
 D-dimer testing is sensitive for thrombus formation, and in patients who are not high risk, this test is used to rule-out venous thromboembolism. D-dimer has been shown to increase with age, which can cause a lower specificity (i.e. more false positive tests) in older patients. Specificity can range from 49 – 67% in patients ≤ 50 years of age, but in older patients (i.e. ≥ 80 years of age) the specificity is quoted as 0 – 18%. The result of this is, older patients often have more diagnostic imaging, but a higher cut-off may lead to increased false negative cases (i.e. missed VTE) and make this strategy less safe. So could age adjusted d-dimer testing increase specificity without affecting sensitivity?
D-dimer testing is sensitive for thrombus formation, and in patients who are not high risk, this test is used to rule-out venous thromboembolism. D-dimer has been shown to increase with age, which can cause a lower specificity (i.e. more false positive tests) in older patients. Specificity can range from 49 – 67% in patients ≤ 50 years of age, but in older patients (i.e. ≥ 80 years of age) the specificity is quoted as 0 – 18%. The result of this is, older patients often have more diagnostic imaging, but a higher cut-off may lead to increased false negative cases (i.e. missed VTE) and make this strategy less safe. So could age adjusted d-dimer testing increase specificity without affecting sensitivity?
It is important to know what type of d-dimer assay you have at your institution and make sure that it correlates to the studies below. Broadly, d-dimer testing can be described as quantitative tests (i.e. results expressed as a number), semi-quantitative, or qualitative (i.e. results expressed as positive or negative). More specifically there are 5 major types of d-dimer assays:
-
 Enzyme-Linked Immuosorbent Assay (ELISA)
Enzyme-Linked Immuosorbent Assay (ELISA) - Latex Agglutination Assay
- Whole Blood assay (Simplired)
- Turbidimetric Assay
- Immunofiltration Assay
A nice review of some of the newer d-dimer tests can be found by Schutgens RE et al from 2003. Realize for the purpose of this post, we are specifically discussing quantitative d-dimer tests.
How do you perform age adjusted d-dimer testing?
- The formula is: Age (years) x 10 ug/L for patients > 50 years of age
- Example: Patient age 88 = age adjusted d-dimer of 880 ug/L
Where was age adjusted d-dimer testing derived and validated?
-
PE Derivation: [1]
- Conclusion: Age adjusted d-dimer combined with clinical probability, greatly increased the proportion of older patients in whom PE could be safely excluded
-
PE Validation: [2]
- Conclusion: Age-adjusted cut-off increased clinical usefulness of D-dimer in older patients
-
PE Validation: [3]
- Conclusion: Irrespective of which clinical decision rule is used, age-adjusted d-dimer increases the number of patients > 50 years in whom PE can be safely excluded.
-
DVT Validation: [4]
- Conclusion: Combination of low clinical probability of DVT, use of age dependent d-dimer cut-off value for patients > 50 years, DVT can be safely excluded, compared with the conventional cut-off value of 500 μg/L
-
DVT Validation: [5]
- Conclusion: Age-adjusted d-dimer in combination with clinical probability greatly increases the proportion of older patients in whom DVT can be safely excluded
Summary of Studies: Age adjusted d-dimer testing appears to increase specificity in patients age >50 years, without affecting sensitivity
There has also been a systematic review [6] that looked to review the diagnostic accuracy of d-dimer testing in older patients (> 50 years) with suspected venous thromboembolism comparing conventional d-dimer testing with age adjusted d-dimer testing.
What they did:
- Systematic review and meta-analysis
- 12, 497 patients with non-high clinical probability for venous thromboembolism included
- Comparison of conventional d-dimer vs age adjusted d-dimer
Results:
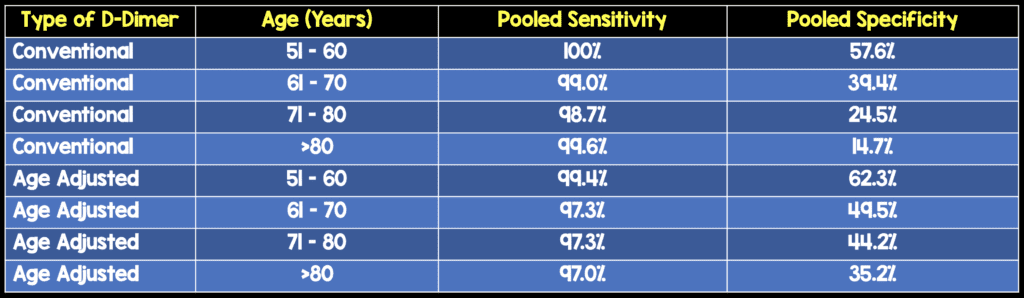
Conclusion: Age adjusted d-dimer testing increases specificity without modifying sensitivity in patients > 50 years of age.
What is the newest study to evaluate age adjusted d-dimer testing? [7]
 The ADJUST-PE Study
The ADJUST-PE Study
What they did:
- Multicenter, prospective validation of diagnostic yield of age-adjusted d-dimer cutoffs
- 19 centers in Belgium, France, the Netherlands, and Switzerland
- 3346 Consecutive patients presenting to ED with clinically suspected PE
- Applied either a revised Geneva score or a 2-level Wells score for PE followed by a high-sensitivity D-Dimer in non-high risk patients
Outcomes:
- Failure rate of diagnostic strategy (i.e. Thromboembolic events during 3 month follow up)
Results:
- Prevalence of PE was 19% (Higher than North American studies)
- 2898 patients had a low or unlikely clinical probability of PE
- 3 month failure rate in patients with a d-dimer level < 500ug/L was 1/810 patients (0.1%)
- 3 month failure rate in patients with a d-dimer level > 500 ug/L but below age-adjusted cutoff was 1/331 patients (0.3%)
- 3 month failure rate in patients with a d-dimer level > age-adjusted cutoff was 7/1481 (0.5%)
- In patients > 75 years with age-adjusted d-dimer level vs a 500 ug/L conventional cutoff, PE exclusion went from 6.4% to 29.7%, without additional false negatives…this is a 5-fold increase.
- 1 in 16 would have PE ruled out with a conventional d-dimer cutoff, but 1 in 3.4 would have PE ruled out with age-adjusted d-dimer cutoffs, with no increase in missed VTE
Limitations:
- 2 different pretest probability scores and 6 different d-dimer assays were used…cutoffs for different d-dimer assays vary from 200 – 500 ug/L
- Not a randomized clinical control study, so there was no control group
- 7 patients were deceased in the > 500 ug/L and < age adjusted cutoff d-dimer, but only one had an autopsy to confirm diagnosis, therefore hard to exclude PE as the cause of death
- Prevalence of PE was higher than what is cited in most North American studies, but the same rate as European studies
- Patient follow up was not with the gold standard CTPA
Conclusion: Compared to a fixed d-dimer cutoff of 500 ug/L, the combination of pretest probability assessment with age-adjusted D-dimer is associated with a larger number of patients in whom PE can be ruled out, without a decrease in missed PE
Take Home Message
In patients > 50 years of age, using a clinical probability assessment plus an age adjusted d-dimer cutoff increases the number of patients that can be safely ruled out for PE/DVT. It is important to note that different hospitals will use different assays of d-dimer and so the age adjusted cutoff used in the above studies may not be the same as your institution.
References:
- Douma RA et al. Potential of an Age Adjusted D-Dimer Cut-Off Value to Improve the Exclusion of Pulmonary Embolism in Older patients: A Retrospective Analysis of three Large Cohorts. BMJ 2010. PMID: 20354012
- Penaloza A et al. Performance of Age-Adjusted D-Dimer Cut-Off to Rule Out Pulmonary Embolism. J Thrombi Haemostasis 2012. PMID: 22568451
- van Es J et al. The Combination of Four Different clinical Decision rules and an Age-Adjusted D-Dimer Cut-Off Increases the Number of Patients in Whom Acute Pulmonary Embolism Can Safely be Excluded. Thromb Haemostasis 2012. PMID: 22072293
- Schouten HJ et al. Validation of Two Age Dependent D-Dimer Cut-Off Values for Exclusion of Deep Vein Thrombosis in Suspected Elderly Patients in Primary Care: Retrospective, Cross Sectional, Diagnostic Analysis. BMJ 2012. PMID: 22674922
- Douma RA et al. using Age-Dependent D-Dimer Cut-Off Value Increases the Number of Older Patients in Whom Deep Vein Trhombosis can be Safely Excluded. Haematologica 2012. PMID: 22511491
- Schouten HJ et al. Diagnostic Accuracy of Conventional or Age Adjusted D-Dimer Cut-Off Values in Older Patients with Suspected venous thromboembolism: Systematic Review and Meta-Analysis. BMJ 2013. PMID: 23645857
- Righini M et al. Age-Adjusted D-Dimer cutoff Levels to Rule out Pulmonary Embolism: The ADJUST-PE Study. JAMA 2014. PMID: 24643601
Other people have also written about age adjusted d-dimer cutoffs, and for their thoughts checkout:
- Emergency Medicine Literature of Note by Ryan Radecki
- Emergency Medicine Ireland by Andy Neill
- CanadiEM by Brent Thomas
The post Age Adjusted D-Dimer Testing appeared first on REBEL EM - Emergency Medicine Blog.