
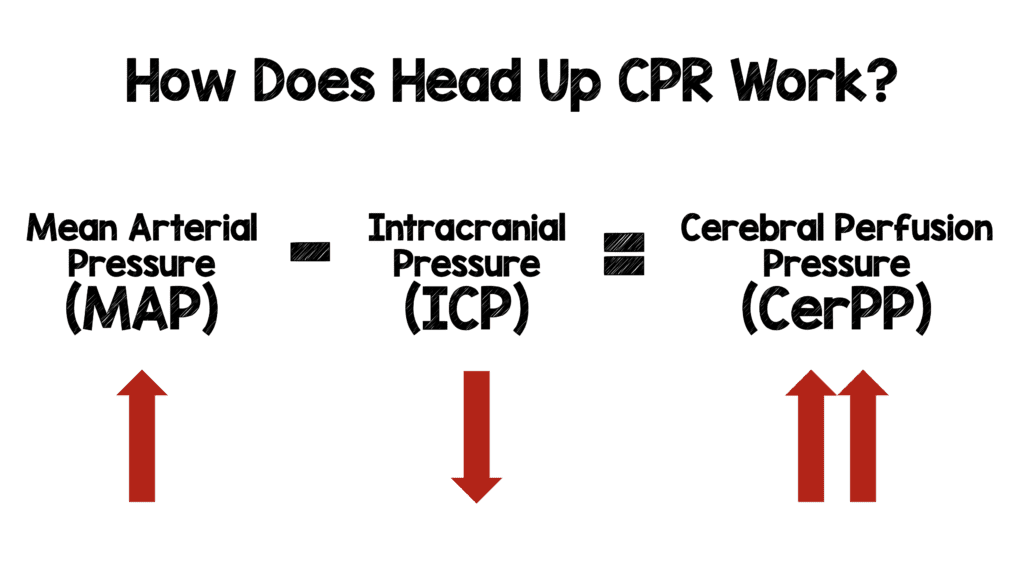
 Background: Head up (HUP) CPR is an emerging concept. The theory behind HUP is it allows for venous blood to drain from the brain to the heart thereby decreasing intracranial pressure and lowering the arterial/venous pressure waves which concuss the brain with each compression. Additionally, conventional CPR increases vascular pressure in both the venous and arterial sides of the heart simultaneously which in turn increases intrathoracic and intracranial pressure which can impede cerebral blood flow and compromise coronary circulation. All of these theories were evaluated and confirmed in animal models with very limited human trials.
Background: Head up (HUP) CPR is an emerging concept. The theory behind HUP is it allows for venous blood to drain from the brain to the heart thereby decreasing intracranial pressure and lowering the arterial/venous pressure waves which concuss the brain with each compression. Additionally, conventional CPR increases vascular pressure in both the venous and arterial sides of the heart simultaneously which in turn increases intrathoracic and intracranial pressure which can impede cerebral blood flow and compromise coronary circulation. All of these theories were evaluated and confirmed in animal models with very limited human trials.
In order for HUP to work however, we have to be able to effectively pump blood up to the brain which is not typically achieved with conventional CPR (C-CPR). Active Compression Decompression with Impedance Threshold Devices (ACD-ITD) are one way to improve C-CPR. They can theoretically help by reducing intracranial pressure (ICP), reduce the potential for concussion with every compression, increase cerebral perfusion pressure (CerPP) and coronary perfusion pressure (CorPP). However, with any new approach, we should always temper enthusiasm, as the realities of implementing them may actually not be helpful, and maybe even harmful.
 Clinical Question: Does head up CPR in OHCA increase cerebral perfusion pressure while maintaining mean arterial pressure?
Clinical Question: Does head up CPR in OHCA increase cerebral perfusion pressure while maintaining mean arterial pressure?
Paper #1: Head Up CPR in Pigs [1]
What They Did:
- This was a randomized, unblinded trial performed in 30 pigs. Pigs had VF induced and after 8 minutes of untreated VF, 2minutes of CPR were performed in the supine position. Pigs were then randomized to:
- Supine CPR (SUP CPR) to HUP CPR (Head and shoulders elevated 30 degrees)
- SUP CPR for the entirety of resuscitation
- Additionally, the authors evaluated Conventional CPR (C-CPR) (Group A) compared to Active Compression-Decompression + Impedance Threshold Devices (ACD + ITD) CPR (Group B) within each randomized group
Results:
-
Group A (C-CPR)
- At 22 minutes the CerPP and CorPP were both improved in the HUP CPR compared to the SUP CPR BUT…None of the pigs achieved ROSC at 22min
-
Group B (ACD + ITD CPR)
- At 22 minutes the CerPP and CorPP were both improved in the HUP CPR compared to the SUP CPR and significantly higher than C-CPR (both in the SUP and HUP groups) AND…Both groups had a similar ROSC rate (6 of 8 in each group)
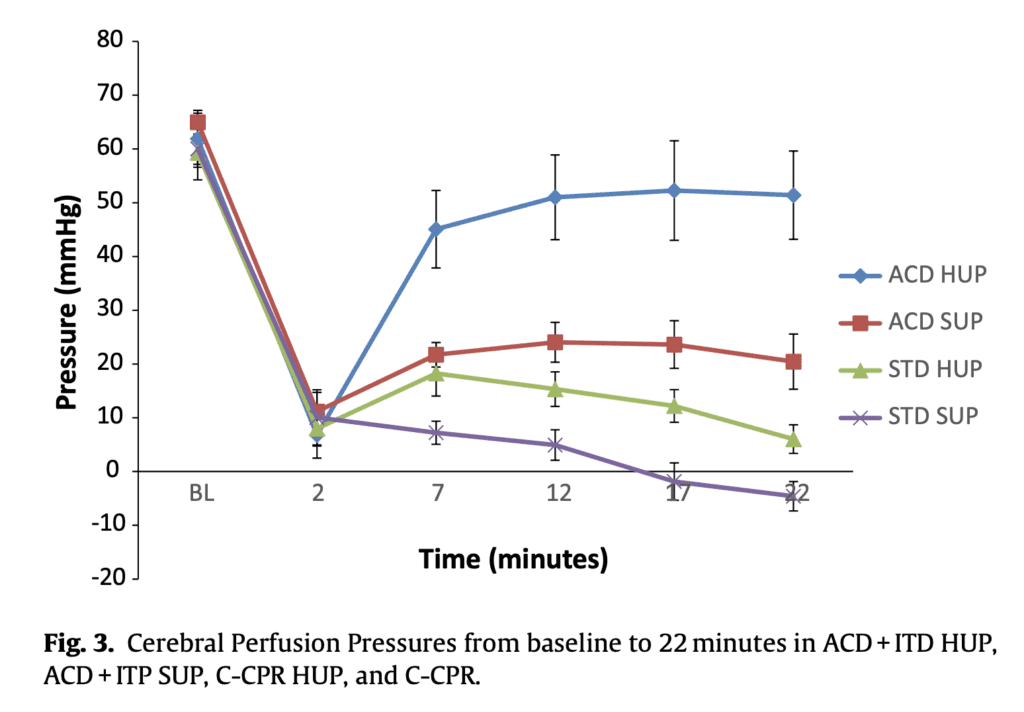
Take Home Point: In this swine model, there appears to be no benefit in performing HUP CPR with C-CPR alone. Using circulation adjuncts such as ACD + ITD CPR with HUP was the most impactful in improving CerPP.
Paper #2: Controlled Sequential Elevation Timing in Pigs [2]
What They Did:
- This was another randomized animal trial with 24 pigs that again had VF induced. Pigs were initially started in the supine position and then gradually elevated with a customized elevation device (CED) at different rates. There were 3 protocols followed:
- Protocol A: CED was activated to elevate the head and thorax over either 4min (3cm/min) or 10min (1.2 cm/min) based upon randomization assignment
- Final head elevation height = 22cm
- Protocol B: Not randomized; Rate of elevation was 2 minutes
- Protocol C: Not randomized; Rate of elevation was 24 seconds
Results:
- 6 pigs in each group (4min, 10min, 2min, and 24sec rise time)
- CerPP and CorPP after 7min were the most improved in the 2 min and 4 minutes of elevation groups followed by the 10 minute and 24 seconds of elevation groups
-
OF NOTE: CerPP and CorPP values in the 4min rise groups were
- 82% and 70% of baseline values after 7 minutes of CPR AND
- 89% and 72% of baseline values after 18 minutes of CPR
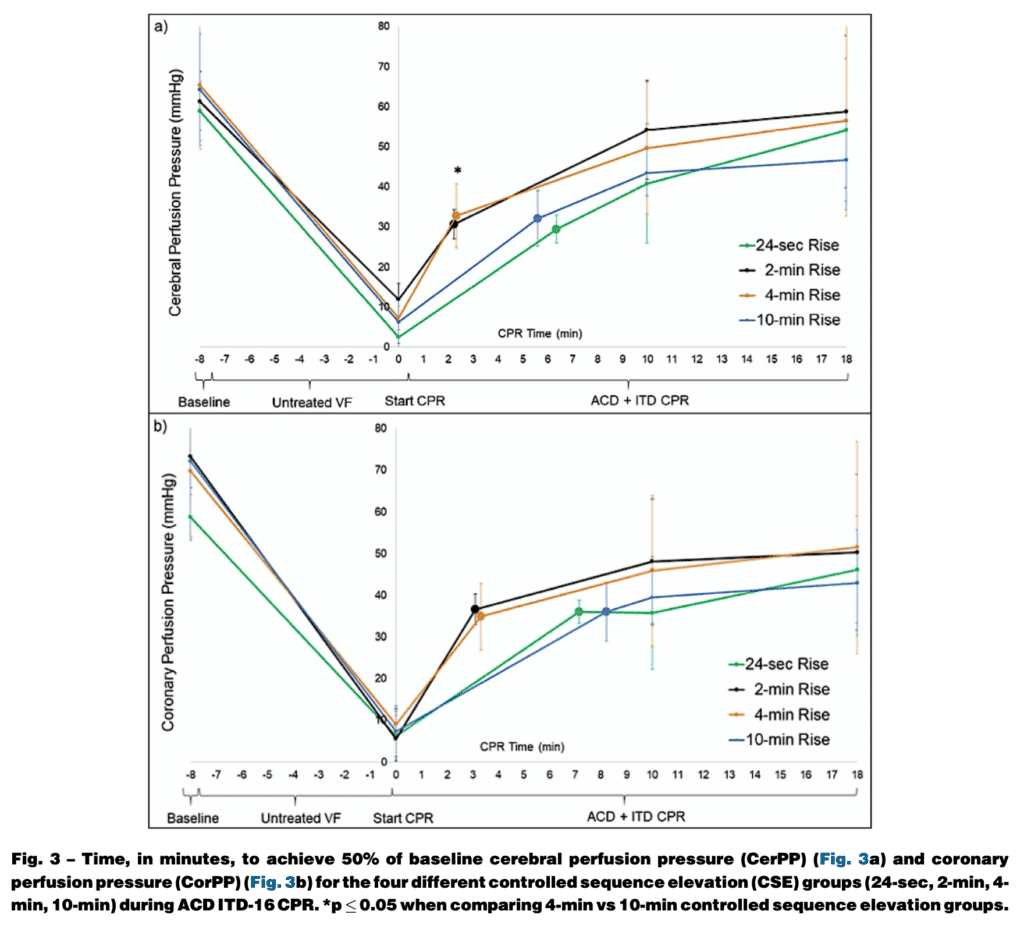
Take Home Point: In this swine model, this study shows it is possible to rapidly generate and sustain near normal CerPP pressures during ACD + ITD CPR by using a customized mechanical head and thorax elevation device, a priming step, and a controlled timing sequence to elevate head and thorax over a 2 – 4 min period.
Paper #3: Clinical Safety and Feasibility of HUP CPR [3]
What They Did:
- Observational, before and after clinical trial in a single prehospital system in the US
- Consecutive OHCA cases followed prospectively over 3.5 calendar years (2014 through 1st half of 2017)
- Year 2014:
- LUCAS mechanical CPR and ITD for out of hospital cardiac arrest were used
- After April 2015:
- O2 was applied but PPV deferred for several minutes
- Solidified a pit crew approach for rapid LUCAS placement (interrupting manual compressions for no more than 5sec)
- Placed patient in a reverse Trendelenburg position (≈20 degrees) after several minutes of CPR
- Year 2014:
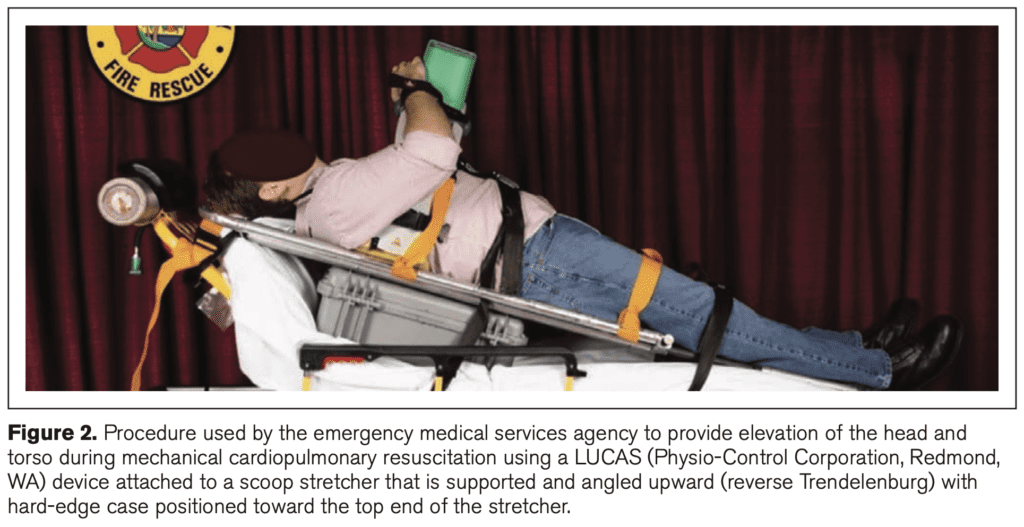
Outcomes: Establish the feasibility of using mechanical CPR devices at a slightly elevated angle and improve resuscitation success (admission to the ED with spontaneous circulation)
Results:
- 2,322 consecutive cases of OHCA encountered
- No problems or physical complications were observed or reported with head-up/torso-up positioning (n = 1,489) in 1st 2 years of implementation
- Initial 1.25 years of study = 806 cases of OHCA (Mean resuscitation rate = 17.87%)
- 2 years after transition period = 1,356 cases of OHCA (Mean resuscitation rate = 34.22%)
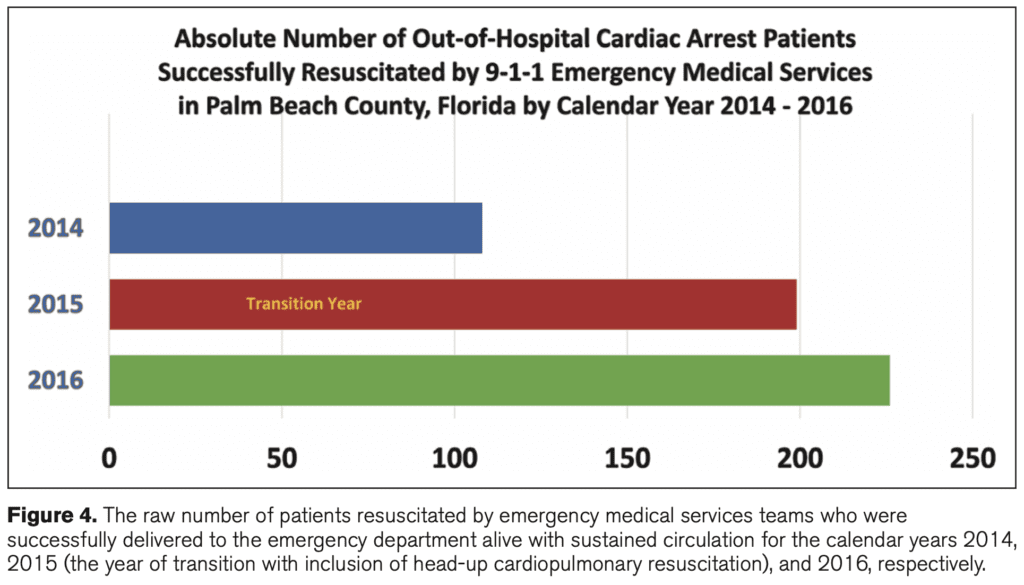
- Resuscitation Success (Admission to the ED with Spontaneous Circulation):
- 2014: 108 patients
- 2015 (Transition Year): 199 patients
- 2016: 226 patients
- Neurologically intact survival rates in 2015 – 2017 remained proportional to EMS resuscitation rates (35 – 40% of those resuscitated ultimately achieved good neurologic status)
Discussion:
- Neurologic status at the time of discharge from the hospital was obtained wherever possible, but not in all patients
- Average EMS crew response intervals: 6:35min/s in 2014, 6:33 in 2015, 6:34 in 2017
- The benefits seen in this study could simply be due to a “Hawthorne effect” and/or progressive experience
- Important Notes About HUP CPR:
- Head-up process should only begin after several minutes of providing traditional supine CPR with the ITD applied to help “prime the pump” which is in line with the previous swine study [2]
- Head up CPR should only be done when using appropriate accompanying adjuncts to enhance circulation (ACD + ITD)
- Human beings have much larger lower extremities which can alter the physiology of head-up/torso-up CPR compared to swine models
- Optimal degree of elevation and actual elevation sequence timing have yet to be determined
- Supine (zero degree) position for the legs accompanied by a head-up and torso-up position may be a more ideal approach than what was used in this trial
Author Conclusion: “The head-up/torso-up cardiopulmonary resuscitation bundle was feasible and associated with an immediate steady rise in resuscitation rates during implementation followed by a sustained doubling of the number of out-of-hospital cardiac arrest patients being resuscitated. These findings make a compelling case that this bundled technique will improve out-of-hospital cardiac arrest outcomes significantly in other clinical evaluations.”
Take Home Point: This trial shows the feasibility/safety of HUP and is the first human trial evaluating HUP CPR resulting in a doubling of successful delivery of resuscitated patients to the ED. These results are promising and yet another step in a potential future advancement in improving outcomes in OHCA
Clinical Take Home Points:
- I find the physiology of HUP CPR fascinating, however, let’s be clear…this is NOT READY FOR PRIMETIME!!!
- Head Up (HUP) CPR is an exciting development in cardiac arrest that has been shown to optimize physiology in animal models:
- Increases CerPP and CorPP
- Decreases ICP
- Increases cerebral blood flow (CBF)
- Maintains MAP
- In early trials HUP with ACD + ITD CPR improves CerPP and CorPP compared to C-CPR and supine CPR
- A priming period prior to HUP appears critical in priming the cardiovascular system
- Before adopting into practice, some important questions still remain unanswered:
- Clinical outcomes of neurologically intact survival were not studied
- Rapid initiation of ACD + ITD CPR plus controlled sequential elevation of the head and thorax may not be immediately available in most systems
- Factors such as witnessed, or bystander CPR cannot be accounted for in these trials
References:
- Ryu HH et al. The Effect of Head Up Cardiopulmonary Resuscitation on Cerebral And Systemic Hemodynamics. Resuscitation 2016. PMID: 26905388
- Rojas-Salvador C et al. Effect of Controlled Sequential Elevation Timing of the Head and Thorax During Cardiopulmonary Resuscitation on Cerebral Perfusion Pressures in a Porcine Model of Cardiac Arrest. Resuscitation 2020. PMID: 31972229
- Pepe PE et al. Confirming the Clinical Safety and Feasibility of a Bundled Methodology to Improve Cardiopulmonary Resuscitation Involving a Head-Up/Torso-Up Chest Compression Technique. Crit Care Med 2019. PMID: 30768501
- Moore JC et al. The “Do’s and Don’ts” of Head Up CPR: Lessons Learned From the Animal Laboratory. Resuscitation 2018. PMID: 30025589
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post In the Pipeline: Head Up CPR in OHCA? appeared first on REBEL EM - Emergency Medicine Blog.