
 The use of heated and humidified high flow nasal cannula (HFNC) has become increasingly popular in the treatment of patients with acute respiratory failure through all age groups. Over the past several years, many studies have come out reviewing the mechanisms of action as well as its use in a variety of conditions. In this episode, I will summarize how it works and for part 2, I will discuss the main indications for its use in both adult and pediatric patients and practical tips on how to use it.
The use of heated and humidified high flow nasal cannula (HFNC) has become increasingly popular in the treatment of patients with acute respiratory failure through all age groups. Over the past several years, many studies have come out reviewing the mechanisms of action as well as its use in a variety of conditions. In this episode, I will summarize how it works and for part 2, I will discuss the main indications for its use in both adult and pediatric patients and practical tips on how to use it.
REBEL Crit Cast Episode 2.0 – Overview of High Flow Nasal Cannula (HFNC) – Part 1
What is HFNC?
- It is NOT standard nasal cannula cranked up to high flow rates
- It is a device made by different companies that can provide up to 50-60L of flow and 21 – 100% FiO2
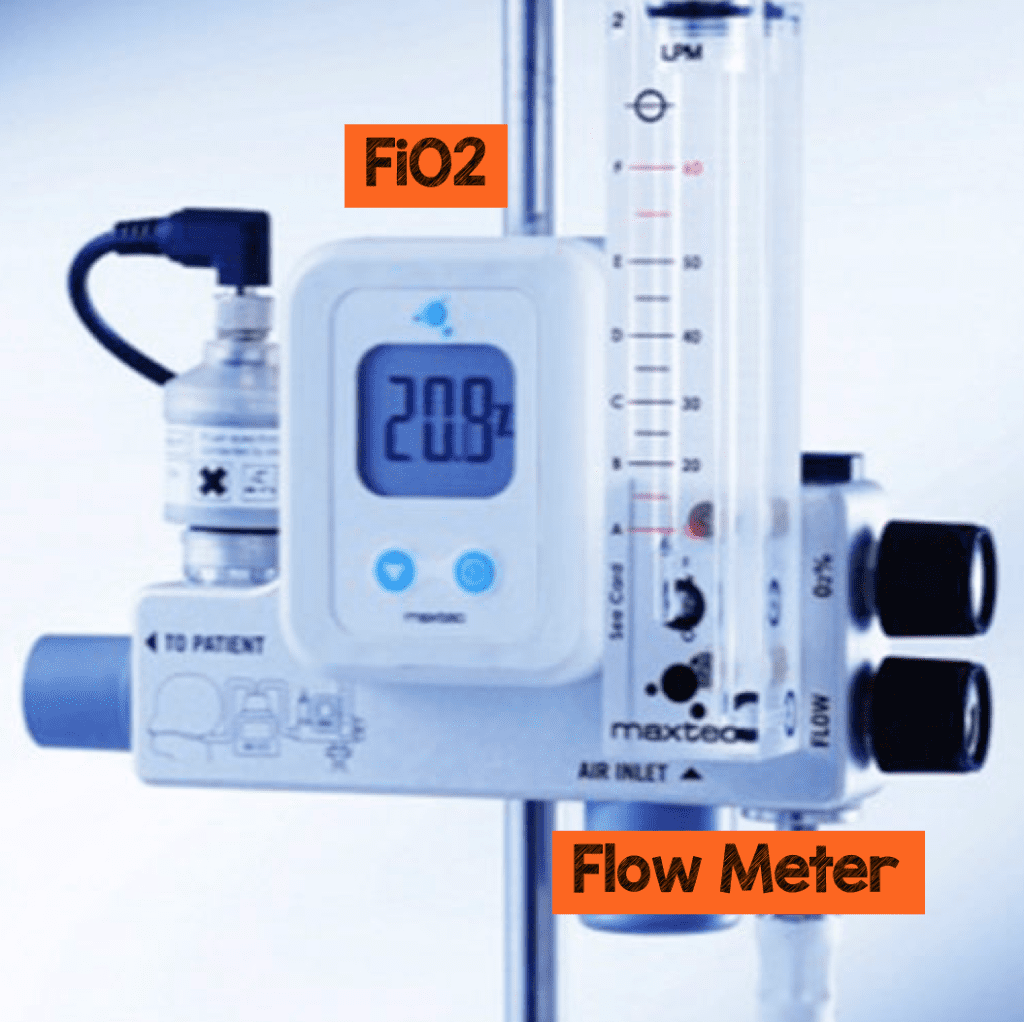
- You can separately dial in high flow rates and varying amounts of FIO2 to meet patient needs
- The key is that the device warms (37°) and humidifies (100% humidity) the gas before reaching the patient
- If the device didn’t warm & humidify the gas, the cold, dry air at these flow rates would not be tolerated by your patient and could be potentially harmful
How Does HFNC work?
- I will use the mnemonic H-I-F-L-O-W to discuss HFNC mechanisms of action
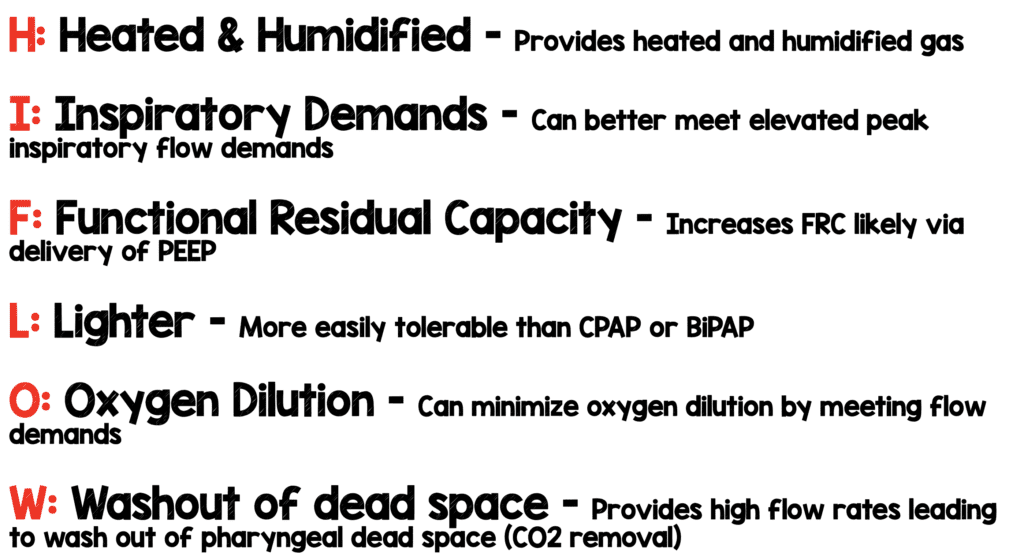
“H”: Heating and Humidification
- HFNC heats air to 37° C and humidifies it to 100% humidity
- This can help ciliary function by facilitating mucous clearance and thinning secretions
- Prevents bronchospasm and increased airway resistance
- Decreases inflammation in the airway
- Decrease energy expenditure (ATP production) needed to heat and humidify gas which may be important in your critically ill patients in shock
“I”: Decreasing Inspiratory Demand
- Example: 70kg patient is in respiratory failure breathing with flow demand of 16L ( ex. RR = 40 breathes/min & Tidal Volume = 400mL TV (MV = RR x TV)).
- Treatment options:
- Low Flow Nasal Cannula = Max 6L (not enough)
- Nonrebreather 15L (still not good enough)
- HFNC 40 – 60L
- HFNC exceeds patients MV and flow needs and therefore should decrease their inspiratory demands
- If therapy is effective by meeting and exceeding patient flow demands, their RR and WOB should improve
“F”: FRC (Functional Residual Capacity)
- Controversial evidence to support how much PEEP provided by HFNC
- Difficult to measure PEEP, as significant amounts of pressure can be lost especially if patients mouth is open
- Adult and pediatric studies have examined impedance tomography (noninvasive measure of end-expiratory lung volumes or lung expansion)
- Patients on HFNC seen to have increased end-expiratory lung expansion and end-expiratory lung volumes
- Patients observed to have decreased end-expiratory lung expansion coming off HFNC
- Likely that HFNC increases FRC by increasing PEEP
“L”: Lighter
- HFNC maybe a more comfortable alternative to NIPPV (CPAP or BiPAP) or invasive PPV such as endotracheal intubation
- Parents of pediatric patients and adult patients have described more comfort with HFNC compared to other forms of NIPPV as well as endotracheal intubation
“O”: Oxygen Dilution
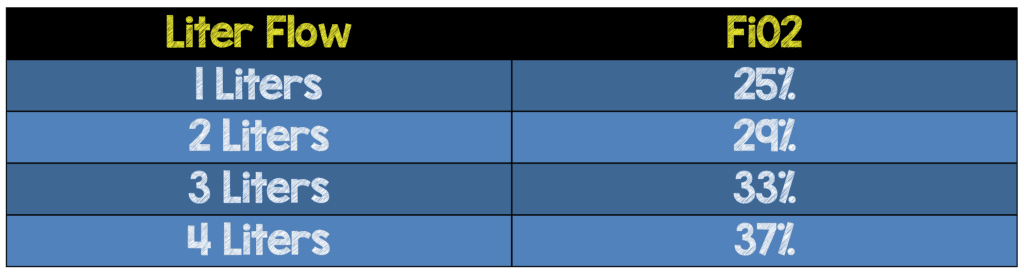
- Rule of “4 to 1” goes like this” if you give someone 1L of nasal cannula (NC), it adds about 4% FiO2 over and above Room Air (21%)
- 1L = 4% + Room Air = 21% so 1L should give 25% Fi02, 2L = 29%….6L = 45%
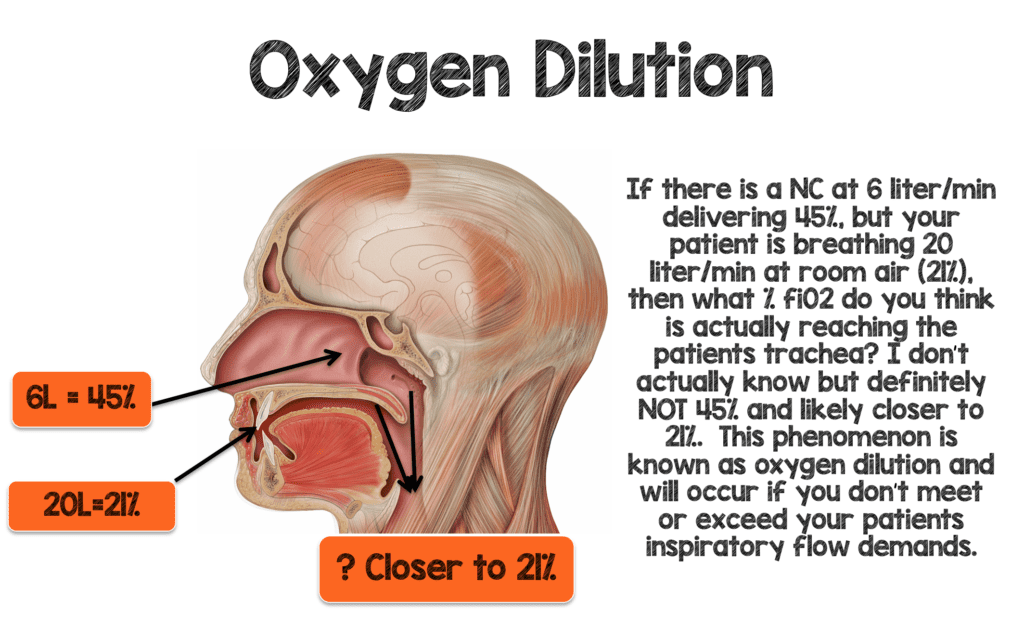
- Consider the patient in respiratory failure, breathing 16L/min (MV = 40RR x 400cc TV)
- Treatment options:
- 6L through the NC
- According to “4:1 Rule” this should deliver FiO2 = 45% to the trachea
- Patient not likely receiving anywhere near 45% as their MV = 16L which through the mouth and nares (around the NC) they are breathing Room Air (21%)
- So gas reaching trachea much closer to 21% due to O2 Dilution
- 6L through the NC
-
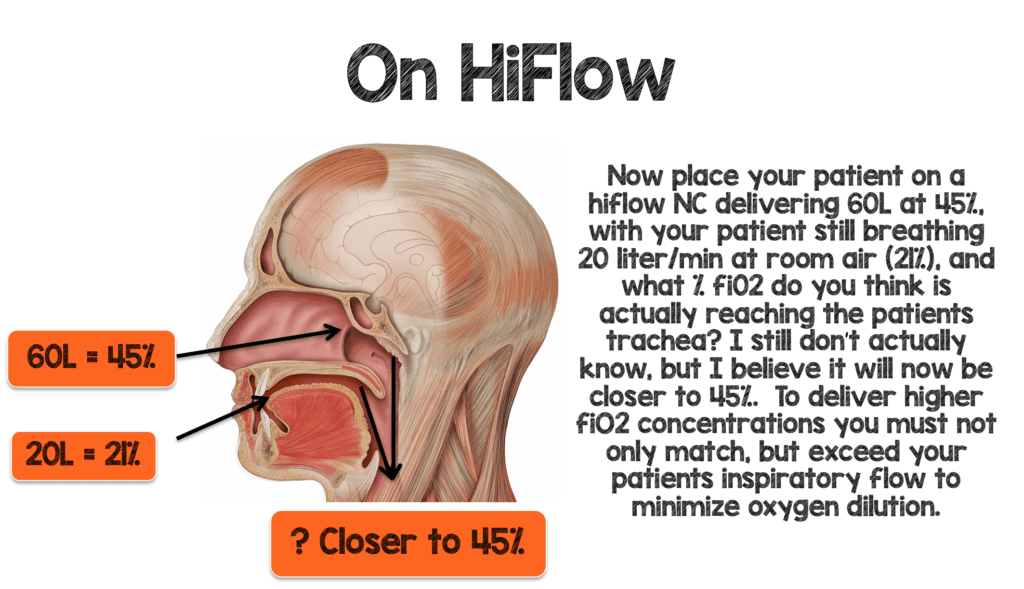
- If you deliver 60L at 45% FiO2 through HFNC
- Providing much higher flow rate than patients inspiratory demands (MV = 16L) than this high flow rate will likely deliver close to 45%
- There will be some Oxygen Dilution, but now gas will be closer to 45% due to the high flow rates delivered by HFNC
- If you deliver 60L at 45% FiO2 through HFNC
-
- HFNC will deliver much higher FiO2 with less dilution, which will definitely benefit patients in terms of hypoxemia
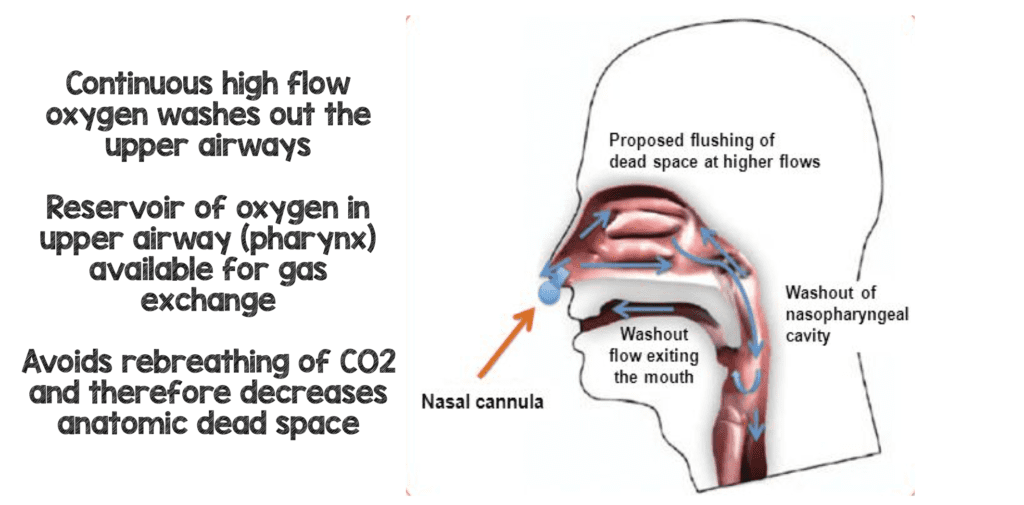
“W”: Washout of Dead Space
- Again, consider a 70kg in respiratory failure breathing with MV = 16L
- Now imagine how much of that inhaled 400mL inhaled gas gets to the lungs?
- Only a small portion of this gas reaches the alveoli as it mixes with the previously exhaled gas (anatomical dead space) filled with CO2
- If we deliver high flow rates (50 – 60L) at 100% FiO2, this can washout this exhaled gas sitting in the upper airway (anatomic dead space) and replace it with fresh 02 rich gas
- This will lead to the patient rebreathing much less CO2 and more fresh O2 rich gas, improving breathing efficiency and decreasing PaCO2 levels
Clinical Bottom Line:
In summary, these different mechanisms described above may all benefit patients in different ways. We are not sure which mechanism is the most important or if they are all helpful. Perhaps, depending on your patient’s condition, one of the mechanisms may be predominate at certain times. One mechanism may be more important in certain disease processes. We will discuss the adult & pediatric indications as well as some practical tips for it’s use in our next podcast!
References:
- Chidekel, A et al. The Effects of Gas Humidification with High-Flow Nasal Cannula on Cltured Human Airway Epithelial Cells. Pulmonary Medicine 2012. PMID: 22988501
- Dysart, K et al. Research in High Flow Therapy: Mechanisms of Action. Respiratory Medicine 2009. PMID: 19467849
- Katz, JA et al. Inspiratory Work with and Without Continuous Positive Airway Pressure in Patients with Acute Respiratory Failure. Anesthesiology 1985. PMID: 3904528
- Parke R et al. Pressures Delivered by Nasal High Flow Oxygen During all Phases of the Respiratory Cycle. Respiratory Care 2013. PMID: 23513246
- Frat JP et al. High-Flow Nasal Oxygen Therapy and Noninvasive Ventilation in the Management of Acute Hypoxemic Respiratory Failure. Annals of Translational Medicine 2017). PMID: 28828372
- Riera J et al. Effect of High-Flow Nasal Cannula and Body Position on End-Expiratory Lung Volume: A Cohort Study Using Electrical Impedance Tomography. Respiratory Medicine 2013. PMID: 23050520
- Roca O et al. Patients with New York Heart Association Class III Heart Failure may Benefit with High Flow Nasal Cannula Supportive Therapy: High Flow Nasal Cannula in Heart Failure. Journal Crit Care 2013. PMID: 23602035
- Möller W et al. Nasal High Flow Clears Anatomical Dead Space in Upper Airway Models. Journal of Applied Physiology 2015). PMID: 25882385
- Lodeserto, F et al. High-flow Nasal Cannula: Mechanisms of Action and Adult and Pediatric Indications. Cureus 2018. PMID: 30740281
Post Written By: Jeffrey Rickert DO
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Crit Cast Episode 2.0: Overview of High Flow Nasal Cannula (HFNC) – Part 1 appeared first on REBEL EM - Emergency Medicine Blog.