
 Background: In the past few years there has been a growing debate between the use of balanced multielectrolyte solutions (BMES) and saline in the critically ill (See the “for more about this topic” section below). Recent research has yielded inconsistent results with RCTs showing improved mortality (SMART), no change in mortality (BaSICS), and decreased acute kidney injury (SMART Trial Part 2). The varied results of high quality trials makes further research important.
Background: In the past few years there has been a growing debate between the use of balanced multielectrolyte solutions (BMES) and saline in the critically ill (See the “for more about this topic” section below). Recent research has yielded inconsistent results with RCTs showing improved mortality (SMART), no change in mortality (BaSICS), and decreased acute kidney injury (SMART Trial Part 2). The varied results of high quality trials makes further research important.
REBEL Cast Ep108: The PLUS Trial – Balanced vs Unbalanced Fluids in the Critically Ill
Paper: Finfer, S et al. Balanced Multielectrolyte Solution Versus Saline in Critically Ill Adults. NEJM 2022. PMID: 35041780 [Access on Read by QxMD]
Clinical Question: Do balanced multicelctrolyte solutions (BMES) reduce death in critically ill patients in the ICU vs 0.9% saline solution?
What They Did:
- Double-blind, parallel group, randomized, controlled trial
- 53 ICUs in Australia and New Zealand
- Patients randomized to:
- BMES: Plasma-Lyte 148
- 9% Saline Solution
Outcomes:
- Primary: Death from any cause within 90 days after randomization
-
Secondary:
- Receipt of new renal replacement therapy
- Maximum increase in creatinine level during ICU stay
Inclusion:
- Patients ≥18 years of age
- Admitted to one of 53 participating ICUs
- Fluid resuscitation was judged by the treating clinician to be necessary (BMES or saline) and equally appropriate
- Expected to be in the ICU for 3 consecutive days
Exclusion:
- Patients requiring specific fluid requirements
- Received disqualifying fluid resuscitation (initially considered to be any volume and later amended to be >500mL of fluid prescribed and administered in the ICU)
- Imminent risk for death
- Preexisting life expectancy of <90d
- Traumatic brain injury or were at risk for cerebral edema
Results:
- 5037 patients recruited
- BMES: 2515 pts
- Saline: 2522 pts
- Primary outcome data available for 4,846 patients (96.2% of recruited patients)
- 45.2% admitted to ICU directly from operating or recovery room (≈27% were emergency surgery as opposed to elective surgery)
- ≈33% admitted to ICU directly from the ED
- 79.00% on mechanical ventilation at the time of randomization
- 42.3% had sepsis
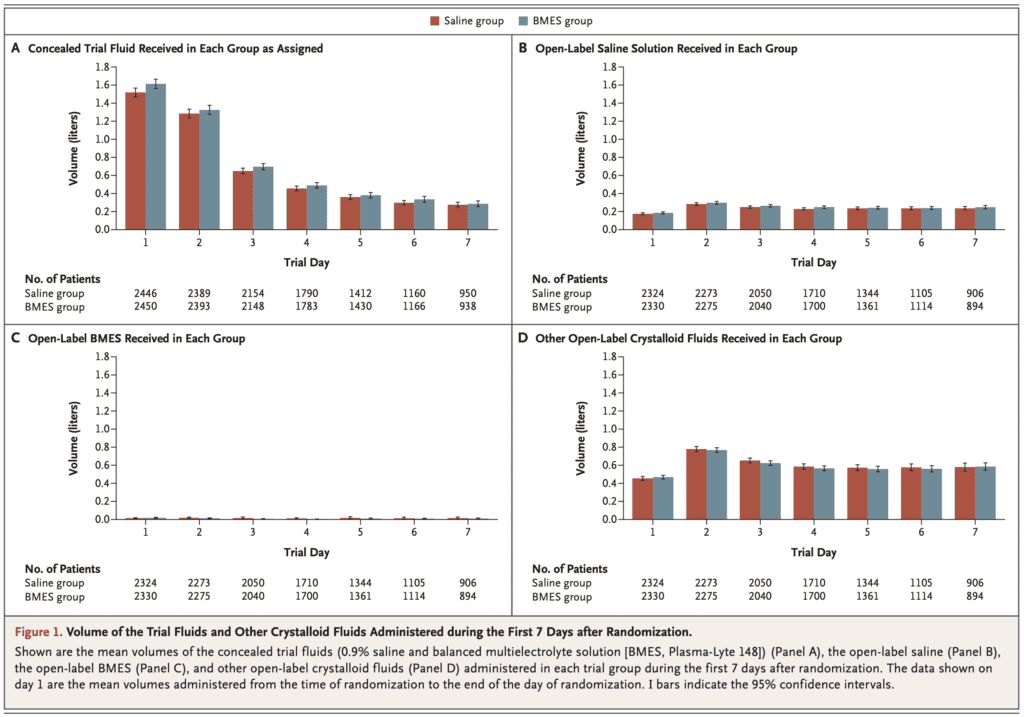
- Volumes of IV fluids, blood products, total fluid input/output, and urine output did not differ significantly between groups
- During the first 7 days after randomization, daily mean heart rate, mean arterial pressure, and mean central venous pressure also did not differ significantly between groups
- Median volume of trial fluid received
- 3.9L (2.0 to 6.7) in the BMES group
- 3.77L (Range 2.0 to 6.3) in the saline group
- Death Within 90d (primary outcome)
- BMES: 530/2433 (21.8%)
- 0.9% Saline: 530/2413 (22.0%)
- Difference -0.15%; 95% CI -3.60 to 3.30; p = 0.90
- OR 0.99; 95% CI 0.86 to 1.14
- NOT STATISTICALLY SIGNIFICANT
- Initiation of New Renal Replacement Therapy
- BMES: 306/2403 (12.7%)
- 0.9% Saline: 310/2394 (12.9%)
- Difference: -0.2%; 95% CI -2.96 to 2.56
- Mean Maximum Increase in Serum Creatinine Level
- BMES: 36.6 +/- 94.0 umol/L
- 0.9% Saline: 36.1 +/- 90.2 umol/L
- Difference 0.5 umol/L; 95% CI -4.7 to 5.3
- Number of adverse and serious adverse events did not differ between groups
Strengths:
- Large, multicenter, double-blind, randomized clinical trial
- Used a patient centered primary outcome with adjusted analyses and multiple evaluations of various subgroups
- Patients received BMES or saline for a longer duration and greater volume (>2L) than in previous trials
- Excellent follow up or the primary and secondary outcomes
- Fluids were supplied in identical 1000 mL bags
- Trial group assignments were concealed from patient, patients’ legally authorized representatives, researchers, and treating clinicians
- The primary outcome was examined in six prespecified subgroups allowing results of the primary outcome to be more robust
- Baseline characteristics were similar between groups (i.e. groups were well balanced at baseline)
Limitations:
- The type and rate of fluids were not controlled for before ICU admission, nor once the patient was outside the ICU
- Arterial pH was significantly higher and serum chloride level significantly lower among patients in the BMES group compared to the saline group. Although this is expected and a lab-oriented outcome, neither is a patient-oriented outcome
- Median time from ICU admission to randomization was 2 days. Lots of interventions, fluids, etc can happen in that timeframe which could have an effect on outcomes
- Reduced size of recruitment and unavailable data on the primary outcome for some patients
- >50% of patients in the BMES group received 500mL or more of saline in the ICU predominantly for delivery of medications that have not been tested for compatibility with BMES. This could have attenuated a protective effect of BMES
- Did not examine the effects of BMES as compared with saline in patients with traumatic brain injury
- Only used Plasma-Lyte 148 as BMES which is not the same as other balanced solutions (i.e. LR)
- Contamination (i.e. randomzed to BMES but got saline) was greater in the BMES group than the saline group (63% vs 3.5%)
Discussion:
- Power calculation
- The authors estimated that 8800 patients would provide the trial with a 90% power to detect an absolute difference of 2.9% in 90d all-cause mortality with a baseline mortality of 23%
- Due to COVID-19, recruitment was disrupted, and it was decided to stop recruitment early
- Therefore, another power calculation estimated that 5000 patients would provide the trial with 90% to detect an absolute difference of 3.8% with the same assumption about baseline mortality
- Fluids
- 24hrs prior to randomization patients received similar amounts and types of IV fluids
- 5% in the BMES group had received 500mL or more of saline
- 2% in the saline group had received 500mL or more of BMES
- During treatment
- Median duration of treatment with assigned trial fluid was 6.0d (Range: 3 to 10) in both groups
- Median volume of trial fluid received
- 9L (2.0 to 6.7) in the BMES group
- 7L (Range 2.0 to 6.3) in the saline group
- After randomization
- 0% in BMES group received 500mL or more of open-label saline
- 5% in the saline group received 500mL or more of BMES
- 24hrs prior to randomization patients received similar amounts and types of IV fluids
- Many patients in this trial were post-surgical which doesn’t apply to an ED population.
Author Conclusion: “We found no evidence that the risk of death or acute kidney injury among critically ill adults in the ICU was lower the use of BMES than with saline.”
Clinical Take Home Point: In critically ill adults in the ICU requiring intravenous fluids, it appears the type of fluid does not make a difference on the outcomes of mortality or AKI. However, there may be individual patient characteristics or other factors (i.e. cost, availability, drug compatibility, etc) that may determine which fluids should be used. This is probably one of the best trials trying to answer the debate on balanced vs unbalanced crystalloids. Unlike other studies where patients received <2L of fluids on average in this trial patients received >3L.
References:
- Finfer, S et al. Balanced Multielectrolyte Solution Versus Saline in Critically Ill Adults. NEJM 2022. PMID: 35041780 [Access on Read by QxMD]
For More Thoughts on This Topic Checkout:
- REBEL EM: SMART Trial Part 2 – Secondary Analysis of Balanced Crystalloids vs Saline in Sepsis
- REBEL EM: The BaSICS RCT – Balanced Solution vs 0.9% Saline Solution in Critically Ill Pts
- REBEL EM: Is the Great Debate Between Balanced vs Unbalanced Crystalloids Finally Over?
- REBEL EM: The SPLIT Trial – Saline vs Plasma-Lyte Fluid Therapy
Post-Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post REBEL Cast Ep108: The PLUS Trial – Balanced vs Unbalanced Fluids in the Critically Ill appeared first on REBEL EM - Emergency Medicine Blog.