
 Case: A 51-year-old woman, with no pertinent past medical history, presented to the Emergency Department (ED) complaining of right hand pain after a large fragment from a wooden cooking spoon penetrated her right palm approximately 1 week ago. She reported immediately removing the splinter and starting old, previously prescribed amoxicillin prior to her visit. She was prompted to visit the ED after her pain gradually increased, affecting her ability to flex and extend her right fourth digit.
Case: A 51-year-old woman, with no pertinent past medical history, presented to the Emergency Department (ED) complaining of right hand pain after a large fragment from a wooden cooking spoon penetrated her right palm approximately 1 week ago. She reported immediately removing the splinter and starting old, previously prescribed amoxicillin prior to her visit. She was prompted to visit the ED after her pain gradually increased, affecting her ability to flex and extend her right fourth digit.
On physical exam, the patient was afebrile with all other vital signs within normal limits. There was significant tenderness localized to the base of the right fourth digit near the proximal interphalangeal (PIP) joint, associated with edema, ecchymosis, and erythema. While the patient’s right hand remained neurovascularly intact, significant restrictions in passive motion, including flexion and extension, was noted to the right fourth digit. On visual inspection, no foreign bodies were appreciated.
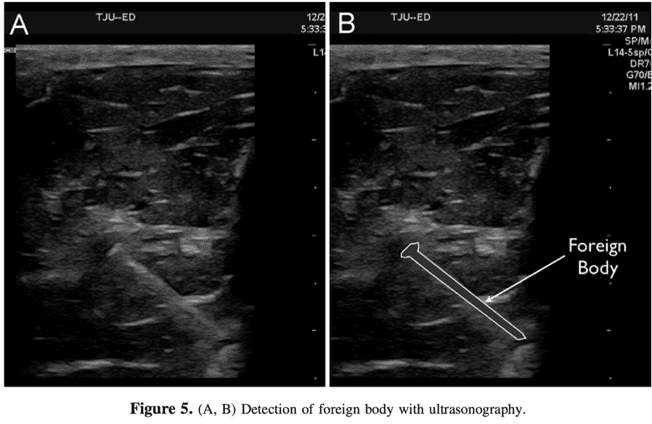
A radiograph of the right hand was ordered, which was negative for any acute abnormalities, including foreign body. However, due to the patient’s clinical presentation and the potential radiolucency of the suspected foreign body, a point-of-care ultrasound was performed.
Background
- Soft tissue injuries are a common presentation. While retained foreign bodies are not that common, missed ones are a common cause of malpractice claims (Halaas 2007)
- Diagnostic dilemma for practitioners
-
Traditional approaches (plain radiography, computed tomography) do not always identify foreign bodies (Ginsburg 1990)
- Traditional techniques come at the expense of radiation and increased throughput times
- Radiolucent objects such as wood or plastic are often not visualized
-
Ultrasonography presents several advantages over traditional imaging techniques for the identification and localization of foreign bodies
- Highly reliable modality for detecting non-radiopaque foreign bodies
- Fast and provides immediate results
Epidemiology (Halaas 2007)
- Annually, there were >8 million emergency department visits for open wounds
- Retained glass present in 15% of wounds
- Prevalence increases in warmer climates and seasons
Presentation
- History of soft tissue injury
- Site of penetration or soft tissue injury on physical examination
- Localized swelling
Complications
- Infection
- Cellulitis
- Osteomyelitis
- Peripheral nerve damage
- Arterial aneurysms
- Synovitis
Diagnosis
- Description of the probable object can help localize the problem and determine the need for removal
-
Plain radiography
- 2 views of area of interest – transverse/longitudinal
- Provides optimal evaluation and characterization of object
- Sensitivity and specificity 29% and 100% respectively (Pattamapaspong 2013)
-
Computed Tomography
- Generally not indicated given the other available imaging modalities
- Avoid excessive and unnecessary radiation in children
- Sensitivity and specificity 63% and 98% respectively (Pattamapaspong 2013)
-
 POCUS
POCUS
- Sensitivity for the localization of foreign bodies can reach between 96.7% – 100% with skilled operators (Lyon 2004)
- Identification of the foreign body can be difficult given echo patterns vary with size, nature, and retention time (Chen 2016)
-
Technique (ACEP UGEP 2008)
- High frequency linear transducer (7.5-10 MHZ) is placed on the area of interest
- Area of interest is then scanned in both sagittal and transverse planes in search of the hyperechoic object
- Tegaderm may be placed over a laceration to avoid further contamination of the wound site
- Standoff pad may be used to elevate the transducer: fill a glove with ultrasound gel to help identify very superficial foreign bodies
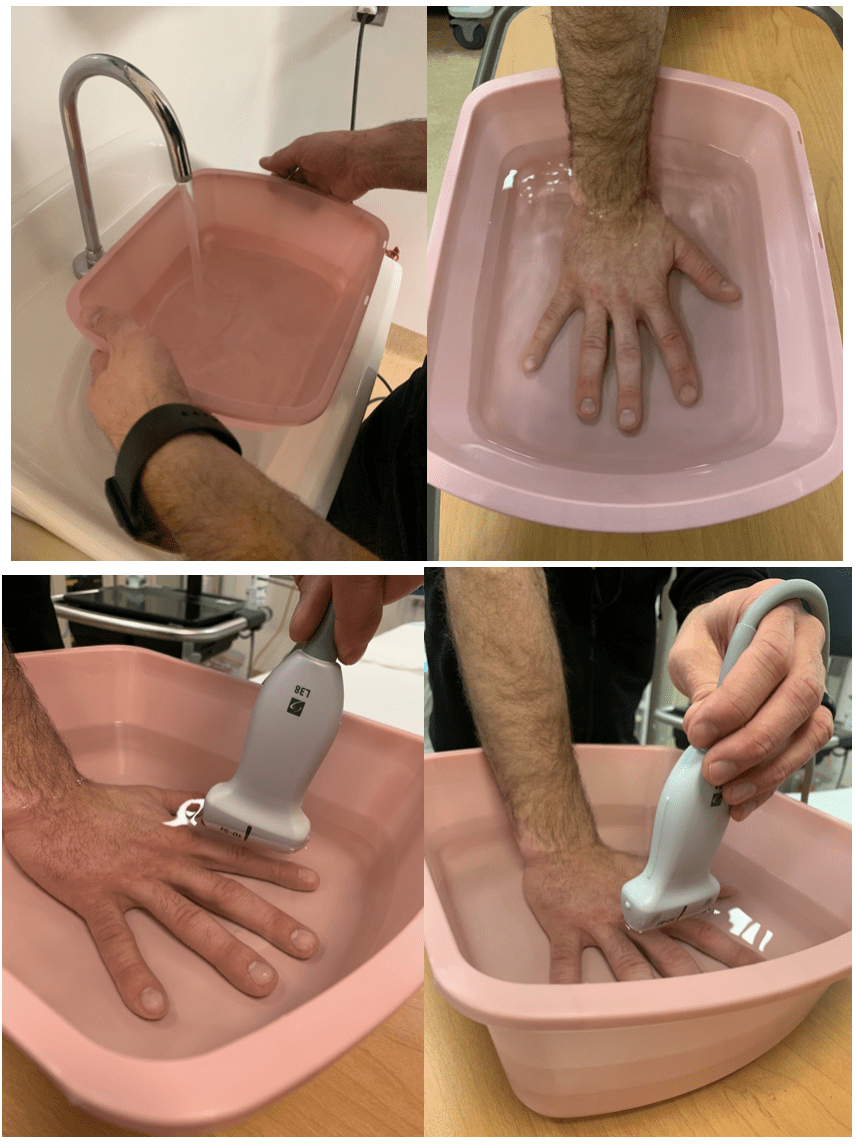
- Alternative technique is placing the extremity in a water bath with the probe placed just below the surface of the water, but does not need to contact the skin as the water acts as an ultrasound medium to enhance visualization
Case Findings

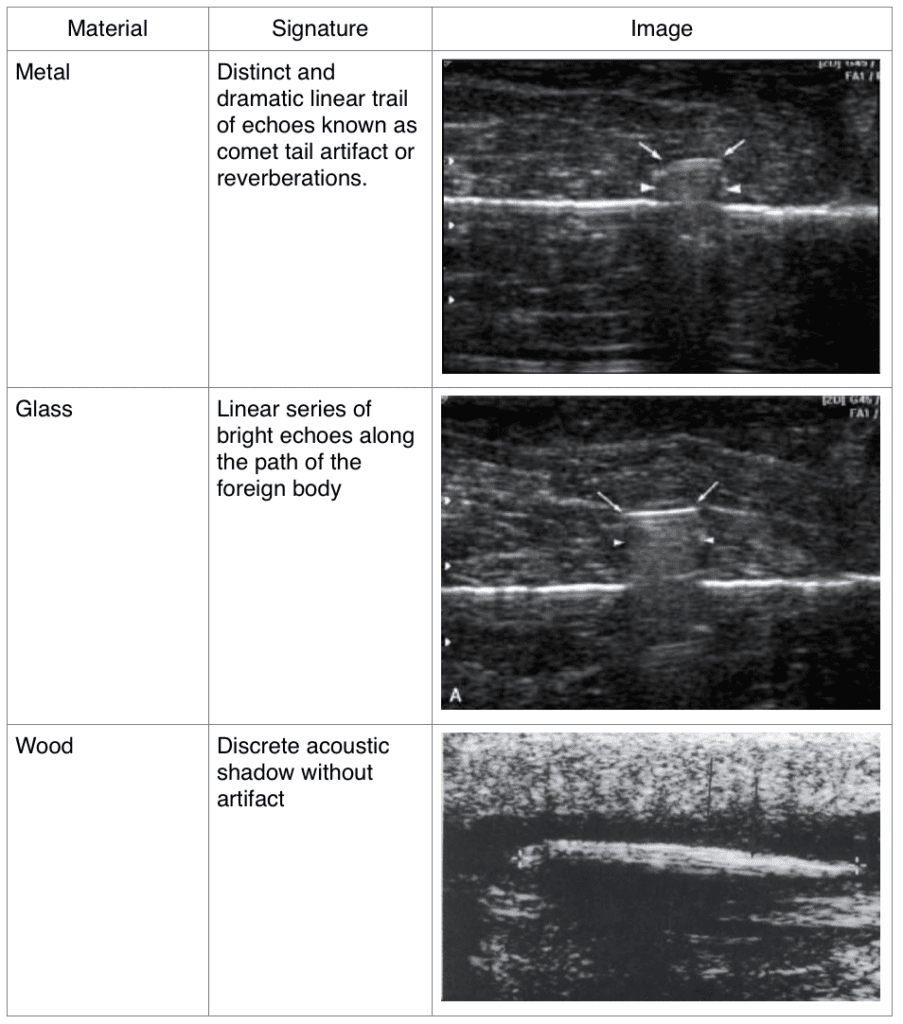
Common Sonographic Signatures (Lyon 2004)
 Management
Management
- Prior to attempting ED removal, indications for consulting a specialist include:
-
- Significantly deep structures
- Failed retrieval requiring further dissection
- Neurovascular compromise
- Objects located near vascular structures
- Concerns for compartment syndrome
-
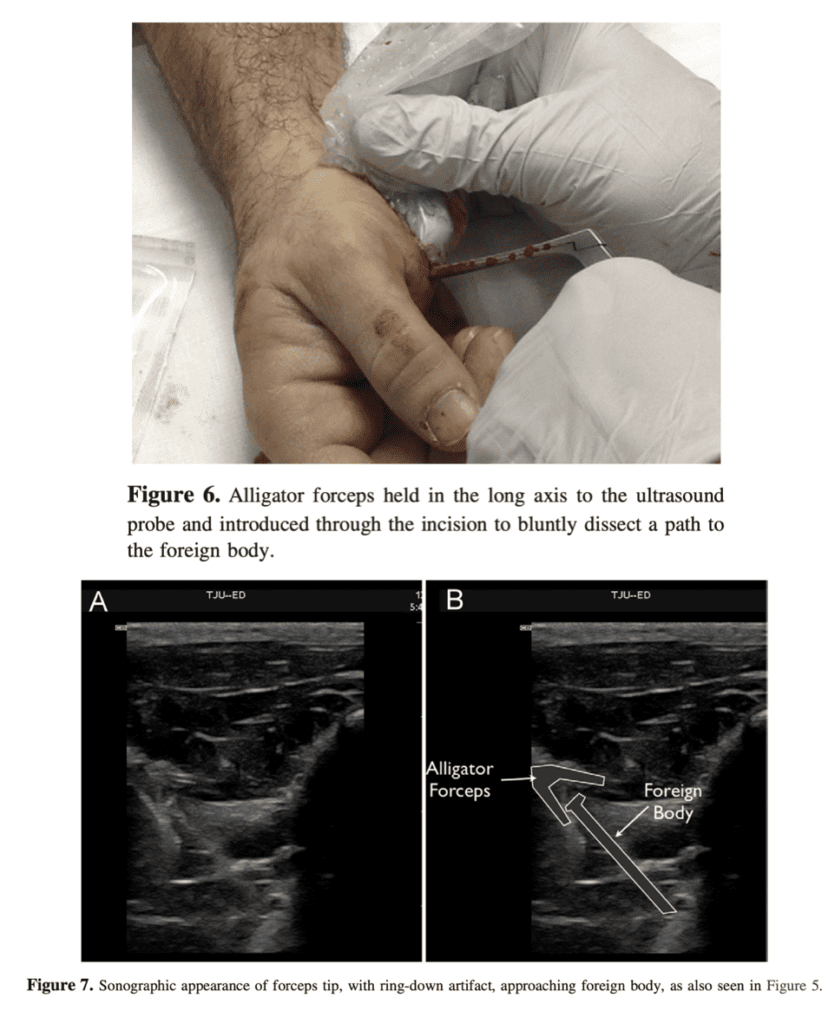
Overview of ED approach (Paziana 2012):
- Real-time ultrasound guided retrieval
- Identify object and critical surrounding structures
- Hold u/s probe in long axis
- Introduce retrieval device and use u/s guidance to obtain foreign body
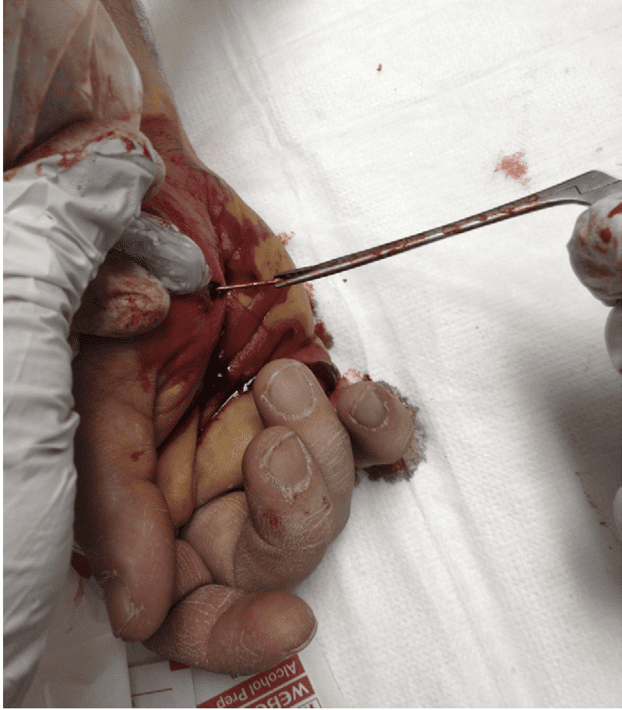
- Slowly remove foreign body in the same direction it was introduced – AVOID damaging nearby critical structures
- Confirm retrieval of ENTIRE foreign body
Case Conclusion
Ultrasound findings were shared with orthopedic surgery, who recommended antibiotic therapy and outpatient foreign body removal. Subsequently, the patient was prescribed cephalexin, given strict return precautions, and instructed to follow up at the orthopedic clinic.
Take Home Points
- Foreign bodies present a diagnostic dilemma for practitioners
- Wood and plastic are often not identified on traditional imaging
-
Ultrasonography presents several advantages over traditional imaging techniques for the identification and localization of foreign bodies
- Rapid diagnostic modality
- Assist with removal in real time
Guest Post By:
Ellsworth Wright, MD MBS
Brandon Somwaru, DO
PGY-2
St. Joseph’s Regional Medical Center
Paterson, NJ
Video References
- U/S guided removal techniques
References
- Chen K et al. An Overview of point-of-care ultrasound for soft tissue and musculoskeletal applications in the emergency department. J Intensive Care 2016. PMID: 27529031
- Ginsburg M et al. Detection of Soft-Tissue Foreign Bodies by Plain Raidography, Xerography, Computed Tonography, and Ultrasonography. Ann Emerg Med. 1990. PMID: 2188542
- Halaas GW. Management of foreign bodies in the skin. Am Fam Physician. 2007. PMID: 17894138
- Lyon M et al. Detection of Soft Tissue Foreign Bodies in the Presence of Soft Tissue Gas. J Ultrasound Med 2004. PMID: 15154535
- Pattamapaspong N. et al. Accuracy of radiography, computed tomography and magnetic resonance imaging in diagnosing foreign bodies in the foot. Radiol Med. 2013. PMID: 22744349
- Paziana K et al. Soft tissue foreign body removal technique using portable ultrasonography. Wilderness Environ Med. 2012. PMID: 22835803
- Geria R. Ultrasound Guided Procedures: Foreign Body Localization. Sonoguide 2008. [Link is HERE]
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post POCUS and Soft Tissue Foreign Bodies appeared first on REBEL EM - Emergency Medicine Blog.