
Background Information:
 Hypothermia was first introduced in 2002 by two studies, Bernard et al and The Hypothermia After Cardiac Arrest (HACA) trial.1,2 The latter, although a small trial, showed improved neurologic outcomes at six months when patients were cooled to 32-34oC. For a long time, a temperature of 33oC was the widely accepted standard of therapy for out-of-hospital cardiac arrest.1 In recent years, a trial aptly named the Targeted Temperature Management (TTM) Trial challenged this notion,3 finding that a temperature of 33oC did not confer any benefit over 36oC.4 Since then, not only has the overall benefit of the therapy remained in question, but many institutions were also left on their own to decide the most appropriate temperature to target. Fever has been proposed as a risk factor for unfavorable outcomes, but the available data only gives us association, not causation. The authors of the TTM trial have now come out with their subsequent study looking to assess the benefit of avoiding fever versus targeting a specific temperature in critically ill patients following cardiac arrest.
Hypothermia was first introduced in 2002 by two studies, Bernard et al and The Hypothermia After Cardiac Arrest (HACA) trial.1,2 The latter, although a small trial, showed improved neurologic outcomes at six months when patients were cooled to 32-34oC. For a long time, a temperature of 33oC was the widely accepted standard of therapy for out-of-hospital cardiac arrest.1 In recent years, a trial aptly named the Targeted Temperature Management (TTM) Trial challenged this notion,3 finding that a temperature of 33oC did not confer any benefit over 36oC.4 Since then, not only has the overall benefit of the therapy remained in question, but many institutions were also left on their own to decide the most appropriate temperature to target. Fever has been proposed as a risk factor for unfavorable outcomes, but the available data only gives us association, not causation. The authors of the TTM trial have now come out with their subsequent study looking to assess the benefit of avoiding fever versus targeting a specific temperature in critically ill patients following cardiac arrest.
Paper: Dankiewicz J et al. Hypothermia Versus Normothermia After Out-Of-Hospital Cardiac Arrest. NEJM 2021. PMID: 34133859
Clinical Question:
- Does targeted hypothermia lead to improved outcomes in comparison to targeted normothermia (and avoidance of fever) in patients with ROSC after OHCA?
What They Did:
- International, multicenter randomized superiority trial with co-enrollment along with the Targeted Therapeutic Mild Hypercapnia (TAME) trial.
- Patients were randomized in a 1:1 ratio into one of two groups for an intervention period of 40 hours:
- Hypothermia / Intervention group: Rapid target temperature of 33oC achieved through cold fluids and surface or intravascular cooling devices. This was maintained for 28 hours after randomization followed by hourly rewarming to 37oC in increments of ⅓ of a degree
- Normothermia / Control group: Temperature trigger of 37.8oC at which point patients received surface or intravascular cooling devices to aggressively maintain a temperature of 37.5oC. This was maintained for 72 hours after randomization in patients who remained sedated or comatose
- Due to inherent problems with blinding body temperature, clinicians were non-blinded however assessors of prognosis, participants, outcome assessors, statisticians and data managers were all blinded
- Two duplicate manuscripts were written for both scenarios before randomization was eventually revealed
- Outcomes were assessed at 30 days, 180 days and (an on-going) 24-months via face-to-face interview or telephone interview (due to limitations from the COVID19 Pandemic). Information was obtained by the patient and/or their healthcare proxy
- During these structured interviews, formally trained interviewers graded the patient’s outcomes using the modified Rankin Scale (Table 1)

Table 1: modified Rankin Scale
Inclusion Criteria:
- Adult patients over the age of 18 years old
- Out-of-hospital cardiac arrest of a presumed cardiac or unknown cause
- Unconscious and not able to obey verbal commands and no verbal response to pain
- Sustained (20-minutes) return of spontaneous circulation (ROSC) with signs of circulation without the need for chest compressions
- Eligible for intensive care without restrictions or limitations
- Inclusion within 180 minutes of ROSC
Exclusion Criteria:
- Unwitnessed cardiac arrest with an initial rhythm of asystole
- Temperature of <30oC upon admission
- Requiring Extracorporeal Membrane Oxygenation prior to ROSC
- Obvious or suspected pregnancy
- Intracranial bleeding
- Severe COPD requiring long-term home oxygen therapy
Outcomes:
Primary
- Death from any cause at 6 months
Secondary
- Any of the following adverse events
- Arrhythmia
- Bleeding
- Skin complications (from cooling devices)
- Pneumonia
- Sepsis
- Poor Functional outcome (defined as a modified Rankin Score of 4-6) at 6 months
- Number of days patient was alive and out of the hospital at 180 days
- Survival determined by Time-to-death analysis
- Health-related quality of life assessed via the European Quality of Life-5-Dimensional-5-Level Questionnaire (EQ-5D-5L)
Results:
Critical Results:
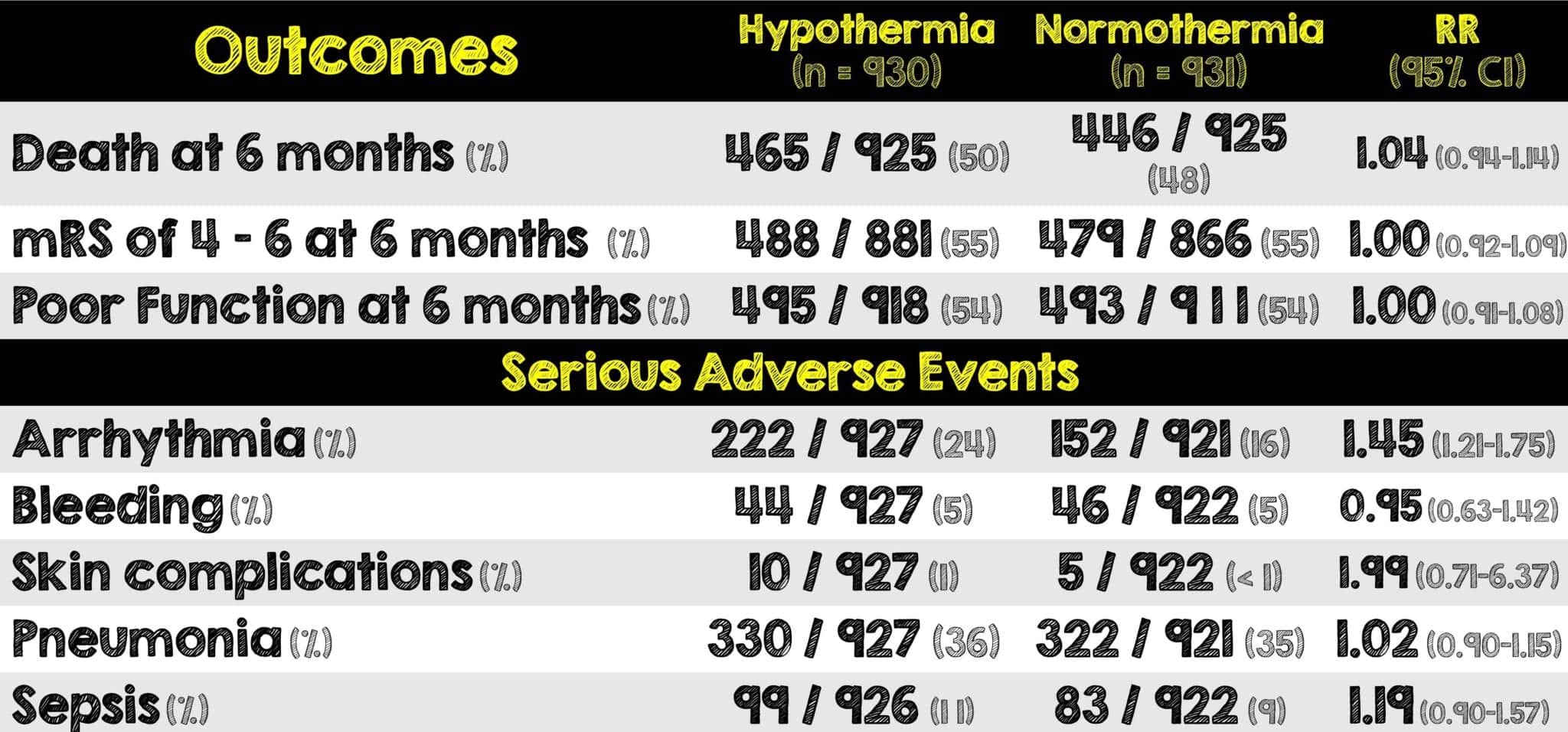
- The p-value for the primary outcome: death from any cause at 6-months was 0.37 (not statistically significant)
- The only secondary outcome to be statistically significant at <0.001 was arrhythmia causing hemodynamic compromise
- The hypothermia group required more paralytics and longer duration of mechanical ventilation than the normothermia group
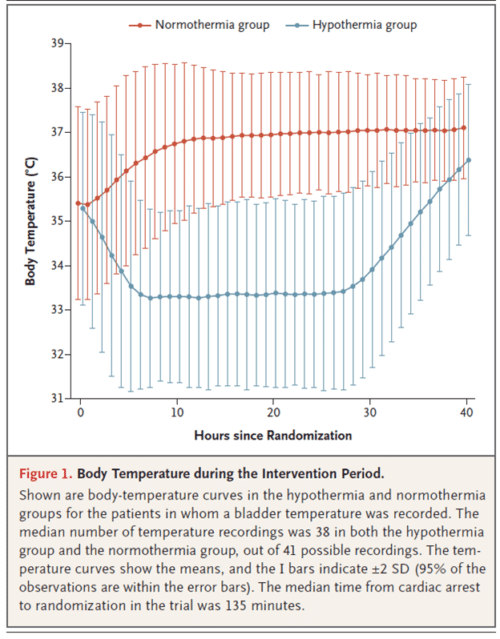
Figure 1: Body Temperature During the Intervention Period (Image from Paper)
Strengths:
- The methodology of this study was intricate, organized, and extremely well thought out
- There was a lack of benefit in functional outcomes which was consistent across all subgroups, adding to the validity of the results
- Clear separation in temperatures between the two groups
- Large sample size of patients leading to less chance of random error in the outcomes. This sample size was 5x bigger than combined enrollment of the earlier trials on this topic
- High external validity given the large sample size of patients across 61 varying institutions in 14 different countries
- Primary outcome was at low risk of bias and outcome assessors were unaware of the trial group assignments
- Both groups (intervention and control) were equally balanced
- A complete and thorough post-cardiac arrest intensive care bundle was applied to both groups thus minimizing practice variability
- Only had three deviations from the protocols just mentioned
- At 96 hours a physician unaware of intervention assignments performed a neurologic assessment of the patients who remained in the ICU
- Nearly complete follow-up with 94% of patients having outcomes assess via the mRS (a well-recognized, validated and frequently used, scoring system) and <1% missing for the primary outcome
Limitations:
- It is unclear whether the findings can be applied to patients with in-hospital cardiac arrests
- Although difficult to do any earlier, cooling in the hypothermia arm was achieved 3 hours after randomization
- Predominance of the patients in both groups were male
- Bundle of protocolized intensive post-cardiac arrest care is not representative of current clinical practice at all institutions (this includes approaches to sedation, paralysis and mechanical ventilation)
- Conservative protocol for neuro-prognostication and guidance for withdrawal of care may have influenced outcomes
- Very particular subset of patients enrolled (ie. Unwitnessed cardiac arrest with asystole and pregnant patients were excluded)
- 20% of patients were co-enrolled with the TAME study, unclear the impact of this until those study results are published
- There was no third group to answer the question as to whether temperature management is better than no temperature management
Discussion:
- This was an incredibly well-designed study and one that continues to add more to our knowledge of targeted temperature management for post-cardiac arrest patients. We must be careful broadly applying its results and consider the implications when translating clinical research into clinical practice.
- When the first TTM trial came out, hospitals quickly changed their target temperature to 36o Although much smaller and their methods less intricately designed, two trials in two different countries found higher odds of neurologically intact survival at 33oC. The worse outcomes may have been due to difficulty with compliance at achieving 36oC temperatures.3,4
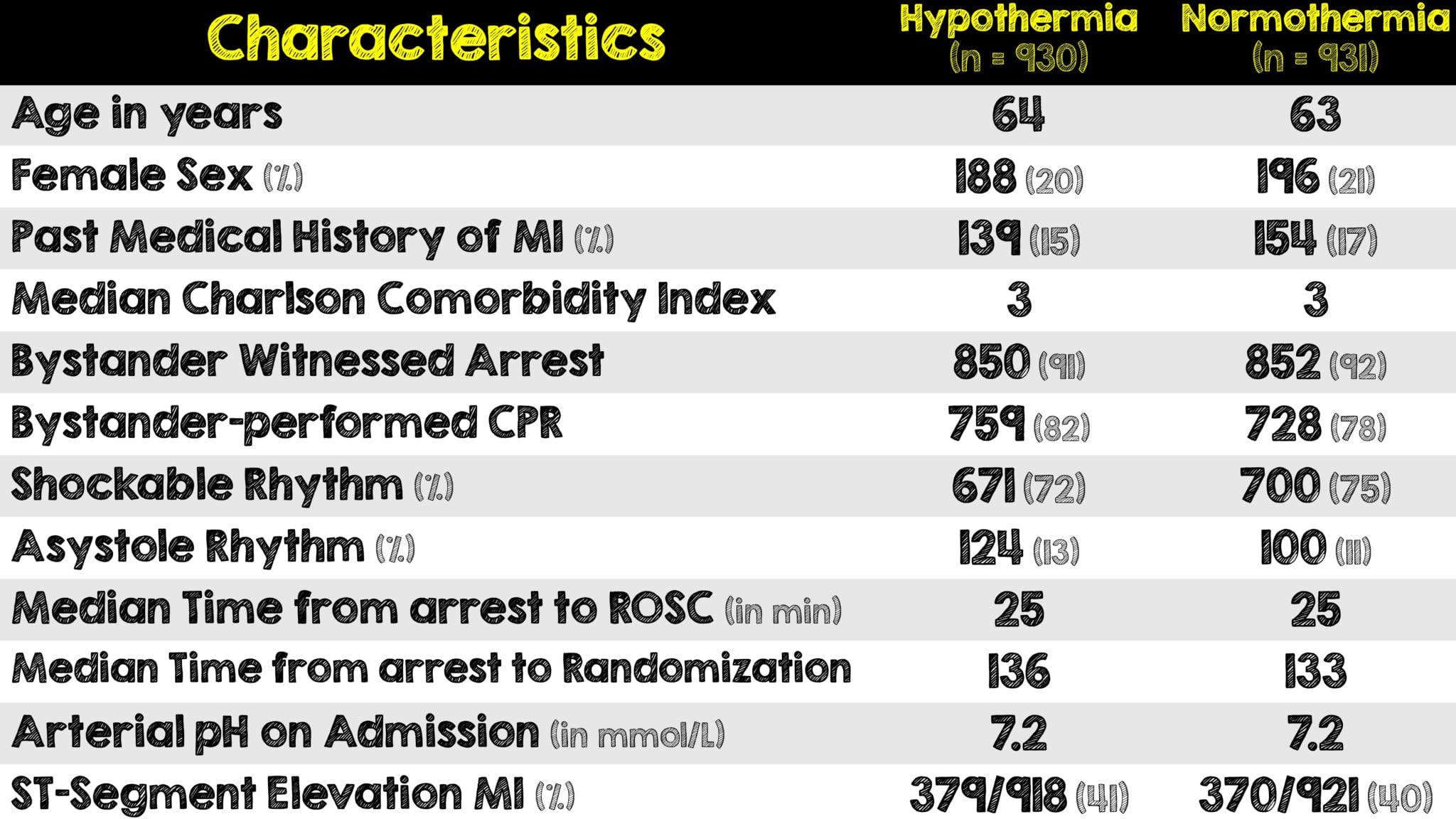
- Not only were patients with unwitnessed cardiac arrest excluded, over 90% of patients in both groups had bystander CPR performed, which is a rate not found anywhere in the United States. Additionally, a significantly large number of patients were found to have a STEMI. All these contribute to the notion that the patient population in this trial was unique
- Note that approximately half of the normothermia patients required a cooling device to avoid fever. Although not placed to maintain a targeted temperature, the role and benefit of these devices must be addressed in a separate study
- The survival of roughly half of these patients is remarkable and not seen in most if any hospitals in the United States. This is likely attested to the high bystander CPR rate or the post-arrest critical care bundle that they received while in the ICU. Additionally,unwitnessed cardiac arrest w/asystole was excluded thus further skewing the overall patient population.
- Regardless, this trial highlights the importance of having more robust CPR-training for bystanders, a well-developed pre-hospital care, consistent neuro-prognostication and a protocolized system for taking care of these post-arrest patients in the ICU
- This trial and its predecessor (the TTM) highlight the importance of minimizing premature withdrawal of life-sustaining therapy. An independent clinician blinded to the interventions performed neuro-prognostication according to pre-specified criteria to identify patients likely of a poor outcome. This practice should arguably be done in all clinical practices, outside of trials, to prevent premature closure in patients who could survive.5
- The time to cool is an aspect of this study that needs to be commented on. Operationally, it is extraordinarily difficult to achieve cooling to a targeted temperature within 3 hours as patients who present to the emergency department have to be stabilized, sent to a CT scanner and in this case then the cardiac cath lab. We know from many animal studies that earlier cooling has a more potential benefit,6 since prehospital hypothermia was not implemented in this trial, it still remains unclear if even earlier implementation of cooling may have had any benefit.
- On the topic of cooling and time, the duration of hypothermia also remains unknown. While there is currently a trial underway to answer this question, (ICECAP) the results likely won’t be available for several years.7
Author’s Conclusions:
- In patients with coma after out-of-hospital cardiac arrest, targeted hypothermia did not lead to a lower incidence of death by 6 months than targeted normothermia.
Our Conclusion:
- We agree with the author’s conclusion that cooling did not lead to improved outcomes. Targeted temperature management is a very resource heavy and expensive intervention that comes with many adverse events. The present trial, in addition to evidence from the prior TTM trial, is the highest level of evidence we have on this topic. Despite a different patient population, cooling has continued to show more harm than benefit. The role of targeted temperature management in post-cardiac arrest care is starting to shift more towards a greater vigilance on avoiding fever rather than keeping patients at a specific temperature. Additionally, more effort and focus should be directed at bystander CPR, early defibrillation, and well-designed post-cardiac arrest care bundles in the ICU.
Clinical Bottom Line:
- Targeted temperature management may still have a role in post-cardiac arrest therapy as a super aggressive approach to avoiding fever. With no benefit in survival and more harm with adverse events (ie. additional paralytics and prolonged duration of mechanical ventilation), cooling may not have as meaningful of an effect on clinical improvement as originally thought. Rather than doing less, this trial highlights the importance of doing MORE for these patients such as hypervigilance of fever avoidance, bystander CPR training, immediate defibrillation, percutaneous coronary intervention access, early and unbiased neuro-prognostication and well-designed post-cardiac arrest care bundles in the ICU to improve outcomes.
REFERENCES:
- Bernard SA, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002 Feb 21; PMID: 11856794
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002 Feb PMID: 11856793
- Morrison LJ, et. Translating Targeted Temperature Management Trials into Postarrest Care. N Engl J Med. 2021 Jun 17. PMID: 34133865
- Dankiewicz J et al. Hypothermia Versus Normothermia After Out-Of-Hospital Cardiac Arrest. NEJM 2021. PMID: 34133859
- Nielsen N, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. Dec 2013. PMID: 24237006
- Johnson NJ, et al. Targeted Temperature Management at 33 Versus 36 Degrees: A Retrospective Cohort Study. Crit Care Med. Mar 2020. PMID: 31809279
- Bray JE, et al. Changing target temperature from 33°C to 36°C in the ICU management of out-of-hospital cardiac arrest: A before and after study. Resuscitation. Apr 2017 PMID: 28159575
- Scales DC, et al. Improving appropriate neurologic prognostication after cardiac arrest: a stepped wedge cluster randomized controlled trial. Am J Respir Crit Care Med 2016; PMID: 27115286
- Olai H, et al. Meta-analysis of targeted temperature management in animal models of cardiac arrest. Intensive Care Med Exp 2020; PMID: 31953652
- More details regarding the ICECAP Trial can be found here
For More Thoughts on This Topic Checkout:
- First10 in EM: The Big Chill on Therapeutic Hypothermia
- PulmCrit: A History of Hypothermia for Cardiac Arrest, 2002-2021 (RIP)
- The Bottom Line: TTM2
- The SGEM: SGEM#336 – You Can’t Always Get What You Want – TTM2 Trial
- St. Emlyn’s Blog: The TTM2 Trial. Normothermia or Hypothermia Post Cardiac Arrest
Post Peer Reviewed By: Salim Rezaie, MD (Twitter: @Srrezaie) and Ananad Swaminathan, MD (@EMSwami)
The post TTM2: Hypothermia vs Normothermia for Out-of-Hospital Cardiac Arrest appeared first on REBEL EM - Emergency Medicine Blog.