
 Background: The standard approach to treating pediatric community-acquired pneumonia (CAP) is a 10-day course of antibiotics. However, two high-quality randomized control trials challenged this standard within the last 12 months. The SAFER Trial [reviewed here] and CAP-IT Trial [reviewed here] found treatment for CAP in children with a shorter duration of antibiotic therapy to be noninferior to standard treatment duration.
Background: The standard approach to treating pediatric community-acquired pneumonia (CAP) is a 10-day course of antibiotics. However, two high-quality randomized control trials challenged this standard within the last 12 months. The SAFER Trial [reviewed here] and CAP-IT Trial [reviewed here] found treatment for CAP in children with a shorter duration of antibiotic therapy to be noninferior to standard treatment duration.
The SCOUT-CAP trial differs from previous RCTs by using a novel combination of clinical response, the persistence of symptoms, and antibiotic-associated adverse effects coupled with the total duration of antibiotic therapy to test for superiority in short-course and standard-course antibiotic strategies for pediatric CAP.
Article: Williams DJ et al. Short- vs. Standard-Course Outpatient Antibiotic Therapy for Community-Acquired Pneumonia in Children: The SCOUT-CAP Randomized Clinical Trial. JAMA Pediatr. 2022;e215547. PMID: 35040920
Clinical Question: “Is a 5-day strategy of antibiotics superior to a 10-day strategy for the treatment of nonsevere pneumonia in young children demonstrating early clinical response?”
What They Did:
- Randomized double-blind placebo-controlled superiority trial
- Performed at eight outpatient sites
- Participants enrolled December 2, 2016–December 16, 2019
- After completing 5 days of antibiotics, children were randomized 1:1 to a strategy of 5 additional days of placebo or 5 additional days of antibiotics.
- Participants were approached between 3–6 days after the start of antibiotics.
Population:
Inclusion:
- Children 6–71 months of age
- Diagnosed with uncomplicated community-acquired pneumonia (CAP) in an outpatient clinic, urgent care, or emergency department.
- AND prescribed either amoxicillin, amoxicillin and clavulanate, or cefdinir
-
Parental report of clinical improvement
- NO Subjective fever or documented temperature 38.3 °C or higher in preceding 24 hours
- NO Tachypnea (50 breaths per min for < 2 years; 40 breaths per min ≥ 2 years old)
- NO Severe cough
Exclusion:
- Treatment with any systemic antibiotic therapy within 7 days before the diagnosis of CAP
- Initial treatment for CAP with combination antibiotic therapy
- History of anaphylaxis or severe drug allergy to study antibiotics
- Presence of concomitant bacterial infection that requires > 5 days of antibiotic therapy
-
Radiographic findings (where applicable) of complicated pneumonia at presentation or any subsequent chest radiograph up to the time of enrollment
- clinically significant pleural effusion, lung abscess, or pneumatocele
- Hospitalization for pneumonia during Day -5 to -1 of antibiotic therapy for CAP
- Pneumonia due to S. aureus or group A streptococcus documented by positive blood culture or PCR at the time of enrollment
- History of pneumonia within the previous 6 months
- History of persistent asthma within the previous 6 months or current acute asthma exacerbation
- Provider-diagnosis of aspiration pneumonia, bronchiolitis, or bronchitis
- Surgery or other invasive procedures of the upper or lower airway (e.g., bronchoscopy, laryngoscopy) with general anesthesia or hospitalization </=7 days before diagnosis of CAP
- History of an underlying chronic medical condition
- History of a condition that compromises the immune system
- Any other condition that in the judgment of the investigator precludes participation because it could affect the safety of the subject
- Current enrollment in another clinical trial of an investigational agent
- Previous enrollment in this trial
Intervention:
-
Short course antibiotic strategy:
- 5 days of matching placebo
Control:
-
Standard course antibiotic strategy:
- 5 days of initially prescribed antibiotic (amoxicillin, amoxicillin and clavulanate, or cefdinir)
Outcomes:
Primary Outcome:
- Response Adjusted for Duration of Antibiotic Risk (RADAR) measured at the first outcome assessment visit (OAV1 on days 6–10)
- RADAR determined using 2 step process
-
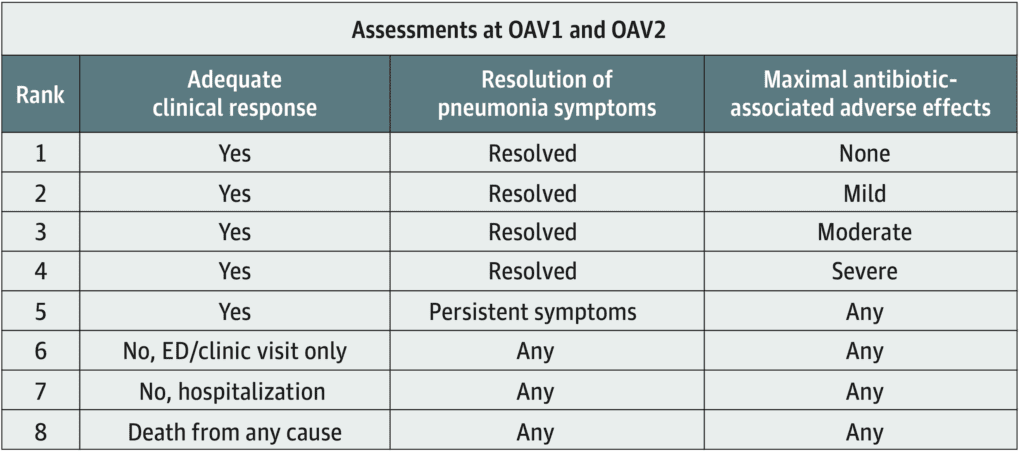
- Clinical Outcomes are categorized according to the desirability of outcome ranking (DOOR)
-
Ranked participants’ overall experiences
- When comparing different DOOR ranks, participants with more desirable DOOR received a higher rank.
- When comparing outcomes with the same DOOR rank, participants who took fewer total days of antibiotics received a higher rank.
Secondary Outcomes:
- RADAR at OAV2 (days 19–25)
- DOOR at OAV1 and OAV2
-
DOOR individual components at OAV1 and OAV2
- Adequate clinical response
- Resolution of symptoms
- Antibiotic-associated adverse effect
Results:
- 390 children assessed for eligibility
- 385 enrolled
- 5 additional patients were deemed ineligible after randomization but before day 1
-
192 randomized to short-course strategy
- 189 patients included in the intention-to-treat analysis
- 170 patients included in the complete-case cohort on OAV1
- 163 patients included in the complete-case cohort on OAV2
-
193 randomized to standard-course strategy
- 191 patients included in the intention-to-treat analysis
- 171 patients included in the complete-case cohort on OAV1
- 167 patients included in the complete-case cohort on OAV2
Primary Outcome Results:
-
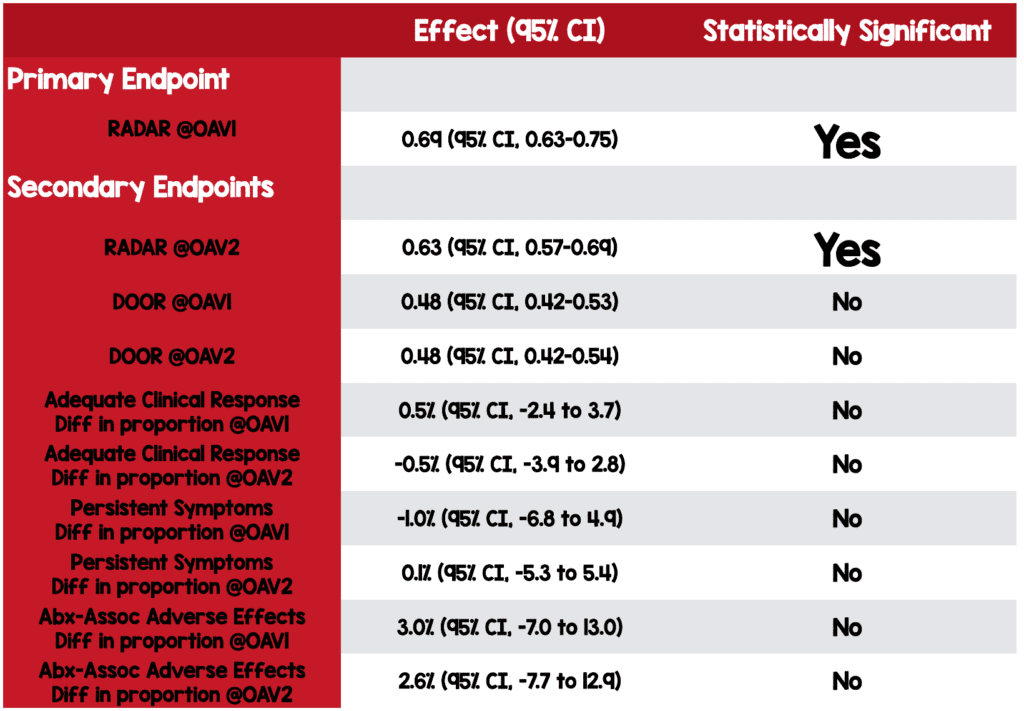
RADAR at OAV1: Clinically significant difference
- Estimated probability of a more desirable RADAR for the short-course strategy of 0.69 (95% CI, 0.63-0.75)
Secondary Outcome Results:
RADAR at OAV2: Clinically significant difference
- The probability of a more desirable RADAR in the short-course strategy was 0.63 (95% CI, 0.57-0.69)
DOOR at OAV1 and OAV2: No significant difference
- The probability of a more desirable DOOR for the short-course strategy was 0.48 (95% CI, 0.42-0.53) at OAV1
- The probability of a more desirable DOOR for the short-course strategy was 0.48 (95% CI, 0.42-0.54) at OAV2
Adequate Clinical Response at OAV1 and OAV2: No significant difference
- 1% vs <1%; difference in proportion, 0.5% (95% CI, −2.4 to 3.7) at OAV1
- 1% vs 2%; difference in proportion, −0.5% (95% CI, −3.9 to 2.8) at OAV2
Persistent Symptoms at OAV1 and OAV2: No significant difference
- The difference in proportion, −1.0% (95% CI, −6.8 to 4.9) at OAV1
- The difference in proportion, 0.1% (95% CI, −5.3 to 5.4) at OAV2
Antibiotic-Associated Adverse Effects at OAV1 and OAV2: No significant difference
- Difference in proportion 3.0% (95% CI, −7.0 to 13.0) at OAV1
- Most adverse effects were mild (e.g., irritability and diarrhea)
- 11% in both groups had moderate to severe adverse effects.
- The difference in proportion, 2.6% (95% CI, −7.7 to 12.9) at OAV2
- 36 (19%) children in both groups had moderate to severe adverse effects.
Strengths:
- Investigators asked a clinically relevant patient-centered question.
- Primary and secondary endpoints were complex but patient-oriented.
- The multicenter randomized, double-blind placebo-controlled study design increases generalizability to a broader population.
- The placebo and antibiotics were matched for taste and appearance, decreasing the potential for unblinding and bias.
- Investigators performed an intention-to-treat analysis.
-
Investigators performed a worse-case analysis and complete-case analysis for missing data.
- Worse-case is a variation of sensitivity analysis that evaluates the uncertainty in data by incorporating varying probability estimates for the endpoints in Question.
- Complete-case analysis evaluates only patients with complete data.
- Baseline Characteristics appear well-matched in both groups.
Limitations:
- The study was performed in a single country which may limit generalizability.
-
The studied population likely represents a convenience sample with selection bias
- Only 390 patients were assessed in 8 cities over 3 years.
- Or approximately 1 patient every 3 weeks per site
- This is a relatively small number of patients for a relatively common disease.
- There were many exclusion criteria, including asthma and any chronic underlying medical condition limiting generalizability to a more diverse population.
-
Caregivers recorded symptoms using a daily memory aid and diary.
- Increases the potential for measurement bias and recall bias.
- There is no information on diagnostic testing or radiographic imaging in either arm.
-
It appears the primary outcome was modified [Link is here].
- Initially registered with a primary endpoint of DOOR at OAV1
- Investigators do not define mild, moderate, and severe antibiotic-associated adverse effects.
-
Lots of patients with missing information which is essentially loss to follow up
- Patients should be analyzed as having met the worse possible outcome.
- However, this can be complicated when outcomes are not binary as those in this study.
- In the resistome substudy, the endpoint was a disease-oriented outcome.
Discussion:
Recent Evidence
- The SCOUT-CAP trial is the third positive, high-quality RCT in the last 12 months, investigating the duration of antibiotic therapy for pediatric CAP. Two other trials were noninferiority trials, while SCOUT-CAP was a superiority trial. The medical evidence is trending towards shorter courses of antibiotics for pediatric CAP. However, clinical guidelines are often slow to adapt to current evidence.
-
The SAFER Trial [Link is here]
- The per-protocol analysis of the short-course antibiotic arm crossed the noninferiority margin by a narrow margin. However, a potentially more clinically relevant secondary endpoint of “clinical cure not requiring additional intervention” was statistically noninferior to the standard-length arm.
-
The CAP-IT Trial [Link is here]
- Found low-dose antibiotic arm was noninferior to high dose, and a 3-day duration was noninferior to 7 days, concerning the need for further antibiotic retreatment.
RADAR and DOOR Explained:
-
DOOR: Desirability Of Outcome Ranking (see chart above)
- 8 class system ranks patients according to clinical response, resolution of symptoms, and antibiotic-associated adverse effects.
-
RADAR: Response Adjusted for Duration of Antibiotic Risk
- It was determined using a 2 step process that first compared the DOOR of participants. If two participants had the same rank, investigators next considered the total duration of antibiotics, granting a higher ranking to the patient with fewer total days of antibiotics.
- RADAR, the primary endpoint, is abstract and esoteric. In addition, the investigators arbitrarily decided that achieving a 60% probability of a more desirable RADAR for the short-course strategy would be clinically relevant. Moreover, the investigators changed the primary outcome from DOOR at OAV1 to RADAR after registering the trial. Authors should clearly state the reason for changing endpoints, so healthcare providers may fully understand any potential study limitations and biases.
Inside the Numbers:
- There was no difference between the short-course and standard-course treatment arms for DOOR or any individual component at OAV1 or OAV2. Superiority in the short-course strategy was driven by fewer total days of antibiotics taken, highlighting the importance of knowing if these children truly had bacterial pneumonia. If many children had viral pneumonia, investigators might falsely conclude that a shorter-course treatment strategy is superior to the standard course.
- Microbial stewardship principles recommend that antibiotic duration be kept to the minimum length to treat the infection effectively, thereby decreasing antibiotic exposure and limiting the potential for developing resistance. Additionally, the number of pathogens with antibiotic-resistant genes was significantly lower in the short-course strategy contradicting the dogmatic teaching that shorter courses of antibiotics could select for more resistant pathogens.
Diagnosing Community-Acquired Pneumonia:
- CAP is overdiagnosed, and many children will have viral pneumonia or possibly even another viral process. There was no standard definition or diagnostic criteria for CAP in this trial. Children with viral pneumonia will improve despite antibiotic therapy and not because of it. Therefore, It doesn’t matter if we prescribe five days or zero days of antibiotics—if it’s not bacterial CAP, antibiotic treatment is useless.
- Investigators provide no information on diagnostic testing or radiographic imaging in either arm. Testing is not required or routinely recommended for healthy children with CAP treated in an outpatient setting. In any case, the poor sensitivity of both laboratory diagnostics and radiographic imaging limits their routine utility. However, there may be variations in clinical practice, and it’s likely some practitioners ordered testing on enrolled patients. Imbalanced testing frequency or imbalanced test results (e.g., more patients with abnormal chest Xrays in one treatment arm) among the study groups could alter the trial findings.
Follow-Up:
- The studied cohort was a select group of healthy children who already demonstrated clinical improvement at enrollment (day 3–6 of antibiotics), underpinning the importance of close outpatient follow-up. When we see patients a second time in the emergency department, it’s often for treatment failure. Therefore, it’s critical to have a conversation with both parents and pediatricians and stress the importance of close follow-up when recommending short-course antibiotics.
Authors Conclusions: “A 5-day course of guideline-recommended antibiotics is a safe and effective approach for treating young children with uncomplicated outpatient CAP who demonstrate early clinical improvement. Implementation of this strategy is encouraged to optimize treatment efficacy, lessen unnecessary antibiotic use, and reduce the prevalence of antibiotic resistance genes among colonizing oropharyngeal flora.”
Clinical Bottom Line:
In this trial, investigators found shorter courses of antibiotics to be superior in treating healthy, clinically improving children diagnosed with uncomplicated CAP. The SAFER trial and CAP-IT trial found short courses of antibiotics to be noninferior to standard duration antibiotic treatment for pediatric CAP. Larger prospective international RCTs may still be needed before widespread adoption. But the pendulum is swinging, and the current evidence represents an opportunity for shared-decision making with parents.
References:
- Williams DJ, Creech CB, Walter EB, et al. Short- vs Standard-Course Outpatient Antibiotic Therapy for Community-Acquired Pneumonia in Children: The SCOUT-CAP Randomized Clinical Trial. JAMA Pediatr. 2022;e215547. PMID: 35040920
- Pernica JM, Harman S, Kam AJ, et al. Short-Course Antimicrobial Therapy for Pediatric Community-Acquired Pneumonia: The SAFER Randomized Clinical Trial. JAMA Pediatr. 2021;175(5):475-482. PMID: 33683325
- Bielicki JA, Stöhr W, Barratt S, et al. Effect of Amoxicillin Dose and Treatment Duration on the Need for Antibiotic Re-treatment in Children With Community-Acquired Pneumonia: The CAP-IT Randomized Clinical Trial [published correction appears in JAMA. 2021 Dec 7;326(21):2208]. JAMA. 2021;326(17):1713-1724. PMID: 34726708
For More on This Topic Checkout:
- REBEL EM: The CAP-IT Trial: Amoxicillin Dose and Duration in Children with Community-Acquired Pneumonia
- REBEL EM: The SAFER Trial: Pediatric CAP – Amoxicillin 5d vs 10d
- The SGEM: SGEM#338 – Are Children With CAP Safe and Sound if Treated for 5D Rather Than 10D of Antibiotics?
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter:@EMSwami) and Salim R. Rezaie, MD (Twitter:@srrezaie)
The post The SCOUT–CAP Trial: 5d Abx vs. 10d Abx in Pediatric CAP appeared first on REBEL EM - Emergency Medicine Blog.