
 Background: In patients presenting to the ED with acute coronary syndrome (ACS), dual antiplatelet therapy is the current standard treatment. This typically consists of aspirin and an adenosine diphosphate receptor antagonist. It is fairly well understood that prasugrel and ticagrelor provide greater, and more rapid platelet inhibition than clopidogrel (i.e. Plavix) [5][6]. Both ticagrelor and prasurgel have a class I recommendation for use in ACS with or without ST-segment elevation. The loading strategies of these two medications are different: ticagrelor is administered as a pre-treatment medication prior to diagnostic angiography while prasugrel is given after coronary anatomy has been assessed by angiography (No advantage has been observed when prasugrel is used as pretreatment) [7]. The authors of this trial (ISAR-REACT 5) looked to compare ticagrelor vs prasugrel in patients with ACS to evaluate efficacy and safety.
Background: In patients presenting to the ED with acute coronary syndrome (ACS), dual antiplatelet therapy is the current standard treatment. This typically consists of aspirin and an adenosine diphosphate receptor antagonist. It is fairly well understood that prasugrel and ticagrelor provide greater, and more rapid platelet inhibition than clopidogrel (i.e. Plavix) [5][6]. Both ticagrelor and prasurgel have a class I recommendation for use in ACS with or without ST-segment elevation. The loading strategies of these two medications are different: ticagrelor is administered as a pre-treatment medication prior to diagnostic angiography while prasugrel is given after coronary anatomy has been assessed by angiography (No advantage has been observed when prasugrel is used as pretreatment) [7]. The authors of this trial (ISAR-REACT 5) looked to compare ticagrelor vs prasugrel in patients with ACS to evaluate efficacy and safety.
Paper: Schupke S et al. Ticagrelor or Prasugrel in Patients With Acute Coronary Syndromes. NEJM 2019. PMID: 31475799
Clinical Question: Does ticagrelor or prasugrel improve the composite of death, myocardial infarction, or stroke at one year after randomization in patients with ACS?
What They Did:
- Intracoronary Stenting and Antithrombotic Regimen: Rapid Early Action for Coronary Treatment (ISAR-REACT) 5 trial
- Phase 4, multicenter, randomized, open-label trial of patients with acute coronary syndromes and for whom invasive evaluation was planned in Germany (21 centers) and Italy (2 centers)
- Patients randomized to:
- Ticagrelor: Loading dose 180mg and continued as a maintenance dose of 90mg PO BID
- Loading dose initiated shortly after randomization
- Prasugrel: Loading dose of 60mg and continued as a maintenance dose of 10mg PO qD (Reduced maintenance dose of 5mg daily was recommended in patients who were 75 years of age or older in patients with body weight of <60kg)
- Loading dose depended on the clinical presentation:
- STEMI: shortly after randomization
- NSTEMI/UA: postponed until the coronary anatomy was known with no pretreatment before diagnostic angiography and before proceeding to PCI
- Loading dose depended on the clinical presentation:
- Ticagrelor: Loading dose 180mg and continued as a maintenance dose of 90mg PO BID
Outcomes:
- Primary: Composite of death, myocardial infarction, or stroke at 1 year
-
Secondary:
- Bleeding at 1 year
- Incidence of the individual components of the primary end point at 1 year
- Incidence of definite or probable stent thrombosis at 1 year
Inclusion:
- Age ≥18 years
- Hospitalized for ACS (STEMI, NSTEMI, or UA)
- Invasive evaluation planned (i.e. coronary angiography)
Exclusion:
- Intolerance or allergy to ticagrelor or prasugrel
- History of any stroke, TIA, or intracranial bleeding
- Known intracranial neoplasm, intracranial AVM, or intracranial aneurysm
- Active bleeding, clinical findings, that in the judgement of the investigator are associated with an increased risk of bleeding
- Fibrin-specific fibrinolytic therapy <24h before randomization or non-fibrin specific fibrinolytic therapy <48h before randomization
- Platelet count <100,000/uL at time of screening
- Known anemia (Hb <10g/dL) at time of screening
- Oral anticoagulation that cannot be safely discontinued for the duration of the study
- INR >1.5 at time of screening
- Chronic renal insufficiency requiring dialysis
- Moderate or severe hepatic dysfunction (Child Pugh B or C)
- Increased risk of bradycardia (sick sinus, AV block grade II or III, bradycardia-induced syncope)
- Index event is an acute complication (<30d) of PCI
- Concomitant medical illness in the opinion of the investigator is associated with a life expectancy <1yr
- Concomitant oral or IV therapy with strong CYP3A inhibitor, CYP3A substrates with narrow therapeutic indices, or strong CYP3A inducers that cannot be safely discontinued
- ≥1 dose of ticagrelor or prasugrel within 5d before randomization
- No written informed consent
- Participation in another investigational drug study
- Previous enrollment in this study
- Pregnancy, giving birth within last 90d, or breast feeding
- Inability to cooperate with protocol requirements
Results:
- 4018 patients randomized
- In patients with STEMI, the interval from symptom onset to randomization was 3.2hrs (range 1.8 to 7.7hrs) in the ticagrelor group and 3.0hrs (range 1.9 to 8.4hrs) in the prasugrel group
- 84.1% of patients underwent PCI
- Glycoprotein IIb/IIa inhibitors were used in 12.3% of patients who underwent PCI
- >99% of patients were receiving ≤100mg of aspirin at the time of discharge
- In patients undergoing PCI for ACS without STEMI the interval from randomization to receipt of the loading dose was 6min (range 1 to 25min) in the ticagrelor group and 61min (range 30 to 142min) in the prasugrel group
-
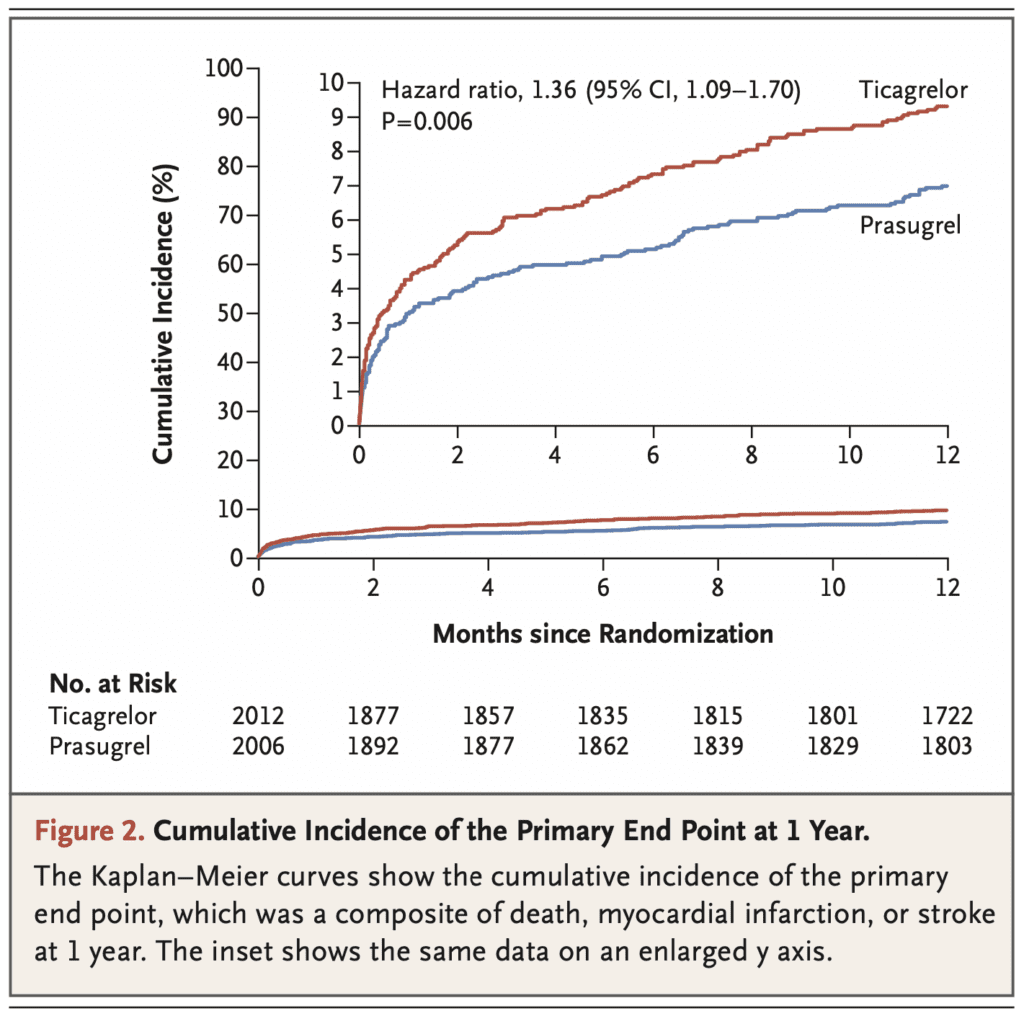
Composite of Death, MI, or Stroke at 1 Year (Primary Outcome):
- Ticagrelor: 9.3%
- Prasugrel: 6.9%
- HR 1.36; 95% CI 1.09 to 1.70; p = 0.006
- Death at 1 Year:
- Ticagrelor: 4.5%
- Prasugrel: 3.7%
- HR 1.23; 95% CI 0.91 to 1.68
- MI at 1 Year:
- Ticagrelor: 4.8%
- Prasugrel: 3.0%
- HR 1.63; 95% CI 1.18 5o 2.25
- Stroke at 1 Year:
- Ticagrelor: 1.1%
- Prasugrel: 1.0%
- HR 1.17; 95% CI 0.63 to 2.15
- Definite or Probable Stent Thrombosis:
- Ticagrelor: 1.3%
- Prasugrel: 1.0%
- Definite Stent Thrombosis:
- Ticagrelor: 1.1%
- Prasugrel: 0.6%
- Major Bleeding:
- Ticagrelor: 5.4%
- Prasugrel: 4.8%
- HR 1.12; 95% CI 0.83 to 1.51; p = 0.46
Strengths:
- Large, multicenter, randomized controlled trial
- Analyses of the primary end point were performed according to the intention-to-treat principle (i.e. inclusion of all patients according to the randomly assigned trial group, irrespective of the actual treatment received) which generalizes to clinical practice
- The safety endpoint of bleeding was analyzed with a modified intention-to-treat principle (included all patients who received at least one dose of the randomly assigned trial drug and were assessed for bleeding events up to 7d after discontinuation of the drug)
- Groups were fairly well balanced at baseline
- 1 year follow up was complete in all but 90 patients in total
- Funding institutions were not involved in the writing of the manuscript or data evaluation
- Outcome assessors were blinded
Limitations:
- Large exclusion criteria, limits the population these results would apply to
- A significant proportion of patients in both groups discontinued the medication after discharge (15.2% in ticagrelor group and 12.5% in the prasugrel group). A per-protocol analysis would be interesting since the percentage discontinuing favored the prasugrel group
- 83% of patient follow up was done by telephone as opposed to face-to-face contact
- The dosage of aspirin in this trial was rather low at ≤100mg per day compared to previous trials using ≥300mg per day. This could have affected ticagrelor outcomes in this trial [4]
- The incidence of the primary outcome in the prasugrel and ticagrelor groups were lower than what was predicted, which means this trial may have been underpowered
- Open-label trial: Patients and clinicians were aware of which drug was being given which could bias results
- Primary outcome was a composite of death, mi, and stroke which are not equivalent outcomes
Discussion:
- The sample size calculation was based on the assumption that the incidence of the primary end point would be 10.0% in the ticagrelor group and 12.9% in the prasugrel group. With this assumption, a total of 1895 patients in each group would be needed for the trial to have 80% power to detect a relative risk that was lower by 22.5% in the rate of the primary endpoint in the ticagrelor group as compared with the prasugrel group
- Although a composite outcome of death, mi, and stroke, when evaluated as individual outcomes, there was a significant reduction of MI (HR 1.63; 95% CI 1.18 to 2.25) but not in the other individual outcomes
- In patients with ACS, without STEMI the pretreatment in the ticagrelor group was 98.7% vs 86.1% in the prasugrel group
- The findings of this trial are interesting as looking at previous evidence:
- In the Platelet Inhibition and Patient Outcomes (PLATO) trial ticagrelor was superior to clopidogrel in patients who underwent PCI and those who were only medically managed.
- In the Targeted Platelet Inhibition to Clarify the Optimal Strategy to Medically Manage Acute Coronary Syndromes (TRILOGY ACS) trial, prasugrel was not superior to clopidogrel in patients who had acute coronary syndromes without STEMI and who did not undergo revascularization.
- Therefore, looking at previous evidence one would think ticagrelor would be superior to prasugrel, which emphasizes the importance of replication of findings
- In the PLATO trial 61.0% of patients underwent PCI during index hospitalization, however 84.0% underwent PCI in this current trial. Therefore, the number of patients not undergoing PCI are small in this trial
- Compliance may have been an issue with less patients likely to stay compliant with ticagrelor as this is a BID medication compared to prasugrel which is a qD medication
Author Conclusion: “Among patients who presented with acute coronary syndromes with or without ST-segment elevation, the incidence of death, myocardial infarction, or stroke was significantly lower among those who received prasugrel than among those who received ticagrelor, and the incidence of major bleeding was not significantly different between the two groups.”
Clinical Take Home Point: In this multicenter, international randomized clinical trial of adult patients with ACS undergoing PCI, prasugrel was superior to ticagrelor in the primary outcome. Additionally, a prasugrel-based strategy with deferred loading after knowledge of the coronary anatomy was superior to a ticagrelor-based strategy with routine pretreatment in patients with NSTEMI and UA. Finally, when evaluating the individual results from the composite primary outcome, the findings of this study were driven by reduction in MI, not in death or stroke.
References:
- Schupke S et al. Ticagrelor or Prasugrel in Patients With Acute Coronary Syndromes. NEJM 2019. PMID: 31475799
- Wallentin L et al. Ticagrelor Versus Clopidogrel in Patients with Acute Coronary Syndromes. NEJM 2009. PMID: 19717846
- Roe MT et al. Prasugrel Versus Clopidogrel for Acute Coronary Syndromes Without Revascularization. NEJM 2012. PMID: 22920930
- Mahaffey KW et al. Ticagrelor Compared with Clopidogrel by Geographic Region in the Platelet Inhibition and Patient Outcomes (PLATO) Trial. Circulation 2011. PMID: 21709065
- Brandt JT et al. A Comparison of Prasugrel and Clopidogrel Loading Doses on Platelet Function: Magnitude of Platelet Inhibition is Related to Active Metabolite Formation. Am Heart J 2007. PMID: 17174640
- Gurbel PA et al. Randomized Double-Blind Assessment of the ONSET and OFFSET of the Antiplatelet Effects of Ticagrelor Versus Clopidogrel in Patients with Stable Coronary Artery Disease: The ONSET/OFFSET Study. Circulation 2009. PMID: 19923168
- Montalescot G et al. Pretreatment with Prasugrel in Non-ST-Segment Elevation Acute Coronary Syndromes. NEJM 2013. PMID: 23991622
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)


The post ISAR-REACT 5 Trial: Ticagrelor vs Prasugrel in ACS appeared first on REBEL EM - Emergency Medicine Blog.