
 Background: Each year approximately 790,000 Americans suffer an acute myocardial infarction (AMI) (Benjamin 2017). Traditional treatment for an acute myocardial infarction has included morphine, oxygen, nitroglycerine and aspirin (MONA) with interventions such as percutaneous coronary intervention providing more definitive management. There has been little data from randomized control studies that supports the use of oxygen in AMI. Recent studies such as the AVOID trial suggest that hyperoxia results in harm while a 2016 Cochrane Review suggest no benefit in supplemental oxygen. (Stub 2015, Cabello 2016). There has, however, not been a large randomized control study comparing supplemental O2 to ambient air with patient centered outcomes until the DETO2X-AMI trial.
Background: Each year approximately 790,000 Americans suffer an acute myocardial infarction (AMI) (Benjamin 2017). Traditional treatment for an acute myocardial infarction has included morphine, oxygen, nitroglycerine and aspirin (MONA) with interventions such as percutaneous coronary intervention providing more definitive management. There has been little data from randomized control studies that supports the use of oxygen in AMI. Recent studies such as the AVOID trial suggest that hyperoxia results in harm while a 2016 Cochrane Review suggest no benefit in supplemental oxygen. (Stub 2015, Cabello 2016). There has, however, not been a large randomized control study comparing supplemental O2 to ambient air with patient centered outcomes until the DETO2X-AMI trial.
Clinical Question: Is there a mortality benefit to routine oxygen therapy in patients with suspected AMI who are not hypoxemic at baseline?
Article: Hofmann R et al. Oxygen Therapy in Suspected Acute Myocardial Infarction. N Engl J Med 2017. PMID: 28844200
Population: Adults aged >30 with symptoms suggestive of AMI for less than 6 hours with an O2 saturation > 90% and either EKG changes indicative of ischemia or a positive troponin T who presented to ambulance services, Emergency Departments (EDs), coronary care units or a catheterization laboratory at a participating hospital (35/69 Swedish Hospitals participating in the SWEDEHEART Registry).
Intervention: Supplemental oxygen at 6L/min
Control: Ambient room air
Outcomes:
- Primary: Death from any cause at 1 year
- Secondary: Death from any cause within 30 days after randomization, rehospitalization with myocardial infarction, rehospitalization with heart failure, and cardiovascular death and composites of these endpoints at 30 and 365 days
Design: Registry based, non-blinded, randomized clinical trial
Exclusion: Patients who were receiving ongoing O2 therapy, presentation with cardiac arrest or development of cardiac arrest between presentation and enrollment
Primary Results:
-
6629 patients (3311 in the oxygen group, 3318 in the ambient air group)
-
403 patients did not complete the study (withdrew, change in clinical status, early discharge, communication issues)
- 297 in the oxygen group
- 106 in the ambient air group
-
306 underwent oxygen treatment outside the protocol due to hypoxia
- 62 in the oxygen group
- 254 in the ambient air group
-
403 patients did not complete the study (withdrew, change in clinical status, early discharge, communication issues)
Critical Results:
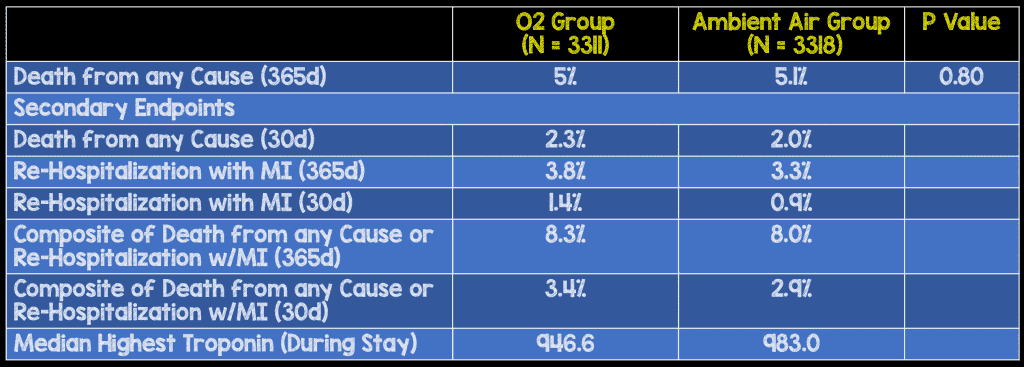
- There is no significant different between the group of patients treated with supplemental oxygen or ambient air in any of the primary or secondary outcomes.
Strengths:
- The study asked a simple, clinically relevant question
- Unlike the prior AVOID trial, the endpoint is patient centered (i.e. death)
- Randomization was appropriately performed
- Most myocardial infarction related outcomes were included between the primary and secondary outcomes
- Follow up was adequate as only Swedish citizens who had a personal identification number were included so the Swedish National Population Registry could be used
- Both populations received the same level of care (i.e. PCI, CABG, coronary Angiography, Aspirin, Beta Blocker, Statin etc…)
Limitations:
- Blinding was not performed as pressurized air was not available at all sites
- Single country study leads to questions of external validity (homogenous population)
- Clinical and procedural end-points were obtained from the SWEDEHEART registry and not prospectively during patient care.
Other Issues: None
Author’s Conclusion: “Routine use of supplemental oxygen in patients with suspected myocardial infarction who did not have hypoxemia was not found to reduce 1-year all-cause mortality.”
Our Conclusion: This multi-site randomized control study suggests that routine supplemental oxygen therapy shows no mortality benefit for patients with suspected myocardial infarction at 1 year.
Potential to Impact Current Practice: Based on this data and previous studies (AVOID trial, 2016 Cochrane Review), it does not appear that there is a benefit of using supplemental oxygen in AMI patients who are not hypoxic at baseline.
Bottom Line: The use of supplemental oxygen does not appear to offer any benefit to patients with acute myocardial infarction in patients with an O2 saturation > 90%. With roughly 790,000 patients in the United States suffering from acute myocardial infarction, there is a potential to save a significant amount of money annually.
Guest Contributor

Brent Dibble, MD
PGY-3 Resident
Bellevue/NYU Emergency Department
For More Thoughts on This Topic Checkout:
- Ryan Radecki at EM Lit of Note: Neither Benefit Nor Harm Seen With Oxygen in Myocardial Infarction
- Rory Spiegel at EM Nerd (EMCrit): The Case of the Liberated Radicals
- ScanCrit: O2 Not Needed in Myocardial Infarction
- Aidan Burrel at The Bottom Line: DETO2X-AMI – Oxygen Therapy in Suspected Acute Myocardial Infarction
- Niall Morris at St. Emlyn’s: JC – Oxygen in ACS. A Fuss About Nothing? The DETO2X Trial
- Ken Milne at The SGEM: Sometimes, All You Need is the Air You Breathe
References:
- Benjamin EJ et al. Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. 2017; 135:e1–e458. PMID: 28122885
- Cabello JB et al. Oxygen therapy for acute myocardial infarction. Cochrane Database Syst Rev 2016;12:CD007160. PMID: 20556775
- Hofmann R et al. Oxygen Therapy in Suspected Acute Myocardial Infarction. N Engl J Med 2017. PMID: 28844200
- Stub D et al. Air versus oxygen in ST-segment-elevation myocardial infarction. Circulation 2015;131: 2143-50. PMID: 26002889
Post Peer Reviewed By: Salim R. Rezaie (Twitter: @srrezaie)
The post The DETO2X Trial: Do Patients with AMI Need Supplemental O2? appeared first on REBEL EM - Emergency Medicine Blog.