthened.html













Pediatric Tactical Emergency Casualty Care
DIRECT THREAT CARE (DTC)
Goals:
1. Accomplish the mission with minimal casualties
2. Prevent any casualty from sustaining additional
injuries
3.
Keep response team maximally engaged in neutralizing
the existing threat (e.g. active shooter, unstable building, confined space
HAZMAT, etc.)
4. Minimize
public harm
Principles:
1.
Mitigate ongoing direct threat (e.g. active fire
fight, unstable building collapse, dynamic explosive scenario, etc.).
2.
Threat mitigation techniques will minimize risk to
casualties and the providers. These should include techniques and tools for
rapid casualty access and egress.
3. Minimal trauma interventions are warranted.
4. Consider
hemorrhage control
a.
TQ application is the primary “medical” intervention
to be considered in Direct Threat Care.
b.
Consider instructing casualty to apply direct pressure
to the wound if no tourniquet available or application is not tactically
feasible.
5. Consider quickly placing or directing casualty to be
placed in position to protect airway.
Guidelines:
1. Mitigate any threat and
move to a safer position (e.g. Return fire, utilize less lethal technology,
assume an overwhelming force posture, extraction from immediate structural
collapse, etc.).
2. Direct the casualty to move to a safer position and
apply self aid if able.
a. Attention must be paid to
the type of instruction that will be presented to this population.
b. Use of tactile direction,
visual signaling and simple language may improve communication.
3.
Casualty Extraction
a. If a casualty can move to safety, they should be
instructed to do so.
b.
If a casualty is unresponsive, the scene commander or
team leader should weigh the risks and benefits of a rescue attempt in terms of
manpower and likelihood of success. Remote
medical assessment techniques should be considered.
c. If the casualty is
responsive but cannot move, a tactically feasible rescue plan should be
devised.
d. Recognize that threats are
dynamic and may be ongoing, requiring continuous threat assessments.
4. Stop life threatening external hemorrhage if
tactically feasible:
a. Provider should not hesitate to apply tourniquets to
pediatric casualties.
b. Apply a tourniquet over the clothing as proximal--
high on the limb-- as possible.
c. Tighten until cessation of
bleeding and move to safety. Consider moving to safety prior to application of
the TQ if the situation warrants.
d. Consider instructing
casualty to apply direct pressure to the wound if no tourniquet available or
application is not tactically feasible
5. Consider quickly placing
casualty, or directing the casualty to be placed, in position to protect airway
if tactically feasible
Skill Sets:
1.
Tourniquet application
2. Consider PACE Methodology- Primary, Alternative,
Contingency, Emergency
3.
Commercially available tourniquets
4.
Field expedient tourniquets
5.
Tactical casualty extraction
6.
Rapid placement in recover position
INDIRECT THREAT CARE (ITC)
Goals:
1. Goals 1-4 as above with DTC care
2. Stabilize the casualty as
required to permit safe extraction to dedicated treatment sector or medical
evacuation assets
Principles:
1. Maintain tactical supremacy, mitigate threats and
complete the overall mission.
2.
Conduct dedicated patient assessment and initiate
appropriate life-saving interventions as outlined in the ITC guidelines. DO NOT
DELAY casualty extraction/evacuation for non life-saving interventions.
3. Consider establishing a casualty collection point if
multiple casualties are encountered
4.
Establish communication with the tactical and/or
command element and request or verify initiation of casualty
extraction/evacuation.
5.
Prepare casualties for extraction and document care
rendered for continuity of care purposes.
Guidelines:
1.
Bleeding:
a. Assess for unrecognized hemorrhage and control all
sources of major bleeding:
i. If not already done, use a
tourniquet for potentially life-threatening bleeding.
i. Apply the tourniquet over
the clothing as proximal-- high on the limb-- as possible. If able and tactical
situation permits, consider fully exposing the wound, applying tourniquet
directly to the skin.
ii. For any traumatic total or
partial amputation, a tourniquet should be applied regardless of bleeding.
ii. Apply pressure dressing
with deep wound packing to control life-threatening external hemorrhage that is
anatomically amenable to such treatment.
b. For compressible hemorrhage
not amenable to tourniquet use, or as an adjunct to tourniquet removal (if
evacuation time is anticipated to be longer than two hours),
apply a hemostatic agent in accordance with the
directions for its use with an appropriate pressure bandage. Before releasing
any tourniquet on a casualty who has received IV fluid resuscitation for
hemorrhagic shock, ensure a positive response to resuscitation efforts (i.e., a
peripheral pulse normal in character and normal mentation).
c. Reassess all tourniquets
that were applied during previous phases of care. Consider exposing the injury.
Tourniquets applied hastily during DTC phase that are determined to be both
necessary and effective in controlling hemorrhage should remain in place if the
casualty can be rapidly evacuated to definitive medical care. If ineffective in
controlling hemorrhage or if there is any potential delay in evacuation to
care, expose the wound fully, identify an appropriate location immediately
proximal to the first tourniquet, and apply a new tourniquet directly to the
skin.
d. When time and the tactical
situation permit, a distal pulse check should be accomplished on any limb where
a tourniquet is applied. If a distal pulse is still present, consider
additional tightening of the tourniquet or the use of a second tourniquet, side
by side and proximal to the first, to eliminate the distal pulse.
e. Expose and clearly mark all
tourniquet sites with the time of tourniquet application.
2.
Airway Management:
a. Unconscious casualty without airway obstruction:
iii. Chin lift or jaw thrust maneuver
iv.
Nasopharyngeal airway
v. Place casualty in the recovery position
vi. Caution advised in patients with suspected C-spine
injury.
b. Casualty with airway obstruction or impending airway
obstruction:
i. Chin lift or jaw thrust maneuver
ii.
Nasopharyngeal airway
iii. Allow casualty to assume
position that best protects the airway- including sitting up
iv. Place unconscious casualty in the recovery position
c.
If previous measures unsuccessful:
i. Airway positioning may be enhanced by elevation of the
shoulders
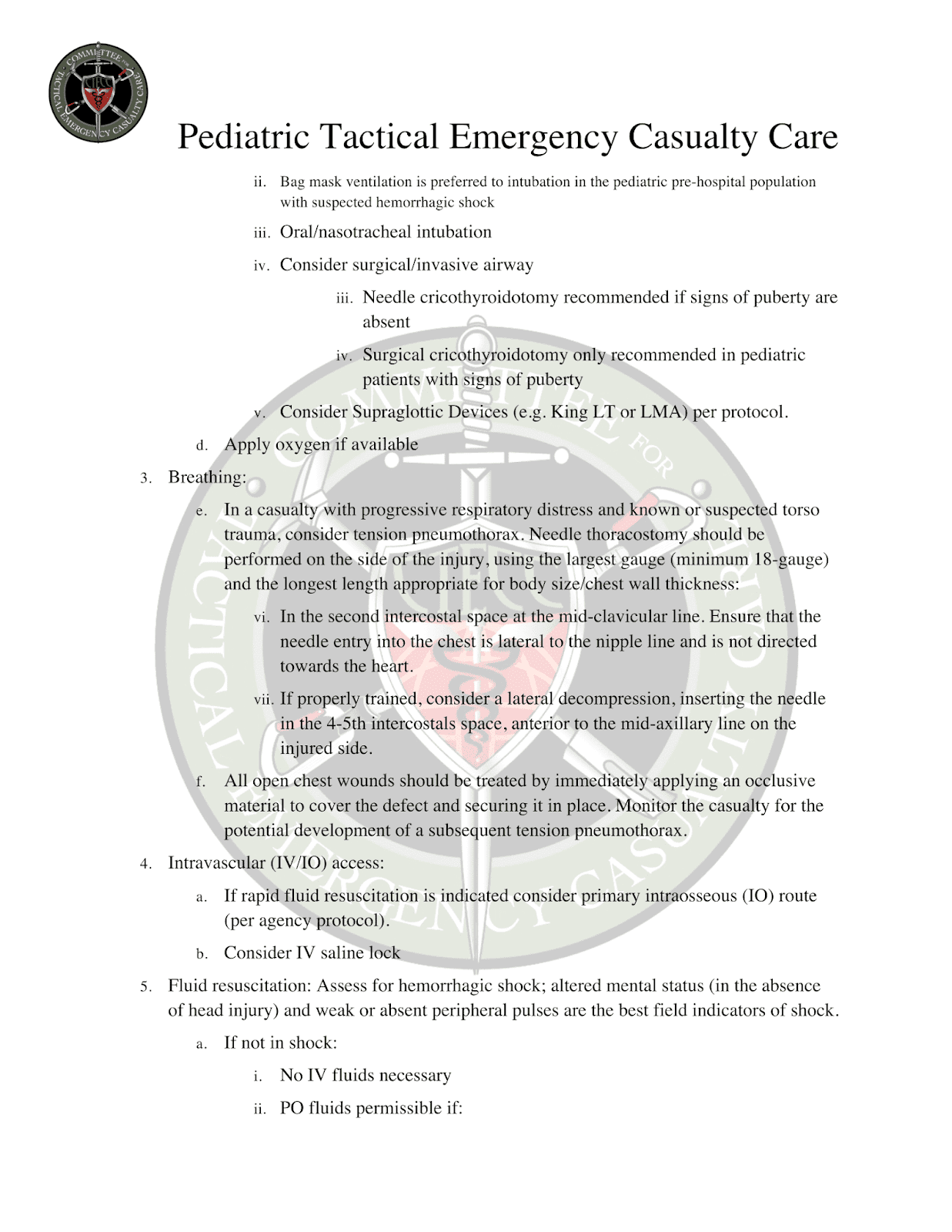
ii. Bag mask
ventilation is preferred to intubation in the pediatric pre-hospital population
with suspected hemorrhagic shock
iii.
Oral/nasotracheal intubation
iv.
Consider surgical/invasive airway
iii. Needle cricothyroidotomy
recommended if signs of puberty are absent
iv. Surgical cricothyroidotomy
only recommended in pediatric patients with signs of puberty
v. Consider Supraglottic Devices (e.g. King LT or LMA)
per protocol.
d.
Apply oxygen if available
3.
Breathing:
e. In a casualty with
progressive respiratory distress and known or suspected torso trauma, consider
tension pneumothorax. Needle thoracostomy should be performed on the side of
the injury, using the largest gauge (minimum 18-gauge) and the longest length
appropriate for body size/chest wall thickness:
vi.
In the
second intercostal space at the mid-clavicular line. Ensure
that the
needle entry into the chest
is lateral to the nipple line and is not directed towards the heart.
vii. If properly trained,
consider a lateral decompression, inserting the needle in the 4-5th
intercostals space, anterior to the mid-axillary line on the injured side.
f. All open chest wounds
should be treated by immediately applying an occlusive material to cover the
defect and securing it in place. Monitor the casualty for the potential
development of a subsequent tension pneumothorax.
4.
Intravascular (IV/IO) access:
a. If rapid fluid
resuscitation is indicated consider primary intraosseous (IO) route (per agency
protocol).
b.
Consider IV saline lock
5. Fluid resuscitation: Assess
for hemorrhagic shock; altered mental status (in the absence of head injury) and
weak or absent peripheral pulses are the best field indicators of shock.
a.
If not in shock:
i.
No IV fluids necessary
ii.
PO fluids permissible if:
v. Conscious, can swallow, and
has no injury requiring potential surgical intervention
vi. If confirmed long delay in evacuation to care
b.
If in shock:
i.
Administer appropriate IV fluid bolus (20cc/kg NS/LR)
and re-assess casualty. Repeat bolus after 30 minutes if
still in shock.
ii. If a casualty with an
altered mental status due to suspected TBI has a weak or absent peripheral
pulse, resuscitate to mid age-specific systolic blood pressure range, or return
of strong peripheral pulse.
6. Prevention of hypothermia
(Note, due to high total body surface area ratio and other physiological variables,
children are at high risk of hypothermia):
c. Initiate all efforts to
eliminate heat loss as soon as operationally feasible, after life-saving
interventions have been employed.
d. Minimize casualty’s exposure to the elements.
e. Replace wet clothing with dry
if possible. Place the casualty onto an insulated surface as soon as possible.
f. Cover the casualty with
commercial warming device, dry blankets, poncho liners, sleeping bags, or
anything that will retain heat and keep the casualty dry.
g. Warm fluids are preferred if IV fluids are required.
7. Penetrating Eye Trauma: If a penetrating eye injury is
noted or suspected:
a. Perform a rapid field test of visual acuity.
b. Cover the eye with a rigid
eye shield (NOT a pressure patch). If a commercial eye shield is not available,
use casualty’s eye protection device or anything that will prevent external
pressure from being applied to the injured eye.
8.
Reassess casualty:
a. Complete secondary survey
checking for additional injuries. Inspect and dress known wounds that were previously
deferred.
b. Consider splinting
known/suspected fracture to include applying pelvic binding techniques for
suspected pelvic fractures.
9.
Provide analgesia as necessary.
a. Consider oral or rectal (if
available) non-narcotic medications such as Tylenol for mild to moderate pain.
b. Avoid the use of
non-steroidal anti-inflammatory medications (e.g. aspirin, ibuprofen, naproxen,
ketorolac, etc) in the trauma patient as these medications interfere with
platelet functioning and may exacerbate bleeding.
c. Narcotic pain medications
should be utilized per protocol. Consider utilization of mucosal atomizer
devices (MAD). Exercise caution when using narcotic medications (e.g. fentanyl
citrate.) and/or Ketamine for moderate to severe pain in pediatric patients due
to their higher volumes of distribution.
i. Consider adjunct administration of anti-emetic
medicines
ii. Have naloxone readily available whenever administering
opiates
iii. Monitor for adverse effects such as respiratory depression
or hypotension.
10. Antibiotics: Consider
initiating antibiotic administration for casualties with open wounds and
penetrating eye injury when evacuation to definitive care is significantly
delayed or infeasible. This is generally determined in the mission planning
phase and requires medical oversight.
11.
Burns:
a. Facial burns, especially
those that occur in closed spaces, may be associated with inhalation injury.
Look for singed nasal hairs or facial hair or soot in and around the nares
which may indicate possible inhalational injury. Aggressively monitor airway
status and oxygen saturation in such patients and consider early definitive
airway management for respiratory distress or oxygen desaturation.
b.
Smoke inhalation, particularly in a confined space,
may be associated with significant carbon monoxide and cyanide toxicity. Patients with signs of significant smoke inhalation plus:
i. Significant symptoms of
carbon monoxide toxicity should be treated with high flow oxygen if available
ii. Significant symptoms of
cyanide toxicity should be considered candidates for cyanide antidote
administration
c. Estimate total body surface
area (TBSA) burned to the nearest 10% using the appropriate locally approved
burn calculation formula.
d. Cover the burn area with
dry, sterile dressings and initiate measures to prevent heat loss and
hypothermia.
e.
If burns are greater than 20% of Total Body Surface
Area, fluid resuscitation should be initiated under medical control as soon as
IV/IO access is established. If
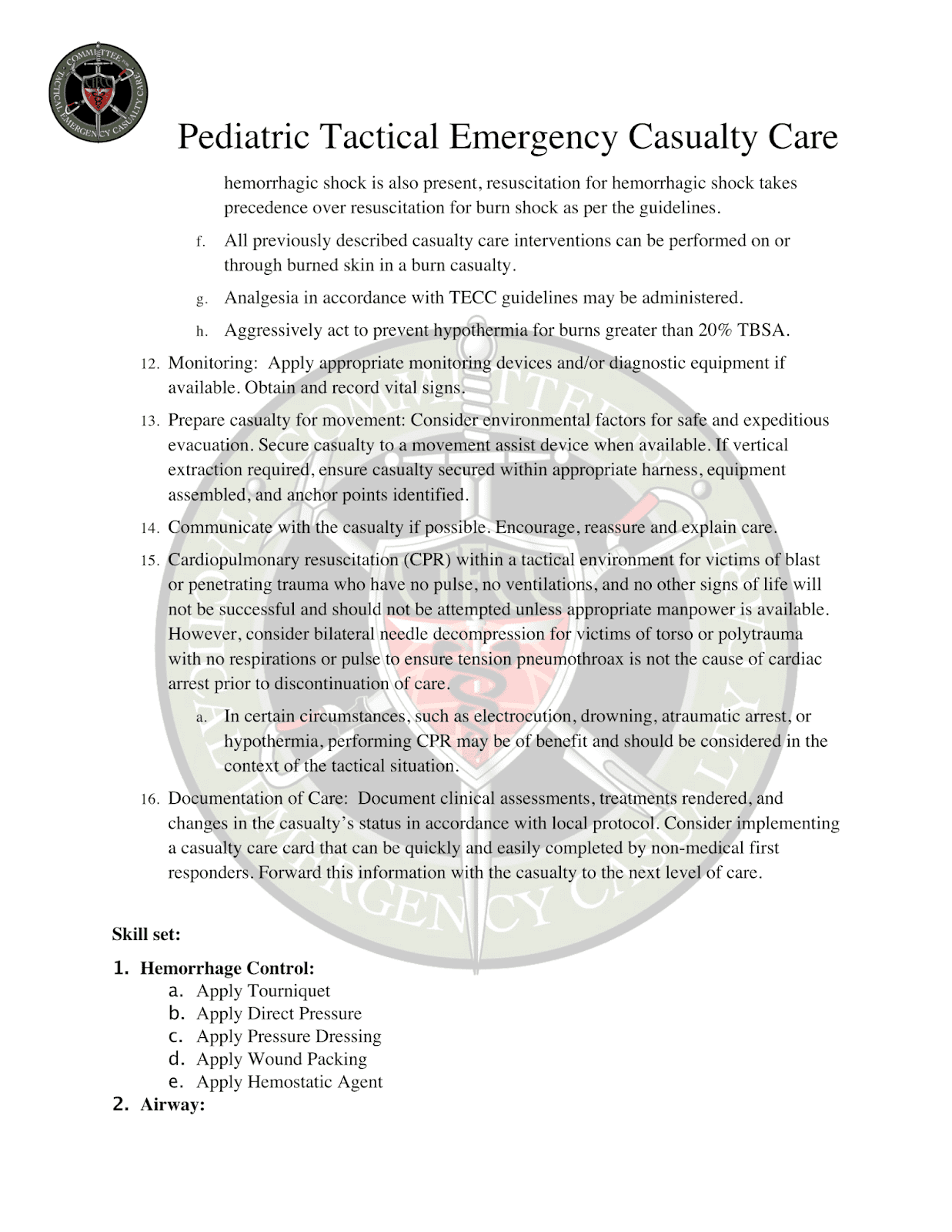
hemorrhagic shock is also
present, resuscitation for hemorrhagic shock takes precedence over
resuscitation for burn shock as per the guidelines.
f. All previously described
casualty care interventions can be performed on or through burned skin in a
burn casualty.
g. Analgesia in accordance with TECC guidelines may be
administered.
h. Aggressively act to prevent hypothermia for burns
greater than 20% TBSA.
12.
Monitoring: Apply appropriate monitoring devices
and/or diagnostic equipment if available. Obtain
and record vital signs.
13. Prepare casualty for
movement: Consider environmental factors for safe and expeditious evacuation.
Secure casualty to a movement assist device when available. If vertical
extraction required, ensure casualty secured within appropriate harness,
equipment assembled, and anchor points identified.
14. Communicate with the casualty if possible. Encourage,
reassure and explain care.
15. Cardiopulmonary
resuscitation (CPR) within a tactical environment for victims of blast or
penetrating trauma who have no pulse, no ventilations, and no other signs of
life will not be successful and should not be attempted unless appropriate
manpower is available. However, consider bilateral needle decompression for
victims of torso or polytrauma with no respirations or pulse to ensure tension
pneumothroax is not the cause of cardiac arrest prior to discontinuation of
care.
a. In certain circumstances,
such as electrocution, drowning, atraumatic arrest, or hypothermia, performing
CPR may be of benefit and should be considered in the context of the tactical
situation.
16. Documentation of Care:
Document clinical assessments, treatments rendered, and changes in the casualty’s
status in accordance with local protocol. Consider implementing a casualty care
card that can be quickly and easily completed by non-medical first responders.
Forward this information with the casualty to the next level of care.
Skill set:
1.
Hemorrhage Control:
a. Apply
Tourniquet
b. Apply
Direct Pressure
c. Apply
Pressure Dressing
d. Apply
Wound Packing
e. Apply
Hemostatic Agent
2.
Airway:
a. Apply Manual Maneuvers (chin lift, jaw thrust,
recovery position, shoulder elevation)
b. Insert
Nasal pharyngeal airway
c. Insert Supraglottic Device (LMA, King-LT, etc)
d. Perform
Tracheal Intubation
e. Perform Surgical Cricothyrotomy (Not recommended for
under 10 yrs)
f. Perform
Needle Cricothyrotomy
3.
Breathing:
a. Application of effective occlusive chest seal
b. Assist Ventilations with Bag Valve Mask
c. Apply
Oxygen
d. Apply
Occlusive Dressing
e. Perform
Needle Chest Decompression
4.
Circulation:
a. Gain
Intravascular Access
b. Gain
Intraosseous Access
c. Apply
saline lock
d. Administer IV/IO medications and IV/IO fluids
e. Administer
blood products
5.
Wound management:
a. Apply Eye
Shield
b. Apply
Dressing for evisceration
c. Apply
Extremity Splint
d. Apply
Pelvic Binder
e. Initiate
Basic Burn Treatment
f.
Initiate
Treatment for Traumatic Brain Injury
6.
Prepare Casualty for Evacuation:
a. Move Casualty (drags, carries, lifts)
b. Apply
Spinal Immobilization Devices
c. Secure
casualty to litter
d. Initiate
Hypothermia Prevention
7.
Other Skills:
a. Perform Hasty Decontamination
a. Initiate
Casualty Monitoring
b. Establish
Casualty Collection Point
c. Perform
Triage
EVACUATION CARE (EVAC):
Goals:
1.
Maintain
any life saving interventions conducted during DTC and ITC phases
2.
Provide
rapid and secure extraction to a appropriate level of care
3.
Avoid
additional preventable causes of death
Principles:
1. Reassess
the casualty or casualties
2.
Rapidly
evacuate patients/casualties is critical
3.
Utilize
additional resources to maximize advanced care
4. Avoid
hypothermia
5.
Communication
is critical, especially between tactical and non tactical EMS teams.
Guidelines:
1.
Reassess all interventions applied in previous phases
of care. If multiple wounded, perform primary triage.
2.
Airway Management:
a.
The principles of airway management in Evacuation Care
are similar to that in ITC with the addition of increased utility of
supraglottic devices and endotracheal intubation.
b. Unconscious casualty without airway obstruction:
i. Chin lift or jaw thrust maneuver
ii.
Nasopharyngeal airway
iii. Place casualty in the recovery position
iv. Caution advised in patients with suspected C-spine
injury
b. Casualty with airway obstruction or impending airway
obstruction:
i. Recovery
position
ii. Naso/oropharyngeal
airway
iii. Airway positioning may be enhance by elevation of
shoulders
iv. Bag mask ventilation is
equivalent to intubation in the pediatric pre-hospital setting
v.
If previous measures unsuccessful, it is prudent to
consider supraglottic Devices (King LT, LMA, etc), endotracheal intubation with
Rapid Sequence Intubation.
vi. Needle cricothyroidotomy recommended if signs of
puberty are absent
vii. Surgical cricothyroidotomy
only recommended in patients with signs of puberty
c.
Following intubation, continuously monitor for ETT
dislodgment, obstruction and equipment failure.
d. If attached to a mechanical
ventilator, consider lung protective strategies and reassess for respiratory
decline in patients with potential pneumothoraces.
e. Use of end-tidal CO2 monitoring is recommended when
available.
f.
Prophylactic hyperventilation is not recommended
3. Breathing:
a.
Reassess casualties who have had chest seals applied
or had needle thoracostomy. If there are signs of continued or progressive
respiratory distress:
i.
Consider repeating needle decompression. If this
results in improved clinical status, the decompression can be repeated multiple
times.
ii. If appropriate provider
scope of practice and approved local protocol, consider placing a chest tube if
no improvement of respiratory distress after decompression if long duration or
air transport is anticipated.
b. All open chest wounds
should be treated by immediately applying an occlusive material to cover the
defect and securing it in place. Monitor the casualty for the potential
development of a subsequent tension pneumothorax. Tension pneumothoraces should be treated as described in ITC.
c.
Administration of oxygen may be of benefit (absent an
environmental risk for fire or explosion) for all traumatically injured
patients, especially for the following types of casualties:
i.
Low
oxygen saturation by pulse oximetry
ii. Injuries
associated with impaired oxygenation
iii. Unconscious
casualty
iv. Casualty with TBI (maintain oxygen saturation >
90%)
v. Casualty
in shock
vi. Casualty
at altitude
vii. Casualties
with pneumothoraces
4. Bleeding:
a.
Fully expose wounds to reassess for unrecognized
hemorrhage and control all sources of major bleeding.
b. If not already done, use a
tourniquet or an appropriate pressure dressing with deep wound packing to
control life-threatening external hemorrhage that is anatomically amenable to
such treatment. For any traumatic total or partial amputation, a tourniquet
should be applied regardless of bleeding.
c.
Reassess all tourniquets that were applied during
previous phases of care. Expose the injury and determine if a tourniquet is
needed.
i.
Tourniquets applied in prior phases that are
determined to be effective in controlling hemorrhage should remain in place if
the casualty can be rapidly evacuated to definitive medical care.
ii. If ineffective in
controlling hemorrhage or if there is any potential delay in evacuation to
care, apply a new tourniquet immediately above the first.
iii. If delay to definitive care
longer than 2 hours is anticipated and wound for which tourniquet was applied
is anatomically amenable, attempt a tourniquet downgrade as described in ITC
(this should be a paramedic or MD action).
iv. A distal pulse check should
be performed on any limb where a tourniquet is applied. If a distal pulse is
still present, consider additional tightening of the tourniquet or the use of a
second tourniquet, side by side and proximal to the first, to eliminate the distal
pulse.
v. Expose and clearly mark all
tourniquet sites with the time of tourniquet application. Use an indelible marker.
5. Fluid
resuscitation:
a.
If casualty displays signs of shock (altered mental
status in the absence of brain injury, weak or absent peripheral pulses, and/or
change in pulse character) resuscitation should be directed towards restoration
of peripheral pulses and improvement of mental status.
b. If BP monitoring is
available, maintain target systolic BP 70mmHg or Mean Arterial Pressure greater
than 60 mm Hg in children under 10 (minimum normal systolic BP = 70 + (Age x
2).
c.
Establish intravascular access if not performed in ITC
phase. Consider primary intraosseous access in Pediatric population
d. Management of resuscitation as in ITC with the
following additions:
i.
If in shock and blood products are not available or
not approved under scope of practice/local protocols resuscitate as in ITC.
ii. If in shock and blood
products are available with an appropriate provider scope of practice under an
approved medical protocol:
1.
Resuscitate with 10-15 cc/kg of plasma (FFP) and 10-15
cc/kg of packed red blood cells (PRBCs) in a 1:1 ratio.
2.
If blood component therapy is not available, and
appropriate training, testing and protocols are in place, consider transfusing
fresh whole blood.
3.
Continue resuscitation as needed to maintain target BP
or clinical improvement.
iii. If a casualty with an
altered mental status due to suspected TBI has a weak or absent peripheral
pulse, resuscitate as necessary to maintain mid age-specific systolic blood
pressure range, or a strong peripheral pulse.
iv. If suspected TBI and
casualty not in shock, raise the casualty’s head to 30 degrees and maintain MAP
> 60mm Hg with volume resuscitation or vasopressor medications, if indicated
and approved under scope of practice/local protocols.
6. Prevention
of hypothermia:
a.
Continue all efforts to eliminate heat loss as
operationally feasible, after life-saving interventions have been employed.
b. Minimize casualty’s
exposure to the elements. Move into a medic unit, warmed vehicle, or warmed
structure if possible. Ensure transport vehicle climate control system does not
worsen hypothermia.
c.
Replace wet clothing with dry if possible. Place the
casualty onto an insulated surface as soon as possible.
d. Cover the casualty with
commercial warming device, dry blankets, poncho liners, sleeping bags, or
anything that will retain heat and keep the casualty dry.
e.
Warm
fluids are preferred if IV fluids are required.
7. Monitoring
a.
Institute electronic monitoring if available,
including pulse oximetry, cardiac monitoring, etCO2 (if assisted ventilation or
altered mental status), and blood pressure.
b. Obtain and record vital signs.
8. Reassess
casualty:
a.
Complete secondary survey checking for additional
injuries. Inspect and dress known wounds that were previously deferred.
b. Determine mode and destination for evacuation to
definitive care.
c.
Splint
known/suspected fractures and recheck pulses.
d. Apply pelvic binding techniques for suspected pelvic
fractures.
e.
Consider the mechanism of injury and the need for
spinal immobilization. Spinal immobilization is not necessary for casualties
with penetrating trauma if the patient is neurologically intact. Patients may
be clinically cleared from spinal immobilization under a locally approved
protocol if they have none of the following:
i. Midline
c-spine tenderness
ii. Neurologic
impairment
iii. Altered
mental status
iv. Distracting
injury
9. Provide
analgesia as necessary.
a. Mild
pain:
i. Consider
oral non-narcotic medications
ii. Avoid the use of
non-steroidal anti-inflammatory medications (e.g. aspirin, ibuprofen, naproxen,
ketorolac, etc) in the trauma patient as these medications interfere with
platelet functioning and may exacerbate bleeding
b. Moderate
to severe pain:
i. Narcotic pain medications
should be utilized per protocol. Consider utilization of mucosal atomizer
devices (MAD). Exercise caution when using narcotic medications (e.g. fentanyl
citrate.) and/or Ketamine for moderate to severe pain in pediatric patients due
to their higher volumes of distribution.
i.
Place patient on appropriate monitor
ii. Consider adjunct administration of anti-emetic
medicines
iii. Have naloxone readily
available whenever administering opiates
iv. Monitor for adverse effects
such as respiratory depression or hypotension.
10.
Burns:
c. Burn care is consistent with the principles described
in ITC.
d.
Smoke inhalation, particularly in a confined space,
may be associated with significant carbon monoxide and cyanide toxicity. Patients with signs of significant smoke inhalation plus:
ii. Significant symptoms of
carbon monoxide toxicity should be treated with high flow oxygen if available
iii. Significant symptoms of
cyanide toxicity should be considered candidates for cyanide antidote
administration
e. Be cautious of off-gassing
from patient in the evacuation vehicle if there is suspected chemical exposure
(e.g. cyanide) from the fire.
f. Consider early airway
management if there is a prolonged evacuation period and the patient has signs
of significant airway thermal injury (e.g. singed facial hair, oral edema,
carbonaceous material in the posterior pharynx and respiratory difficulty).
11. Prepare casualty for
movement: Consider environmental factors for safe and expeditious evacuation.
Secure casualty to a movement assist device when available. If vertical
extraction required, ensure casualty secured within appropriate harness,
equipment assembled, and anchor points identified.
12.
Communicate with the casualty, transporting crew and
with the accepting facility. Encourage, reassure and explain
care to patient and parents.
13. Cardiopulmonary
resuscitation (CPR) may have a larger role during the evacuation phase
especially for patients with electrocution, hypothermia, non traumatic arrest
or near drowning.
a. Consider rescue breaths in
small children with deteriorating cardiopulmonary status.
b. Consider bilateral needle
decompression for victims of torso or polytrauma with no respirations or pulse
to ensure tension pneumothorax is not the cause of cardiac arrest prior to
discontinuation of care.
14. Documentation of Care:
Continue or initiate documentation of clinical assessments, treatments
rendered, and changes in the casualty’s status in accordance with local
protocol. Forward this information with the casualty to the next level of care.


Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/groups/PDFgratisMedicina #DrRamonReyesMD
Facebook
https://www.facebook.com/DrRamonReyesMD
Instagram
https://www.instagram.com/drramonreyesmd/
Pinterest
https://www.pinterest.es/DrRamonReyesMD/
Twitter
https://twitter.com/eeiispain
Blog
http://emssolutionsint.blogspot.com/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html
TELEGRAM
Group https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q

Current recommendations include the use of arterial tourniquets (TQ) in appropiate paediatric trauma patients.
But just how effective are they? The efficacy is less clear.
This study tested 5 different TQ's on two simulated paediatric models, with differing limb diameter replicating various age groups and percentiles.
This study suggested that the test windlass TQs can be applied effectively to upper and lower extremities of children aged 5 years and older in the 50%th percentile for limb circumference. In younger children windlass TQ efficacy is variable.
This study suggests that TQs should remain in use for haemorrhage control in paediatric patients and further evidence is required to better understand the true efficacy.
Have you applied a TQ to a paediatric? Was it effective?
Sweating the Little Things: Tourniquet Application Efficacy in Two Models of Pediatric Limb Circumference.
El-Sherif N1, Lowndes B1, Franz W2, Hallbeck MS1, Belau S3, Sztajnkrycer MD3,4.
Abstract
BACKGROUND:
Current military recommendations include the use of tourniquets (TQ) in appropriate pediatric trauma patients. Although the utility of TQs has been well documented in adult patients, the efficacy of TQ application in pediatric patients is less clear. The current study attempted to identify physical constraints for TQ use in two simulated pediatric limb models.
METHODS:
Five different TQ (Combat Application Tourniquet (CAT) Generation 6 and Generation 7, SOFTT (SOF Tactical Tourniquet), SOFTT-W (SOF Tactical Tourniquet - Wide), SWAT-T (Stretch Wrap and Tuck - Tourniquet) and a trauma dressing were evaluated in two simulated pediatric limb models. Model one employed four cardiopulmonary resuscitation (CPR) manikins simulating infant (Simulaids SaniBaby), 1 year (Gaumard HAL S3004), and 5 years (Laerdal Resusci Junior, Gaumard HAL S3005). Model two utilized polyvinyl chloride (PVC) piping with circumferences ranging from 4.25" to 16.5". Specific end-points included tightness of the TQ and ability to secure the windlass (where applicable).
RESULTS:
In both models, the ability to successfully apply and secure the TQ depended upon the simulated limb circumference. In the 1-year-old CPR manikin, all windlass TQs failed to tighten on the upper extremity, while all TQs successfully tightened at the high leg and mid-thigh. With the exception of the CAT7 and the SOFTT-W at the mid-thigh, no windlass TQ was successfully tightened at any extremity location on the infant. The SWAT-T was successfully tightened over all sites of all CPR manikins except the infant. No windlass TQ was able to tighten on PVC pipe 5.75" circumference or smaller (age < 24 months upper extremity). All windlass TQs were tightened and secured on the 13.25" and 15.5" circumference PVC pipes (age 7-12 years lower extremity, age >13 years upper extremity). The SWAT-T was tightened on all PVC pipes.
DISCUSSION:
The current study suggests that commercial windlass TQs can be applied to upper and lower extremities of children aged 5 years and older at the 50%th percentile for limb circumference. In younger children, windlass TQ efficacy is variable. Further study is required to better understand the limitations of TQs in the youngest children, and to determine actual hemorrhage control efficacy.
© Association of Military Surgeons of the United States 2019. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
KEYWORDS:
Hemorrhage Control; Pediatric; Tourniquet; Trauma
Torniquete SICH en Pediatricos by Dr. Ramon REYES, MD
DESFIBRILADOR AED, DEA, DESA TELEFUNKEN Muerte Subita y Cardioproteccion "Zona Cardioprotegida" Desfibrilador Externo-Automatico
DESA, AED Marca HeartReset AED 100% Holandes
Representamos en exclusiva los Torniquetes 100% Europeos SICH
STRENGTHENED INDIVIDUAL COMBAT HYBRID TOURNIQUET
Dr Ramon REYES, MD,
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..

Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/groups/PDFgratisMedicina #DrRamonReyesMD
https://www.facebook.com/DrRamonReyesMD
https://www.instagram.com/drramonreyesmd/
https://www.pinterest.es/DrRamonReyesMD/
https://twitter.com/eeiispain
Blog
http://emssolutionsint.blogspot.com/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html
TELEGRAM
Group https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q