
 Background: Headache accounts for approximately 2% of all ED visits. One of the most serious etiologies of headache is aneurysmal subarachnoid hemorrhage (SAH), which accounts for 4 – 12% of ED patients with thunderclap headache. There have been several studies in the past few years suggesting that in neurologically intact patients, the sensitivity of modern CT scanners for SAH approaches 100% if performed within 6 hours of headache onset and interpreted by qualified radiologists. If true this data suggests that an LP may not be necessary to rule out SAH and an initial negative CT can be considered a rule-out test.
Background: Headache accounts for approximately 2% of all ED visits. One of the most serious etiologies of headache is aneurysmal subarachnoid hemorrhage (SAH), which accounts for 4 – 12% of ED patients with thunderclap headache. There have been several studies in the past few years suggesting that in neurologically intact patients, the sensitivity of modern CT scanners for SAH approaches 100% if performed within 6 hours of headache onset and interpreted by qualified radiologists. If true this data suggests that an LP may not be necessary to rule out SAH and an initial negative CT can be considered a rule-out test.
REBEL Cast Episode 21: Sensitivity of Early Brain CT to Exclude Aneurysmal Subarachnoid Hemorrhage
Click here for Direct Download of Podcast
What Paper are we Discussing Today?
Dubosh NM et al. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Stroke 2016. [epub ahead of print]. PMID: 26797666
Whats the Clinical Question we are Trying to Answer?
What is the sensitivity of Early Brain CT (Within 6 Hrs) to Exclude Aneurysmal Subarachnoid Hemorrhage?
What They Did:
- Systematic Review and Meta-Analysis to determine the sensitivity of brain CT using modern (16-slice or greater) scanners when performed within 6 hours of headache onset to exclude SAH in neurologically intact patients
- Excluded studies involving traumatic SAH, patients younger than 15 years of age, older generation scanners, and those in which CT was not performed within 6 hours of headache
Outcomes:
- Determine the diagnostic accuracy of early CT only in diagnosis of spontaneous SAH
- Determine the sensitivity, specificity, positive LR, and negative LR of a brain CT performed within 6 hours of headache onset using modern generation scanners in the diagnosis of spontaneous SAH
Results:
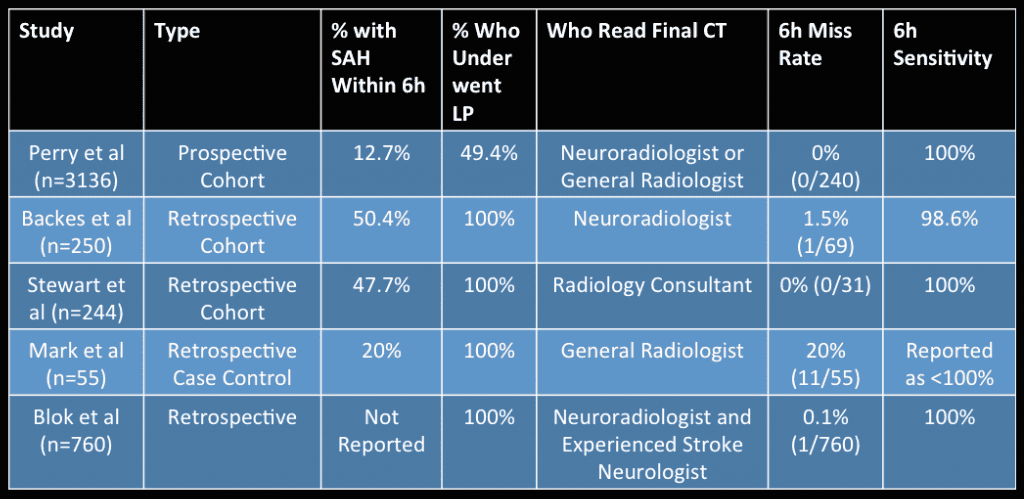
- 5 trials included with 8907 patients
-
Worst Case Scenario
- 13 missed SAH (incidence 1.46/1000) on brain CT within 6 hours
- Pooled Sensitivity: 0.987 (95% CI 0.971 – 0.994)
- Pooled Specificity 0.999 (95% CI 0.993 – 1.0)
- Pooled +LR 921.9 (95% CI 139 – 6103)
- Pooled -LR 0.010 (95% CI 0.003 – 0.034)
-
Intermediate Case Scenario
- 9 missed SAH on brain CT within 6 hours
- Pooled Sensitivity 0.989 (95% CI 0.980 – 0.994)
- Pooled Specificity 1.0 (95% CI 0.993 – 1.0)
-
Excluding 2 Studies Without Direct Information
- Pooled incidence of SAH was 19.1%
- 1/1155 missed SAH (incidence 0.87/1000) on brain CT within 6 hours
- Overall Sensitivity: 0.986 (95% CI 0.951 – 0.996)
- Overall Specificity 0.996 (95% CI 0.974 – 0.999)
Strengths:
- Used Cohen unweighted kappa to measure chance corrected agreement between reviewers
- Assessed quality of included studies with Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool
Limitations:
- There was significant variation in the incidence of SAH among the studies
- The index (gold standard) test was a validated method for diagnosis of SAH including CT or cerebrospinal fluid analysis, and clinical follow-up, however the index test was applied unevenly across the 5 studies, which could introduce bias
- The studies by Blok and Mark et al, only included patients with negative CTs, so estimations of their true positives and negatives had to be made using the Perry et al study numbers for incidence of 12.7% and the proportion of SAH patients who presented within 6 hours, which was 30%
- The study that contributed the largest number of patients did not perform LP in all patients, which could lead to overestimation of CT sensitivity
- Included studies had incidences of SAH that seem higher than what is typically seen in clinical practice
Discussion:
- LPs are associated with patient anxiety and discomfort and can be complicated by post procedure headache (15 – 20% of patients). Traumatic taps, which occur in 10 – 15% of patients, may lead to unnecessary vascular imaging and other downstream testing.
- The Mark et al study had 11 missed cases of SAH, including 7 patients who had vascular anomalies on cerebral angiography, but from the data available, it is not possible to know if these were true aneurysmal SAH or incidental vascular lesions on imaging.
- In the Blok et al study, 760 patients had negative CTs within 6 hours of headache onset, but 52 had CSF positive for bilirubin and only 1 of these was a SAH, but it was a nonaneurysmal, perimesencephalic SAH.
- Some important considerations to think about:
- Headache has a differential diagnosis, and further testing beyond CT may be needed to rule out other etiologies
- CT sensitivity is dependent on the technology of the CT scanner itself and who is interpreting the scans themselves (Trainees and nonexperts have a higher rate of errors in interpretation)
Author Conclusion: “In patients presenting with thunderclap headache and normal neurological examination, normal brain CT within 6 hours of headache is extremely sensitive in ruling out aneurysmal SAH.”
Clinical Take Home Point: A negative head CT in a neurologically normal patient, with a thunderclap headache presentation, a clear time of onset, and a modern CT scanner performed within 6 hours of onset read by an attending radiologist results in a post test risk of SAH of 1 – 2/1000 patients. A shared decision strategy should be used to balance the risk and benefits of performing a lumbar puncture versus a negative CT within 6 hours being sufficient to rule out SAH.
References:
- Dubosh NM et al. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Stroke 2016. [epub ahead of print]. PMID: 26797666
For More Thoughts on This Topic Checkout:
- Ryan Radecki at EMLitofNote: Is the 6-Hr CT for SAH Debate Over?
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)
The post REBEL Cast Episode 21: Sensitivity of Early Brain CT to Exclude Aneurysmal Subarachnoid Hemorrhage appeared first on REBEL EM - Emergency Medicine Blog.