
 Background: Antibodies targeted at the SARS-CoV2 spike protein are an essential part of the body’s immune response to COVID19 infection. Infection with SARS-CoV2 stimulates the immune system to produce a polyclonal spike protein antibody response in the host. Vaccines have similar results and recent studies show that the antibody response is even more robust than with natural infection. These antibodies bind to numerous locations on the SARS-CoV2 spike protein limiting the virus’s ability to enter and infect host cells.
Background: Antibodies targeted at the SARS-CoV2 spike protein are an essential part of the body’s immune response to COVID19 infection. Infection with SARS-CoV2 stimulates the immune system to produce a polyclonal spike protein antibody response in the host. Vaccines have similar results and recent studies show that the antibody response is even more robust than with natural infection. These antibodies bind to numerous locations on the SARS-CoV2 spike protein limiting the virus’s ability to enter and infect host cells.
One of the many massive challenges of the COVID19 pandemic has been the lack of targeted therapeutics. Extensive efforts have been invested into research with only glimmers of benefit for most drugs. The exception to this has been dexamethasone which was shown in the RECOVERY trial to have remarkable impacts on death in patients requiring O2 (NNT = 29) and in those requiring invasive ventilation (NNT = 8.5). The RECOVERY Group has continued to perform excellent research but most of the investigated therapeutics including azithromycin, convalescent plasma, aspirin and colchicine have all fallen flat.
Monoclonal antibody infusions have gained national attention as a potential therapeutic in COVID patients and have been touted by medical experts. The goal of these drugs is to give patients antibodies prior to their body mounting a response in an effort to prevent progression of disease. We have previously reviewed the EUA drug bamlanivimab (LY-CoV555) – a monoclonal antibody. In that review, we note the absence of any difference in patient centered outcome as well as serious methodological flaws. We have also reviewed REGN-COV2 (casirivimab/imdevimab) noting the lack of any evidence of benefit as well as the suspect methodology. In January, in a post for Brief 19, I concluded that “there is no convincing data that monotherapy or a cocktail of antibodies improves meaningful outcomes in patients with COVID19.” However, the RECOVERY group has submitted a new study that was released as a preprint on June 16th, 2021.
Paper: RECOVERY Collaborative Group. Casirivimab and imdevimab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Preprint
Clinical Question: Does a monoclonal antibody cocktail of casirivimab/imdevimab reduce mortality in patients hospitalized with COVID?
Population: Patients admitted to the hospital with clinically suspected or laboratory confirmed SARS-CoV-2 infection > 12 years of age.
Intervention: Casirivimab 4g/imdevimab 4g (REGN-COV) single dose intravenous infusion
Control: Standard of care alone (no placebo)
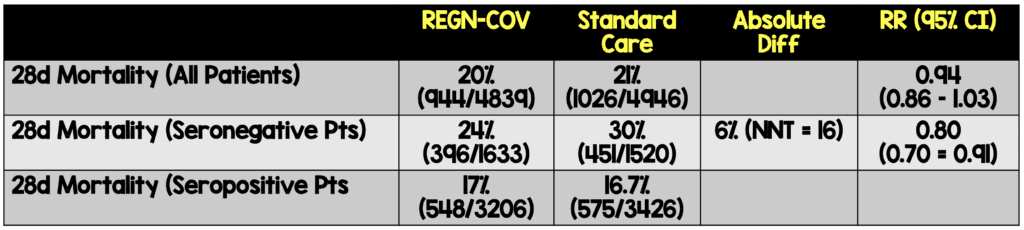
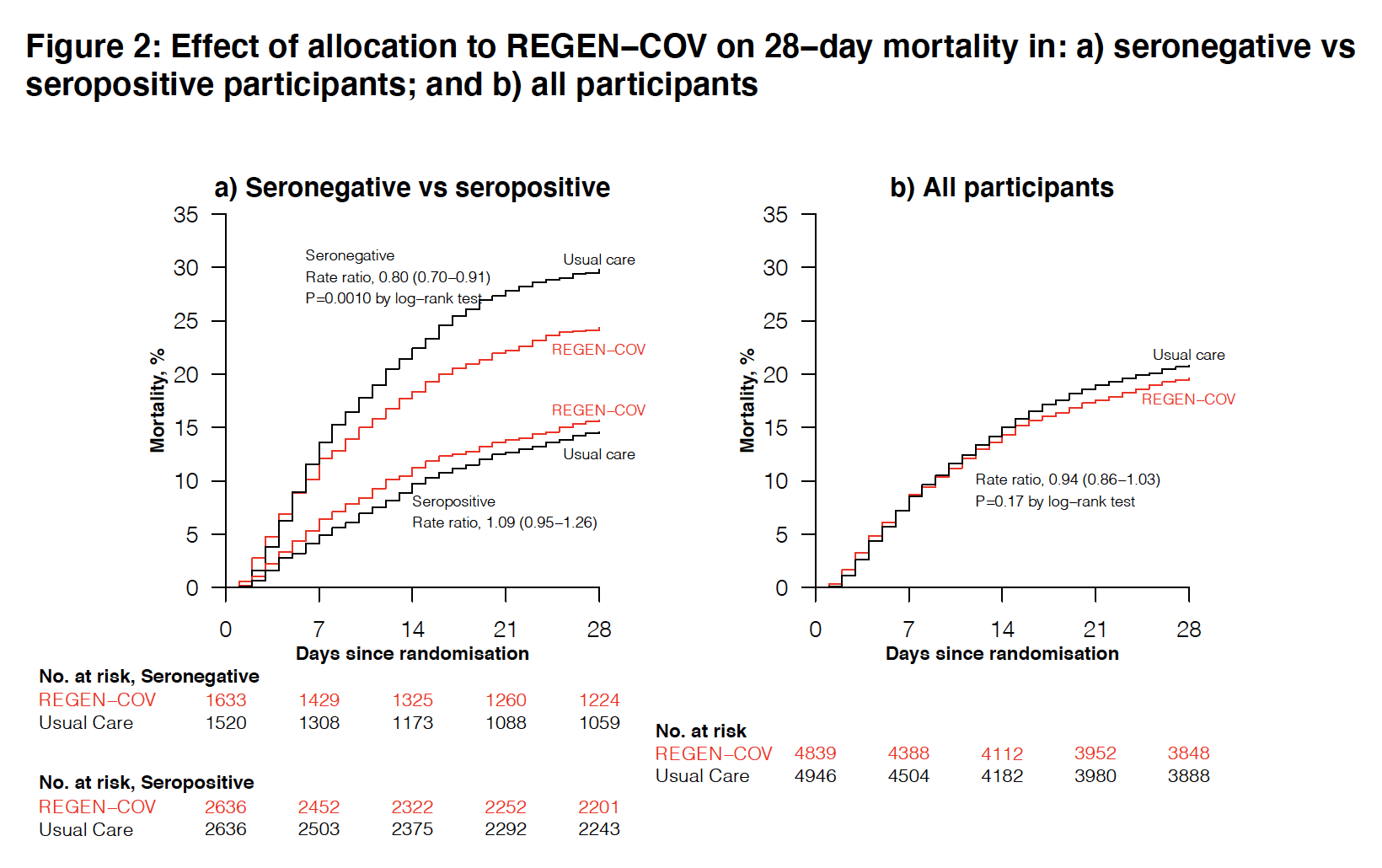
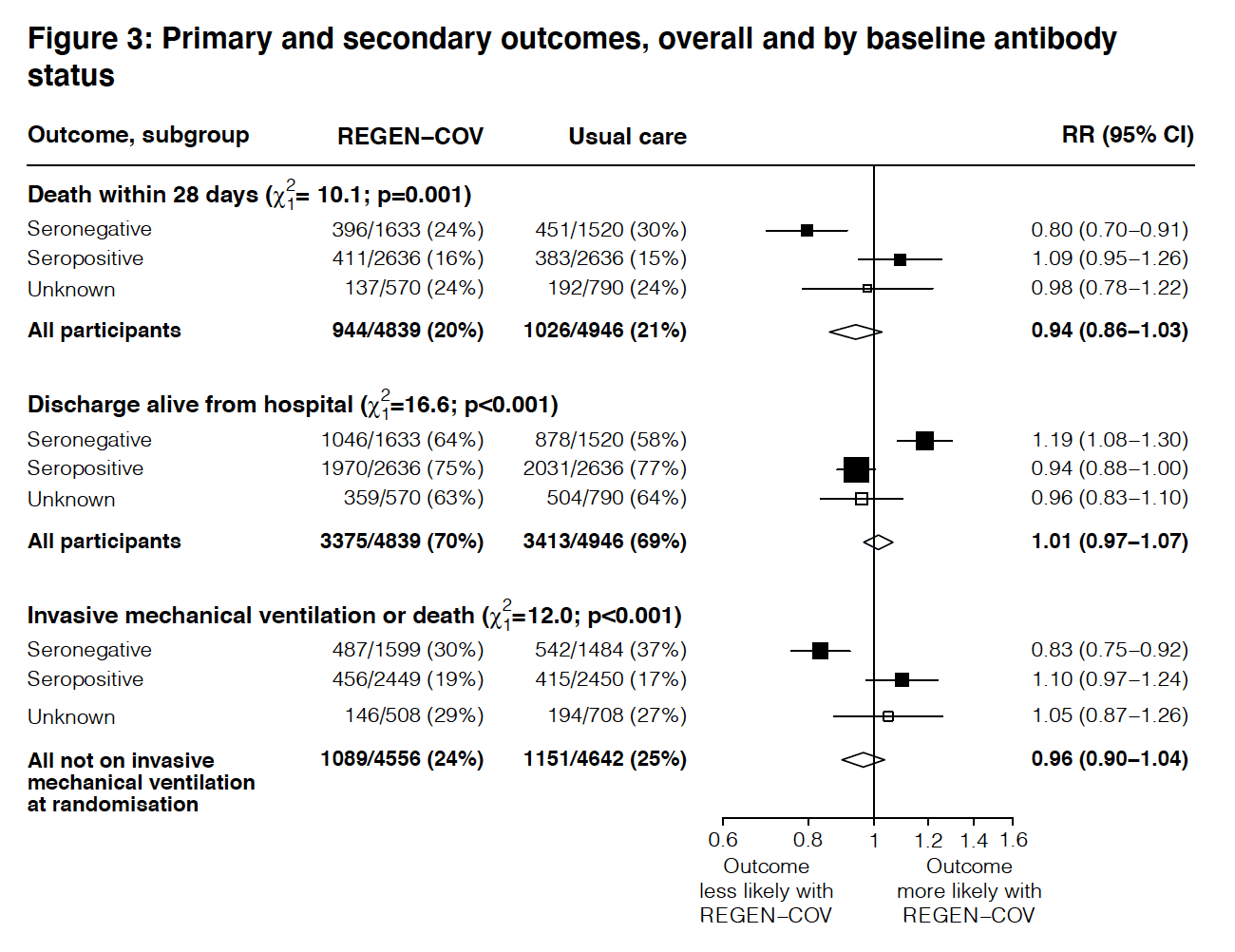
Outcome (primary): 28-day mortality
Outcomes (secondary):
- Time to discharge from hospital
- Composite outcome of invasive mechanical ventilation or death
- Use of invasive or non-invasive ventilation
- Time to successful cessation of invasive mechanical ventilation
- Use of dialysis
Safety Outcomes
- Cause specific mortality
- Major cardiac arrhythmia
- Thrombotic events
- Major bleeding events
Design: Randomized, controlled, open-label, platform trial. This is an adaptive trial that tests different treatment options versus standard care alone to see if that specific treatment has an impact on outcomes.
Excluded:
- Children < 40 kg in weight or < 12 years in age
- Received IVIG during the current admission
- Pregnant or breastfeeding
Primary Results:
-
- 9,785 patients enrolled in this arm of the study
- REGN-COV Group: 4839
- Standard care group: 4946
- Median time from onset of symptoms was 9d (Range 6 to 12 days)
- Serostatus
- Seronegative at baseline: 3153 (32%)
- Seropositive at baseline: 5272 (54%)
- Serostatus unknown: 1360 (14%)
- Respiratory support
- 6.5% did not require O2 on enrollment
- 61% were on simple O2 (no non-invasive or mechanical ventilation)
- 94% of patients received corticosteroids
- Follow up completed for 99% of all patients
- 9,785 patients enrolled in this arm of the study
Critical Results:
 Strengths:
Strengths:
- Study funded by UK Research and Innovation and National Institute of Health Research – No role in study design, data collection, data analysis, data interpretation, writing or reporting.
- Randomized trial with a large sample size and broad eligibility criteria.
- Outcome assessors were masked to treatment assignments.
- Subgroup of seronegative patients established prior to unmasking of data and analysis.
- Groups were well-balanced at baseline
- Follow up complete (99%)
Limitations:
- Regeneron pharmaceuticals supported the study and provided comments on the manuscript – it is unclear what influence these comments had
- Open-label trial: participants and local hospital star were aware of the assigned treatment.
- Patients were not enrolled consecutively (investigator initiated)
- Patients and local staff were not blinded to treatment
Discussion:
- Finding the appropriate patient group that can benefit from this treatment will be a challenge.
- Rapid testing to see if the patient is seronegative or seropositive will be required.
- Many US hospitals still struggle to rapidly test for SARS-CoV2 (many are limited to only testing those who require admission with hours long wait times for results).
- REGN-COV is expensive.
- Though exact costs are difficult to obtain, a report in October 2020 estimated the cost to be between $1500 – $6500.
- This will markedly limit use in the US and virtually prohibit use in countries with lower economic means.
- It’s unclear if REGN-COV will be effective against emerging variants.
- We have already seen monoclonal antibodies lose their efficacy as the predominant variant shifted in different regions.
- The RECOVERY data was collected from September 2020 to May 2021 and likely included a majority of patients with the Alpha variant while Delta variant prevalence in the study group was likely much lower.
- As the Delta variant grows in the share of cases, this monoclonal antibody cocktail may be rendered ineffective as well.
- REGN-COV may still play an important but limited role in COVID-19 treatment.
- While vaccines are cheaper and clearly more effective, there are groups of people who will not achieve the same benefit from them.
- This includes those that have true contraindications to COVID vaccines, those who remain unvaccinated and those who don’t mount as robust a response to vaccines (ie patients on immunosuppressant medications).
- In that latter group, it’s unclear if REGN-COV would offer a benefit.
Author Conclusion: “In patients hospitalised with COVID-19, the monoclonal antibody combination of casirivimab and imdevimab (REGEN-COV) reduced 28-day mortality among patients who were seronegative at baseline.”
Our Conclusions: REGN-COV had no impact on overall mortality amongst patients admitted to the hospital with COVID-19. However, there was a significant reduction in mortality for the subgroup of patients who are seronegative at baseline.
Clinical Take Home Point: This is the first, high-quality data showing a benefit for monoclonal antibodies in patients with COVID19. Application will be limited due to challenges with testing for serostatus, cost and the emergence of resistant variants.
For More Thoughts on This Topic Checkout:
- Brief19: Monoclonal Antibodies Yet. To Show Important Clinical Benefit in Patients with COVID-19
- Brief19: Regeneron’s Antibody Cocktail Shows Promise in the Lab but, Little Difference for Patients
- REBEL EM: BLAZE-1: COVID-19 Neutralizing Antibody (Bamlanivimab)
- REBEL EM: No Evidence that REGN-COV2 (Regeneron) Antibody Cocktail Has Clinical Benefits
- EMCrit: I’m So Confused About Bamlanivimab
- St. Emlyns: REGN Monoclonal Antibodies Work in Selected Hospitalised COVID-19 Patients
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post RECOVERY Trial: The REGN-COV Antibody Cocktail in COVID19 appeared first on REBEL EM - Emergency Medicine Blog.