
 Background: Acute basilary artery occlusion has a high morbidity and mortality. Treatment strategies for acute basilar artery occlusion are rather sparse. Endovascular research over the last 5 years (REBEL EM Post) adds little to the conversation of these strokes as very few patients with basilar artery strokes were included. The Basilar Artery International Cooperation Study (BASICS) was a prospective observational registry in which ≈600 patients were divided into three groups: antithrombic treatment only (antiplatelet drugs or systemic anticoagulation), primary intravenous thrombolysis (including subsequent intra-arterial thrombolysis), or intra-arterial therapy (which compromised thrombolysis, mechanical thrombectomy, stenting, or a combination of these approaches) [2]. The majority of patients (68%) received intra-arterial therapy, but the study showed no statistically significant superiority for any treatment strategy. In a subgroup analysis of the BASICS registry, patients with the most severe neurologic deficits (NIHSS >19) showed a trend toward lower risk of a poor neurologic outcome with endovascular therapy. Clearly, additional data is needed to elucidate the role of endovascular treatment in basilar artery strokes.
Background: Acute basilary artery occlusion has a high morbidity and mortality. Treatment strategies for acute basilar artery occlusion are rather sparse. Endovascular research over the last 5 years (REBEL EM Post) adds little to the conversation of these strokes as very few patients with basilar artery strokes were included. The Basilar Artery International Cooperation Study (BASICS) was a prospective observational registry in which ≈600 patients were divided into three groups: antithrombic treatment only (antiplatelet drugs or systemic anticoagulation), primary intravenous thrombolysis (including subsequent intra-arterial thrombolysis), or intra-arterial therapy (which compromised thrombolysis, mechanical thrombectomy, stenting, or a combination of these approaches) [2]. The majority of patients (68%) received intra-arterial therapy, but the study showed no statistically significant superiority for any treatment strategy. In a subgroup analysis of the BASICS registry, patients with the most severe neurologic deficits (NIHSS >19) showed a trend toward lower risk of a poor neurologic outcome with endovascular therapy. Clearly, additional data is needed to elucidate the role of endovascular treatment in basilar artery strokes.
Paper: Langezaal LCM et al. Endovascular Therapy for Stroke Due to Basilar-Artery Occlusion. NEJM 2021. PMID: 34010530 [Access on Read by QxMD]
Clinical Question: In patients with acute basilar artery occlusion is favorable functional outcome at 90 days improved with endovascular therapy vs standard medical care?
What They Did:
- Basilar Artery International Cooperation Study (BASICS)
- Multicenter, open-label, international, randomized clinical trial of patients with acute basilar artery occlusion
- Trial conducted from 2011 to 2019 in 23 centers from 7 countries
- Randomly assigned patients within 6hrs after time of onset of stroke due to basilar artery occlusion in 1:1 ratio:
- Endovascular therapy
- Standard medical care
Outcomes:
-
Primary: Favorable functional outcome at 90d
- Defined as: modified Rankin score of 0 to 3
- 0 = No disability
- 3 = Moderate disability
- 6 = death
-
Primary Safety Outcome:
- Symptomatic intracranial hemorrhage within 3 days after treatment
- 90d mortality
-
Secondary Clinical Outcomes:
- Excellent outcome (Defined as mRS of 0 to 2)
- NIHSS score at 24hrs
- Distribution of scores on mRS
- Health-related quality of life (Measured on European Quality of Life-5 Dimensions)
Inclusion:
- Original inclusion criteria:
- ≤85 years of age
- Acute signs and symptoms compatible with ischemia in the basilar artery territory
- Proven basilar artery occlusion on CTA or MRA
- NIHSS score of ≥10
- Endovascular therapy had to be feasible within 6hrs and IV thrombolysis in patients assigned to endovascular therapy group had to be initiated within 4.5hrs after the estimated time of stroke
- Due to slow enrollment, 4 years into the trial, after 91 patients had undergone randomization, inclusion criteria were expanded to include:
- 85 years of age or older
- NIHSS <10
- Contraindications to intravenous thrombolysis
Exclusion:
- Intracranial hemorrhage
- Extensive, bilateral brain stem infarction on CT
- Cerebellar mass effect
- Acute hydrocephalus evident on neuroimaging
Results:
- 300 patients enrolled
- IV thrombolysis used:
- Endovascular therapy: 78.6%
- Standard medical care: 79.5%
- Intravenous thrombolysis initiated at a median of ≈2hrs after stroke onset
- Endovascular treatment initiated at median of 4.4hrs after stroke onset
- IV thrombolysis used:
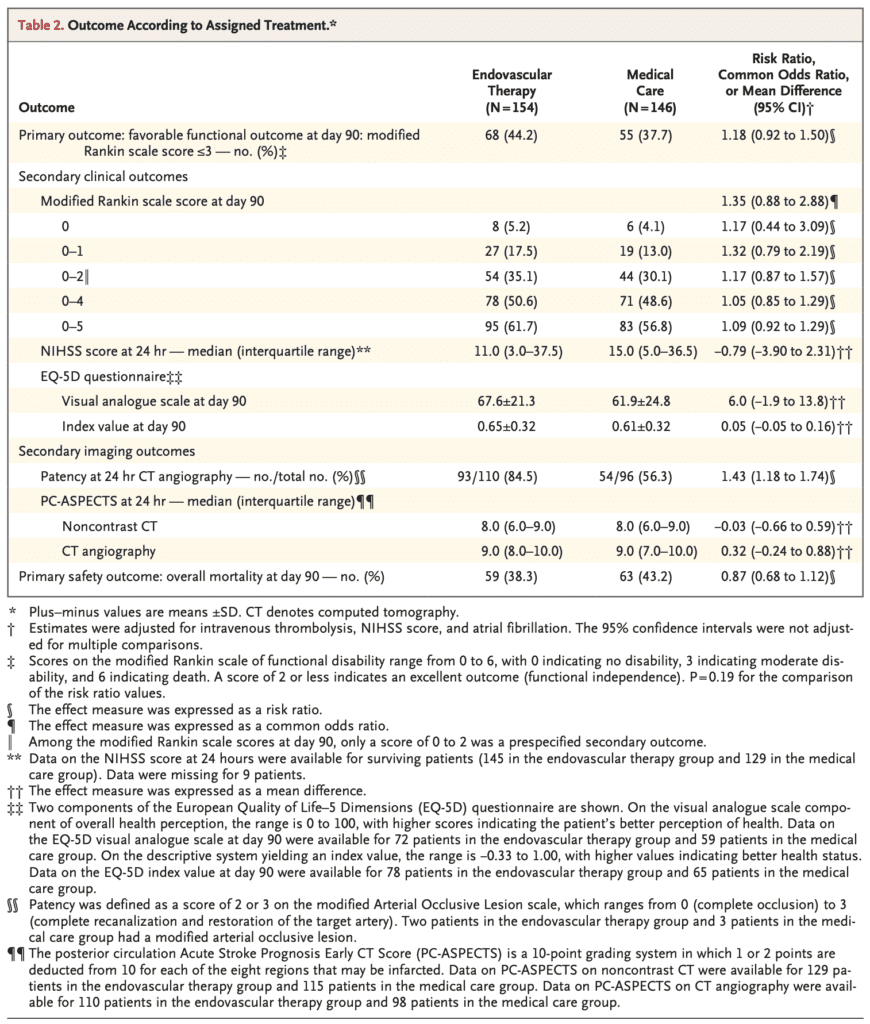
- Favorable Functional Outcome (mRS 0 to 3):
- Endovascular therapy: 44.2%
- Standard medical care: 37.7%
- RR 1.18; 95% CI 0.92 to 1.50; p = 0.19
- Excellent Functional Outcome (mRS 0 to 2):
- Endovascular therapy: 35.1%
- Standard medical care: 30.1%
- RR 1.17; 95% CI 0.87 to 1.57
- Patency of Basilar Artery at 24hrs:
- Endovascular therapy: 84.5%
- Standard medical care: 56.3%
- Symptomatic Intracranial Hemorrhage
- Endovascular therapy: 4.5%
- Standard medical care: 0.7%
- RR 6.9; 95% CI 0.9 to 53.0
- 90d Mortality:
- Endovascular therapy: 38.3%
- Standard medical care: 43.2%
- RR 0.97; 95% CI 0.68 to 1.12; p = 0.29
- Other Outcomes:
Strengths:
- Multicenter, international, randomized clinical trial
- No patients lost to follow-up at 90days
- No primary outcome data were missing
Limitations:
- NIHSS score performed by investigator who was aware of treatment group assignments
- Unblinded trial with subjective outcome of NIHSS score could have caused bias in the primary outcome
- Study too small to draw any definitive conclusions in outcomes. This is evidenced by the wide confidence intervals
- Unable to make statistical comparisons among subgroups
- Originally sought to enroll 750 patients but only enrolled ≈300 patients
- Convenience sample of patients as evidenced by the fact that only 70.8% of 424 eligible patients were randomized
- Patients imbalanced at baseline in terms of incidence of atrial fibrillation (28.6% in the endovascular group and 15.1% in the medical care group)
- Nearly 30% of eligible patients were treated outside the trial and 79.0% of these patients received endovascular therapy. This could have introduced bias in the patients that were enrolled
- Advanced imaging with CT perfusion was not used for patient selection. This is key to understand as patient with infarcted brain will likely have no benefit from endovascular therapy which is evidenced by the high patency rate but no difference in good neurologic outcomes in this study
- NIHSS is less sensitive to symptoms of posterior circulation strokes compared to anterior circulation strokes
Discussion:
- Recruitment of 300 patients over 8 years shows the difficulty in recruitment of patients with basilary artery occlusion. The differences seen in this trial may be meaningful (5% difference in death and 5% difference in good neurologic outcomes) but a much larger study to find this would be needed.
- In regard to the long duration of enrollment, stroke therapy changed quite a bit from 2011 – 2019. The changes and advances in therapy may make a difference as they did with the anterior circulation strokes and endovascular therapy
- Study was underpowered, requiring 712 patients based on observational results from the BASICS registry on basilar artery occlusions. This assumed a 40% favorable outcome in endovascular therapy group and 30% favorable outcome in the medical care group. The power calculation was changed based on evidence from RCTs of anterior circulation strokes receiving endovascular therapy. Data from the anterior circulation strokes assumed a favorable outcome of 46% in the endovascular therapy group while maintaining a favorable outcome of 30% in patients receiving medical care only. Based on this, a new sample size of 282 patients was calculated.
- Unfortunately, this trial doesn’t add much since the techniques used are likely outdated and not using perfusion imaging. Due to the difficulties in enrolling patients, a study like this may never be feasibly done in a reasonable time period to inform clinical practice
Author Conclusion: “Among patients with stroke from basilar-artery occlusion, endovascular therapy and medical therapy did not differ significantly with respect to a favorable functional outcome, but as reflected by the wide confidence interval for the primary outcome, the results of this trial may not exclude a substantial benefit of endovascular therapy. Larger trials are needed to determine the efficacy and safety of endovascular therapy for basilar-artery occlusion.”
Clinical Take Home Point: In patients with basilar artery occlusion, endovascular therapy compared to medical therapy alone was not significantly different with respect to a favorable functional outcome. Although, benefit cannot be excluded based on this trial, a much larger trial would be needed to determine the efficacy and safety of endovascular therapy in these patients. Additionally, the use of advanced imaging (i.e CT perfusion) will most likely be needed to select the appropriate patients for endovascular therapy going forward.
References:
- Langezaal LCM et al. Endovascular Therapy for Stroke Due to Basilar-Artery Occlusion. NEJM 2021. PMID: 34010530 [Access on Read by QxMD]
- Schonewille WJ et al. Treatment and Outcomes of Acute Basilar Artery Occlusion in the Basilar Artery International Cooperation Study (BASICS): A Prospective Registry Study. Lancet Neurol 2009. PMID: 19577962
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post Should we Consider Endovascular Therapy for Acute Basilar Artery Occlusion? appeared first on REBEL EM - Emergency Medicine Blog.