
 Background: Clinically significant pneumothoraces in patients on mechanical ventilation can be dangerous as positive pressure ventilation can cause an increase in intrapleural pressure and trigger tension physiology. Occult pneumothoraces are those not suspected clinically or not evident on plain radiographs but later identified on computerized tomography (CT) imaging. The pendulum is swinging towards conservative management for occult pneumothoraces. However, minimal evidence supports conservative management of occult, traumatic pneumothoraces in ventilated patients.
Background: Clinically significant pneumothoraces in patients on mechanical ventilation can be dangerous as positive pressure ventilation can cause an increase in intrapleural pressure and trigger tension physiology. Occult pneumothoraces are those not suspected clinically or not evident on plain radiographs but later identified on computerized tomography (CT) imaging. The pendulum is swinging towards conservative management for occult pneumothoraces. However, minimal evidence supports conservative management of occult, traumatic pneumothoraces in ventilated patients.
Paper: Smith JA, Secombe P, Aromataris E. Conservative management of occult pneumothorax in mechanically ventilated patients: A systematic review and meta-analysis. J Trauma Acute Care Surg. 2021 Dec 1;91(6):1025-1040. PMID: 34225346.
Clinical Question: In hemodynamically stable mechanically ventilated patients with occult pneumothorax, what is the effectiveness and safety of conservative management compared to prophylactic ICC insertion?
What They Did:
- The authors performed a systematic review and meta-analysis of multiple databases and considered randomized controlled trials (RCTs) and comparative prospective and retrospective cohort studies for inclusion.
- The paper was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines and registered on the International Prospective Register of Systematic Reviews (PROSPERO: CRD42019132958).
Inclusion Criteria
- Patients of any age diagnosed with a blunt or penetrating traumatic occult pneumothorax on thoracoabdominal CT scan receiving mechanical ventilation.
Exclusion Criteria:
- Patients with occult hemopneumothorax
Outcomes:
Main Outcomes
- Intercostal Catheter insertion
- Incidence of tension pneumothorax (diagnosed clinically)
- Incidence of pneumothorax progression (seen on Chest x-ray)
- Incidence of pneumonia/empyema
Additional Outcomes
- Mortality
- ICC insertion (tension pneumothorax)
- ICC insertion (progression to simple pneumothorax)
- ICC insertion (non-pneumothorax reasons)
- Length of stay in hospital and Intensive Care (days)
- Duration of mechanical ventilation (hours)
- Hemodynamic instability (measured as need for vasopressor support)
- Pain (measured by validated pain scoring tools for sedated ICU patients, i.e., Behavioural pain scale (BPS) and Critical-Care Pain Observation Tool (CPOT))
- Analgesia requirements (measured in parenteral morphine equivalents per 24 hours as per ANZCA opioid conversion)
Results:
Paper Selection:
- Researchers identified 3,356 articles.
- 2,230 records remained after the elimination of duplicates.
- 2,210 records were excluded after screening.
-
Researchers performed a full-text review of 20 publications.
- 2 additional articles were identified from reference lists.
-
12 studies included
- 3 RCTs
- 9 cohort studies (2 prospective and 7 retrospective)
-
354 total participants
- 178 in the RCTs and 176 in the cohort studies
Critical Results
-
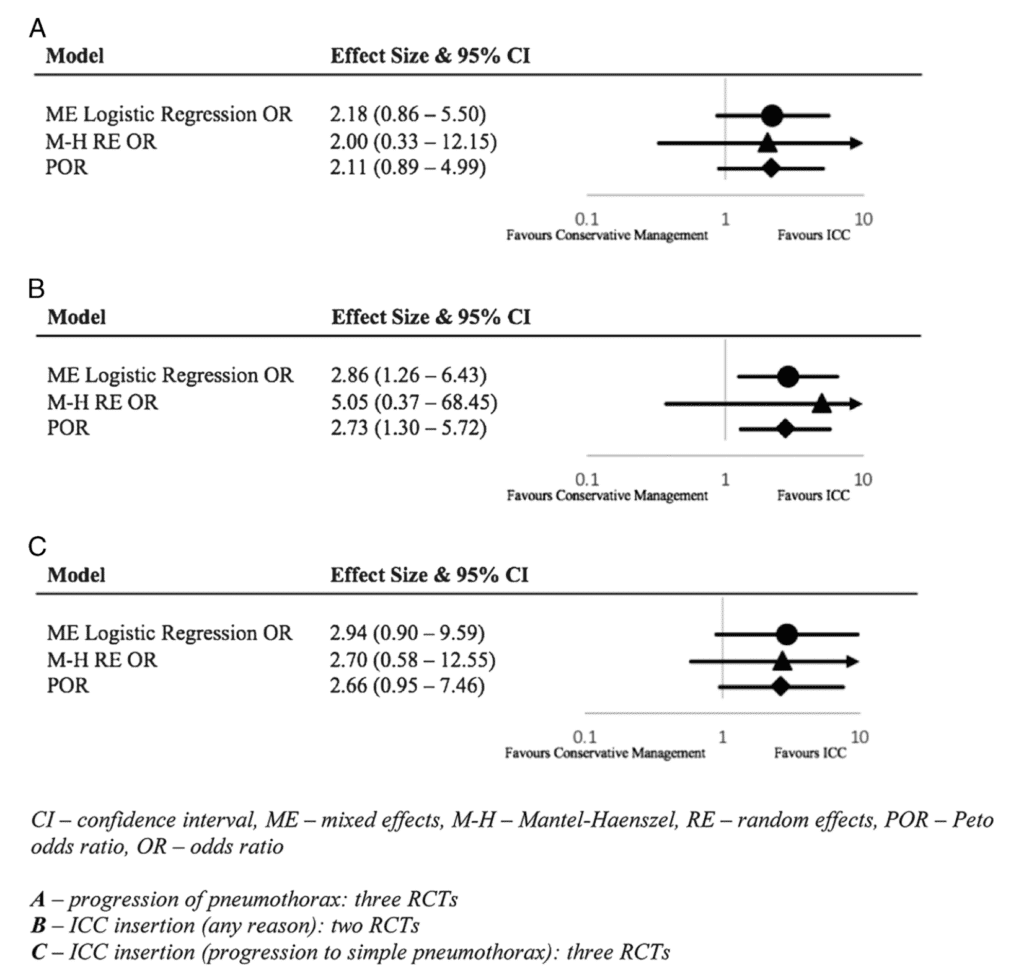
ICC insertion for any reason
- There was a statistically significant difference favoring prophylactic ICC insertion group for the outcome of ICC insertion for any reason
- 2 RCTs, including high-quality trial
- Logistic Regression OR , 95% CI 2.86 (1.26–6.43)
-
Progression of Pneumothorax
- There was a non-statistically significant trend of progression of pneumothorax in the conservative group favoring the ICC insertion group
- Informed by all 3 RCTs, including low and high qualities
-
Length of stay
- No difference in RCTs
- 2 cohort studies suggested conservative management had shorter LOS
-
Duration of mechanical ventilation
- No difference
-
Tension pneumothorax
- Low incidence in both groups (2.8% in conservative, .5% in ICC group)
-
ICC complications
- 19.5% in ICC group, 5.8% in conservative management when ICC was required
- RCTs Logistic Regression Odds Ratio: 0.12 (0.02-0.62 95% Confidence Interval)
-
Incidence of pneumonia/empyema
- no statistically significant difference
- RCTs Logistic Regression Odds Ratio: 1.92 (0.79-4.70 95% Confidence Interval)
- Cohort Studies Logistic Regression Odds Ratio: 0.7 (0.19-2.5 95% Confidence Interval)
-
All-cause mortality
- analysis trended towards conservative management
- RCTs Logistic Regression Odds Ratio: 0.58 (0.15-2.14 95% Confidence Interval)
- Cohort Studies Logistic Regression Odds Ratio: 0.36 (0.1-1.27 95% Confidence Interval)
Strengths:
- The study addresses a patient-centered clinical question that is relevant to ED practice.
-
The authors searched multiple databases comprehensively and included their search strategy making replication possible.
- Contacted authors of included studies for additional information when necessary
- Checked multiple trial registries for unpublished literature
- Included studies from multiple countries
- Included all ages
- Included all languages
- Investigators assessed quality with standardized critical appraisal instruments from the Joanna Briggs Institute (JBI).
- Used PRISMA and registered the meta-analysis with PROSPERO, which increases transparency and reproducibility
Limitations:
- The patient population was very broad and heterogeneous.
-
The initial screening process was performed by one reviewer, increasing the potential for the omission of relevant articles.
- Additional reviewers were used if there were uncertainties.
- Only 3 of 12 studies were RCTs
- Many of the studies included patients who were not mechanically ventilated. Only 1 RCT and 1 cohort study had only mechanically ventilated patients.
- Neither patients, physicians, nor outcome assessors were blinded in the included RCTs.
- Small sample size, leading to wide confidence intervals and low certainty of findings.
- Two cohort studies did not report complete data for the ICC group and, therefore, could not be included in any analyses.
- The authors did not discuss explanations for between-study differences.
- It is unclear what criteria were used to determine hemodynamic instability.
- It is unclear if the results would be similar across the range of included patients (young vs. old, sick vs. less sick, etc.).
- One trial had higher rates of ICC insertion and progression of pneumothorax which inflated some data.
Discussion:
- The inclusion criteria were extensive and included all patients of any age with occult pneumothorax from blunt and penetrating trauma. More stringent inclusion criteria would likely decrease the number of potential studies available for inclusion. While pragmatic, we cannot assume a young, otherwise healthy injured child would respond like an elderly patient with comorbid conditions. The patient population appears too heterogeneous to pool in a systematic review and meta-analysis.
- There was a statistically significant difference in ICC insertion “for any reason” between the two groups. However, the outcome is somewhat misleading. In a comparison of patients with an occult traumatic pneumothorax who were treated with either conservative management or prophylactic ICC insertion, it seems obvious that patients in the prophylactic ICC insertion group would have more chest tubes.
- However, this data was driven by a single small trial (Enderson et al.), which found higher incidences of pneumothorax progression. The authors performed a sensitivity analysis with the Enderson paper removed, which showed a dramatic reduction in the effect size.
- The thirteen included publications contained numerous deficiencies. For example, only two publications included patients exclusively mechanically ventilated. The total sample size of 355 patients is relatively small, and approximately 40% came from just one publication.
- Additionally, many studies contained significant bias. Just ⅔ s of the papers were randomized. Patients were treated the same other than the intervention in only ⅓ of the RCTs. Neither patients, treating clinicians, nor outcome assessors were blinded in any RCTs. Outcomes were measured the same in only ⅓ of all included papers.
- While the data is thought-provoking, included trials have too many inherent flaws to draw any meaningful conclusion or drive practice change.
AUTHORS CONCLUSIONS: “More evidence is required to fully inform the effectiveness of conservative management for occult pneumothoraces in mechanically ventilated patients. However, the evidence we have to date suggests that conservative management is a safe alternative to prophylactic ICC insertion for the initial management of occult pneumothoraces in mechanically ventilated patients, provided that the patients are in a highly monitored environment, the treating clinicians are aware that the patient has an occult pneumothorax and that there is appropriate staff available to recognize and treat tension pneumothorax if it occurs.”
Our Conclusion:
While interesting, the data in this systematic review and meta-analysis are derived from publications with small sample sizes and a serious risk of bias. There is not enough high-quality evidence to draw firm conclusions.
References:
Smith JA, Secombe P, Aromataris E. Conservative management of occult pneumothorax in mechanically ventilated patients: A systematic review and meta-analysis. J Trauma Acute Care Surg. 2021 Dec 1;91(6):1025-1040. PMID: 34225346.
Guest Post By:

Patrick Callan, DO
PGY-1, Emergency Medicine Resident
Vassar Brothers Hospital, Poughkeepsie, New York
E-mail: patrick.callan@nuvancehealth.org
Marco Propersi, DO FAAEM
Vice-Chair, Emergency Medicine
Assistant Emergency Medicine Program Director
Vassar Brothers Hospital, Poughkeepsie, New York
Twitter: @marco_propersi
Post-Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie), Anand Swaminathan, MD (Twitter: @EMSwami)
The post Shifting the Paradigm: Can We Manage Mechanically Ventilated Patients with Occult Traumatic Pneumothorax Conservatively? appeared first on REBEL EM - Emergency Medicine Blog.