
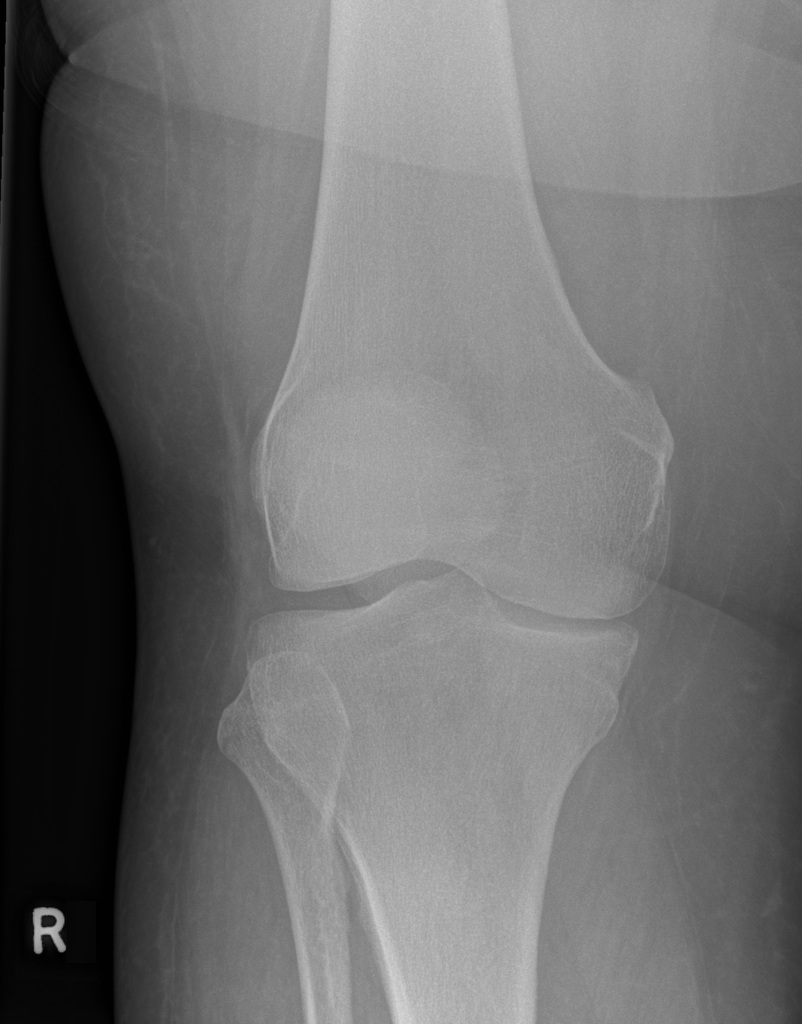
29-year-old F presents to ED with acute onset knee pain. Reports hearing an audible “pop” after twisting her leg while running down the stairs at home. She explains that her right knee is stuck, and she can neither flex nor extend it. An image is shown below (courtesy of Andrew Murphy, Radiopaedia.org)
- Pearl: The most common cause of a locked knee is a bucket-handle meniscus tear [1]. Other causes can be concomitant cruciate ligament injuries, crystal arthropathy, diffuse pigmented villonodular synovitis, or osteoarthritis.
-
Pearl: In patients with chronic knee problems, consider adhesive capsulitis of the knee.
Locked knee syndrome is the inability to flex or extend the knee due to a displaced intra-articular body. A meniscus tear can flip centrally (intercondylar notch), preventing normal flexion and extension [1]. This is often referred to as bucket-handle meniscus tear.
- Pearl: The stump of a complete anterior cruciate ligament (ACL) tear may cause concurrent meniscal tear and locking of the knee [1].
Ligamentous and meniscal injuries of the knee rarely require emergent evaluation in the ED. Initial treatment of these injuries includes RICE therapy (Rest, Ice, Compression, & Elevation) and gentle ROM exercises [2]. At times, the meniscal tear can flip back resulting in a return of range of motion [3]. The patient should be made non-weight bearing and be provided crutches.
- Pearl: Multi-ligamentous injury of the knee requires further assessment – this is an unstable joint with risk for neurovascular injury (eg. popliteal artery dissection).
- Pearl: MRI of the knee without contrast is the imaging of choice as an outpatient, which helps accelerate outpatient surgical management [3]. See the below images.

Image 2. MRI T2 sagittal demonstrating a complete tear of the anterior cruciate ligament. Image courtesy of John Kiel, DO.

Image 3. MRI T2 coronal demonstrating a bucket handle medial meniscus tear. Image courtesy of John Kiel, DO.
Urgent outpatient follow-up with orthopedics. Typically there is no need to consult orthopedics emergently. A locked knee can result in temporary or permanent disability from contractures and flexion deformity. Arthroscopy is warranted if the patient still has a locked knee or has MRI results (such as with this patient) concerning for an intra-articular body. Post-operatively, standard physical therapy should emphasize strengthening of quadriceps, hips, glute muscles, and core coupled with plyometric and proprioceptive training with a return to sports between 6-9 months.
- Pearl: With a locked knee, avoid bracing such as a knee immobilizer. Gentle range of motion should be encouraged [2].
- Pearl: Educate the patient about what will likely happen after their ED visit. If they have further questions you are unable to answer, refer them to their urgent outpatient follow up.
- Pearl: If the patient is an athlete with a local trainer or sports medicine physician, coordinate with them to expedite care as expected within your institution.
References & Resources:
Looking to brush up on knee imaging? Check out the EMRad Archives.
- Agel, J., Rockwood, T., Klossner, D. Collegiate ACL Injury Rates Across 15 Sports: National Collegiate Athletic Association Injury Surveillance System Data Update (2004-2005 Through 2012-2013). Clin J Sport Med. 2016;26(6):518-523. PMID: 27315457
- Fabricant, P. and Jokl, P. Surgical Outcomes After Arthroscopic Partial Meniscectomy. Journal of the American Academy of Orthopaedic Surgeons. 2007;15(11), pp.647-653. PMID: 17989415
- Mohd Miswan, M. F., Latiff Alsagoff, S., Muhamad Effendi, F., & Ibrahim, M. I. The unusual traumatic locked young knee. Malaysian family physician: the official journal of the Academy of Family Physicians of Malaysia. 2019;14(2), 26–28. PMID: 31827732
Author information
{kind=link}
The post SplintER Series: A Case of Inability to Move the Knee appeared first on ALiEM.