
 Background: Not all occlusion myocardial infarctions (OMIs) present with classic ST-segment elevation (We have covered this on REBEL EM Before HERE, HERE, and HERE). OMIs of the “posterior” and “lateral” walls are the most commonly missed, with >50% of left circumflex occlusions (Posterior and lateral walls suppled by the circumflex artery)not receiving emergent reperfusion. These misses occur because isolated posterior OMIs do not result in classic ST-elevation ECG changes. Instead, posterior OMI results in ST depression which is maximal in V1 to V4 (alternatively, ST-depression of subendocardial ischemia is maximal in V5 to V6). While the above findings are well-established, it’s unclear how accurately they predict OMI and the need for cardiac catheterization.
Background: Not all occlusion myocardial infarctions (OMIs) present with classic ST-segment elevation (We have covered this on REBEL EM Before HERE, HERE, and HERE). OMIs of the “posterior” and “lateral” walls are the most commonly missed, with >50% of left circumflex occlusions (Posterior and lateral walls suppled by the circumflex artery)not receiving emergent reperfusion. These misses occur because isolated posterior OMIs do not result in classic ST-elevation ECG changes. Instead, posterior OMI results in ST depression which is maximal in V1 to V4 (alternatively, ST-depression of subendocardial ischemia is maximal in V5 to V6). While the above findings are well-established, it’s unclear how accurately they predict OMI and the need for cardiac catheterization.
Paper: Meyers HP et al. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia. J Am Heart Assoc 2021. PMID: 34775811
Clinical Question: In a group of patients at high-risk for acute coronary syndrome in the ED, is precordial ischemic ST-segment depression maximal in V1 to V4 specific for occlusion myocardial infarction?
What They Did:
- Planned retrospective substudy of the Diagnosis of Occlusion MI and Reperfusion by Interpretation of the Electrocardiogram in Acute Thrombotic Occlusion database
- The database is a 2-site collaboration designed to study ECG findings in OMI
- Any ST-depression maximal in V1 to V4 refers to any ST-depression of any magnitude (Even <0.5mm) that is maximal in V1 to V4 in any context (i.e. RBBB)
Outcomes:
-
Primary: Presence of OMI (Specificity of suspected ischemic STDmaxV1-4 for OMI)
- Confirmed OMI on cardiac catheterization defined as an acute culprit lesion with TIMI 0 to 2 flow
- Presumed OMI with significant cardiac outcome defined as any of the following:
- Acute but nonocclusive (TIMI >2) culprit lesion with highly elevated cardiac troponin T ≥1.0ng/mL or Troponin I ≥10ng/mL
- If no angiography, then highly elevated cardiac troponin and a new or presumed new regional wall motion abnormality on echocardiography
- ECG positive for STEMI with death before attempted emergent catheterization
- TIMI 0 to 1 culprit lesions
Inclusion:
- All urgent and emergent left heart catheterizations during 1 year from 2 institutions
- At Stony Brook cases were added from a prospective cohort of ED patients who were admitted to the cardiology service with suspected ACS during a 6-month time period
- Additional controls were added from Hennepin Healthcare by searching the Use of TROPonin in Acute coronary syndromes (UTROPIA) database with patients without OMI but with STE, STD, or T-wave inversion
Exclusion:
- No ECGs in the electronic medical record
- Insufficient retrospective information available to determine the primary outcome
Results:
- 808 patients with 3421 ECGs
- Final Diagnosis of Acute MI: 265
- 265 met criteria for OMI
- Only 108 (41%) met STEMI criteria at any time
- Median time from presentation to cardiac catheterization = 75min
- Final Diagnosis of Acute MI: 265
- Total of 99 OMIs Detected by Suspected Ischemic STDmaxV1-4
- 47 (47%) had accompanying STEMI criteria in other locations
- Culprit lesions included:
- RCA: 53
- LCx: 32
- PDA: 7
- Smaller Branches (OM1, OM2, Ramus intermedius, and left posterolateral: 30
- Other vessels: 10
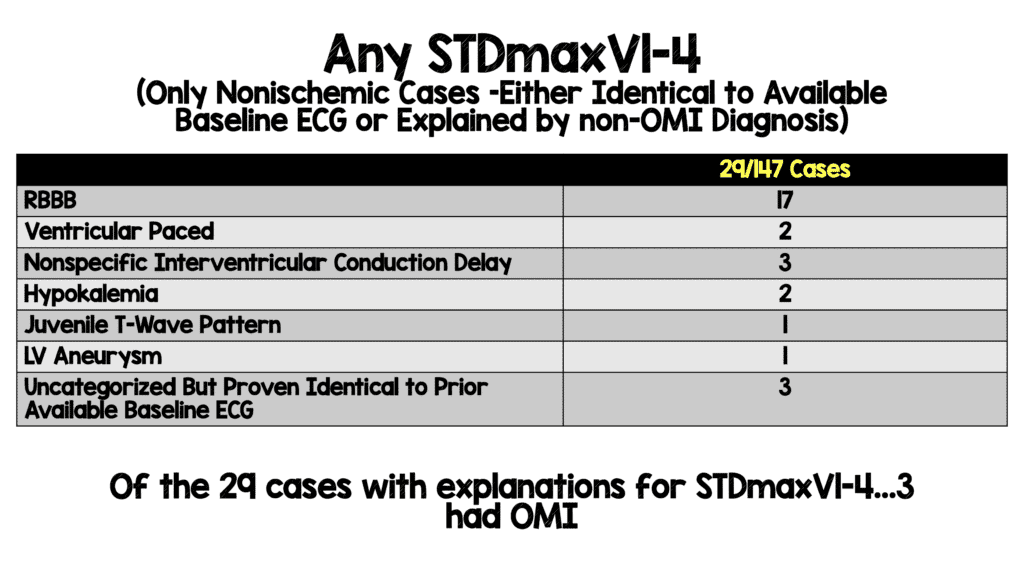
- False Positives (Patients With Suspected Ischemic STDmaxV1-4 But Without OMI):
- 13 patients had STDmaxV1-4 but did not meet the definition of OMI
- All 13 underwent angiogram
- 7 had culprit lesions
- Proximal LAD: 2
- Mid Cx: 1
- Middle RCA: 1
- 2nd OM: 2
- 3rd Diagonal: 1
- 6 required PCI
- 1 died during index visit
- Patients with STEMI(+) OMI and STDmaxV1-4 vs STEMI(-) OMI with STDmaxV1-4:
- 99 patients with OMI with suspected ischemic STDmaxV1-4
- 47 had concomitant STEMI criteria (STEMI(+) OMI)
- 52 remaining (20% of all 265 OMIs) did not (STEMI(-) OMI)
- These patients were completely missed by STEMI criteria but correctly identified by suspected ischemic STDmaxV1-4
- Suspected Ischemic STD Borderline/Equal Between V4 and V5
- 7 patients
- All 7 underwent angiography
- 5 had culprit lesions (All LCx)
- 4 had OMI
- 3 received PCI
Strengths:
- ECGs were interpreted by two ED physicians blinded to all patient information except age and sex
- Interpreters could not go back and change an interpretation once entered, as happens in real time in the ED
- All 108 consecutive OMI cases from the prospective cohort were reviewed for STEMI criteria by a cardiologist blinded to outcome and study goals
Limitations:
- Insufficient resources to perform a prospective, consecutive cohort study and findings may not apply to undifferentiated ED patients without ACS strongly suspected
- Retrospective study performed at only 2 centers
- Only 8 patients had posterior leads performed and recorded
- 2 expert ECG interpreters reviewed all the ECGs. ECG interpretation is subjective and not all ED physicians may have this level of experience and therefore limits external validity of these findings
- Different criteria to establish final diagnosis of AMI at the different hospitals
- Patient selection process was convoluted which could lead to some bias in patient selection
Discussion:
- I have placed all the specific results above for completeness of my review, but quite frankly it is a lot of math to get through. So here is the gist of what the results above show:
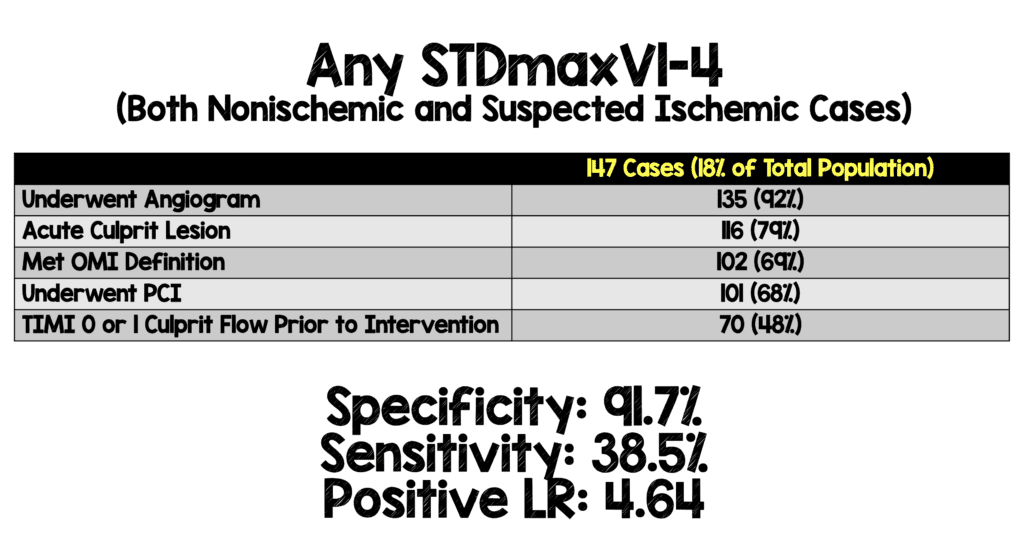
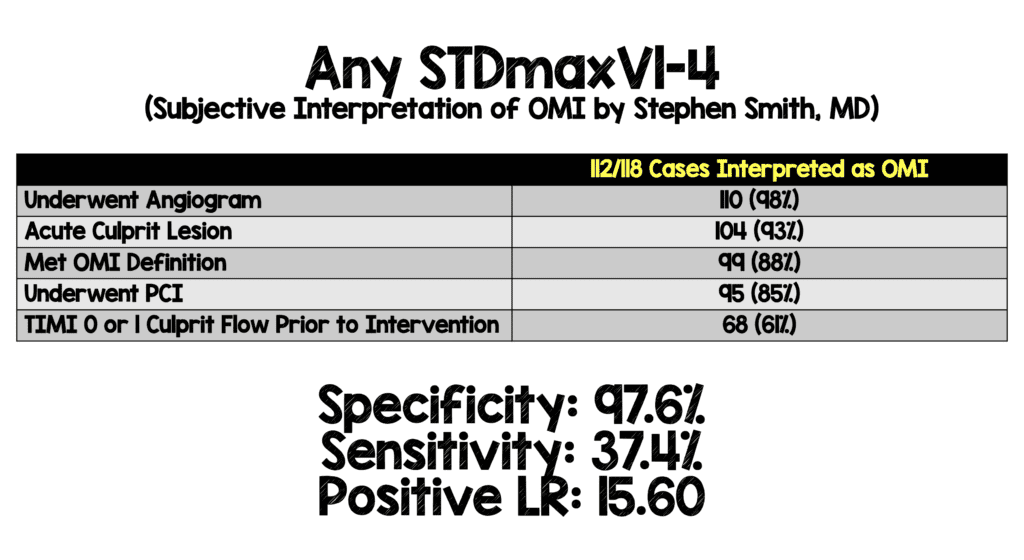
- Any STDmaxV1-4 is 92% specific for OMI among ED patients with ACS
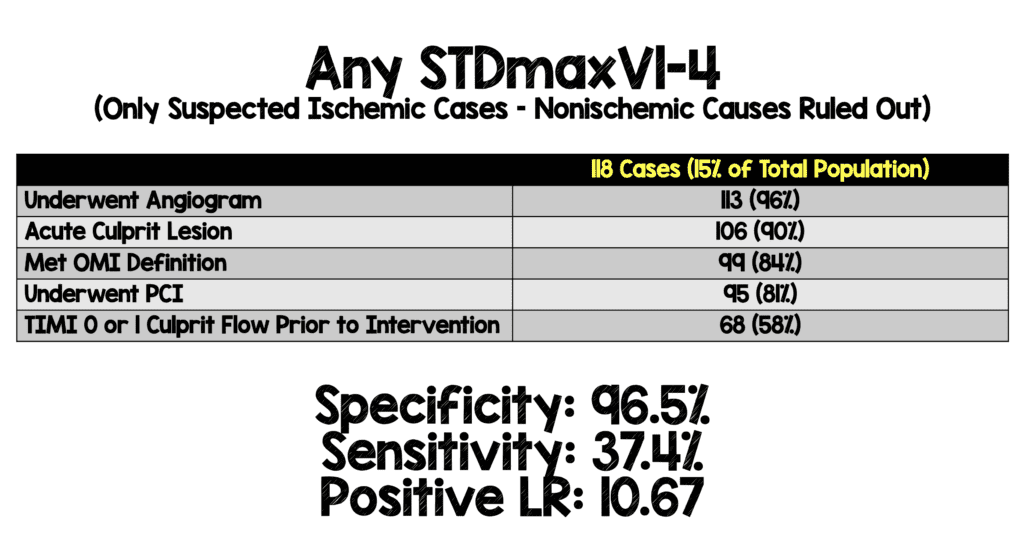
- This number is increased to 97% for suspected ischemic STDmaxV1-4 (STDmaxV1–4 that could not be explained by a nonischemic cause was classified as primary STD, not secondary to an identifiable nonischemic source, and referred to as “suspected ischemic STDmaxV1–4.”)
- The positive likelihood ratio in any patient with STDmaxV1-4 was ≈5. This is only a fair value, and most likely due to the very low sensitivity. The absence of this finding doesn’t rule out OMI
- Among the 99 patients with OMI and STDmaxV1-4, the 52 (53%) lacking STEMI criteria had similarly high peak troponin levels but significantly lower chance of getting emergent heart catheterization within 90minutes of presentation
- STDmaxV1-4 is a single ECG finding designed only to detect the posterior component of an OMI
- STDmaxV1-4 not secondary to an abnormal QRS (i.e. RBBB) is an accurate marker of posterior OMI)
- STDmaxV5-6 is a manifestation of subendocardial ischemia:
- Supply demand mismatch
- ACS involving LM, LAD, or triple vessel disease
- Only 28% of patients with suspected ischemic STDmaxV5-6 had OMI
- Most STDmaxV1-4 will have concomitant subtle OMI findings in the inferior and/or lateral leads
- Even <1.0mm of STDmaxV1-4 is specific for OMI BUT there were no patients who had this and no other findings of OMI in other areas of the ECG
Author Conclusion: “Among patients with high-risk acute coronary syndrome, the specificity of ischemic STDmaxV1-4 was 97% for OMI and 96^ for OMI requiring percutaneous coronary intervention. STEMI criteria missed half of OMIs detected by STDmaxV1-4. Ischemic STDmaxV1-V4 in acute coronary syndrome should be considered OMI until proven otherwise.”
Clinical Take Home Point: In patients with symptoms suggestive of ACS in the ED, the specificity of STDmaxV1-4 was 97% for the diagnosis of posterior OMI and 96% for posterior OMI requiring PCI. This finding of STDmaxV1-4 is both highly accurate and sufficient without the need for routine posterior leads. Until further data become available, in any patient with suspected ACS and ischemic STD maximal in V1 – V4, these findings should be attributed to OMI until proven otherwise.
References:
- Meyers HP et al. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia. J Am Heart Assoc 2021. PMID: 34775811
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post Posterior Occlusion Myocardial Infarctions and STDmaxV1-4 appeared first on REBEL EM - Emergency Medicine Blog.